

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Rheumatoid arthritis (RA) is a type of chronic inflammatory arthritis that results in joint destruction and is associated with progressive disability.1 It is important that treatment is initiated as soon as possible, and that disease activity is strictly controlled to ensure successful inflammation suppression as assessed by validated compound disease activity measures.2 In addition, new global classification criteria, remission criteria, and a treat-to-target (T2T) strategy have been proposed for RA.
The primary target for the treatment of RA should be a state of clinical remission.34 Abrogation of inflammation is the most important way to achieve this goal. This is because the inflammatory response underlying RA is responsible for the signs and symptoms of the disease and is associated with adverse outcomes such as structural damage.5 However, several clinical remission criteria have not always equated to the complete absence of true inflammation.6 Several studies have shown that the progression of radiographic joint damage may occur in clinical remission regardless of the choice of remission definition. Ongoing subclinical inflammation detected by ultrasonography may explain this discrepancy.78
Power Doppler ultrasonography (PDUS) has been demonstrated to detect inflammation in the synovial tissue, and assess the disease activity of RA.91011 Ultrasound (US) has also been shown to predict relapses in patients with RA who have attained clinical remission.121314 However, there are few published studies to our knowledge that have investigated the predictors of imaging remission achievement using ultrasonography among patients with RA that have attained clinical remission. Moreover, no study has identified the rate of imaging remission among RA patients in Korea. Therefore, by evaluating residual inflammation with PDUS in patients with RA who have attained clinical remission, we hypothesized that, while the majority of patients may have attained clinical remission, they have not attained imaging remission. Additionally, we discuss the characteristics of patients who have attained imaging remission. Such details may be useful for informing the proper management of patients with RA.
Go to : 
METHODS
Patients and study design
Ninety-seven adult (> 18 years of age) patients with RA who met the clinical remission criteria defined as DAS28-ESR < 2.615 were enrolled in this study, which was conducted at the rheumatology clinic of Kyung Hee University Hospital. We selected patients with RA who had attained clinical remission for more than 6 months. Demographic data such as age, sex, comorbidities and current medications were collected. Clinical and physical measures were also collected, including tender joint count (TJC), swollen joint count (SJC), patient's general assessment (PGA), evaluator global assessment (EGA), and the health assessment questionnaire (HAQ) score. Laboratory tests including, the erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), rheumatoid factor (RF), anti-cyclic citrullinated peptide (anti-CCP) were recorded. The clinical disease activity index (CDAI) and simplified clinical disease activity index (SDAI) scores were calculated for each patient.16 Additionally, we evaluated the American College of Rheumatology/EUropean League Against Rheumatism (ACR/EULAR) Boolean remission criteria, based on 28. The definitions of clinical remission were; 1) CDAI ≤ 2.8,17 2) SDAI ≤ 3.3,17 3) ACR/EULAR Boolean criteria: a patient must satisfy all of the following, TJC ≤ 1, SJC ≤ 1, CRP ≤ 1 mg/dL, and PGA ≤ 1 (on a 0–10 scale).18
Ultrasonography assessments
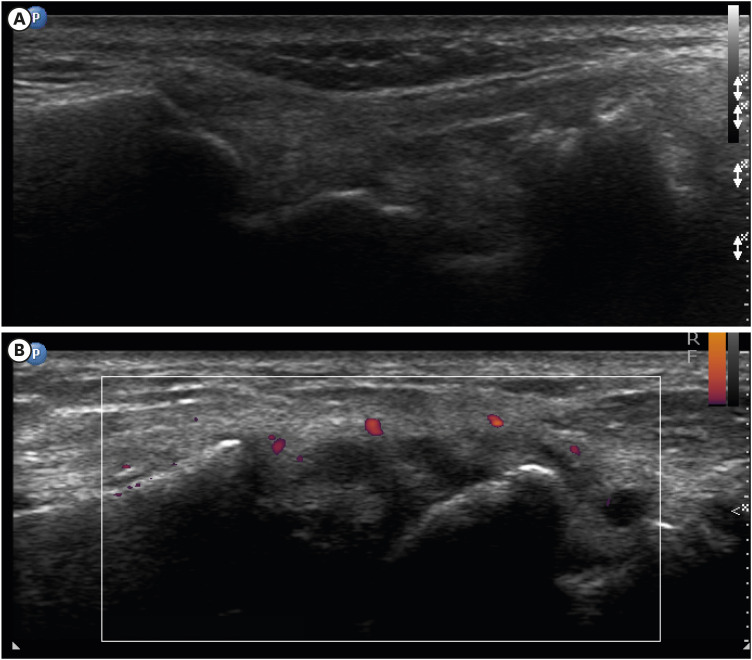
A US was performed by a single experienced sonographer on 16 joints and 2 tendons using the published USRA9 definitions.19 This included the metacarpophalangeal (MCP) 1–3, proximal interphalangeal (PIP) 2–3, radiocarpal (RC), metatarsophalangeal 2–3, and extensor carpi ulnaris tendon bilaterally. There were no changes in the US settings during the study and no software upgrades. The Phillips with a 5.0 to 12.0 MHz linear probe was used, and the power Doppler (PD) parameters were: Doppler frequency, 6.7 MHz; wall filter, 42 Hz; and gain, 74%. PDUS were graded based on a dichotomous assessment (presence/absence) and a semi-quantitative score that ranged from 0 to 3. The PDUS total scores ranged from 0–48. Imaging remission was defined as the absence of synovial hypertrophy and PD signals in all assessed joints (Fig. 1). The US exam was performed the same day as the clinical examination by an expert clinician who was blinded to the clinical data.
Statistical analysis
The χ2 and Fisher exact tests were used to compare the categorical data. Data were examined to determine whether they were normally distributed with the Kolmogorov-Smirnov test. Comparisons of continuous values were determined using the Mann-Whitney test. A univariable logistic regression was conducted to investigate factors associated with the imaging outcomes. A multivariable logistic regression analysis was also performed using the baseline variables that had demonstrated statistical significance (P < 0.05) on the univariable analysis. All statistical calculations were performed with SPSS version 22 (SPSS Inc., Chicago, IL, USA).
Ethics statement
This study was approved by the Institutional Review Board (IRB) of Kyung Hee Medical Center, and the requirement for informed consent was waived (IRB No. 2020-04-038).
Go to :
RESULTS
Patient characteristics
As shown in Table 1, of the 97 patients enrolled, 82 (84.5%) were female. The mean (standard deviation) age was 58.97 (± 11.90) years old. Seventy-eight (80.4%) patients were RF positive, and 82 (92.1%) patients were anti-CCP positive. Twenty (20.6%) patients were treated with biologics.
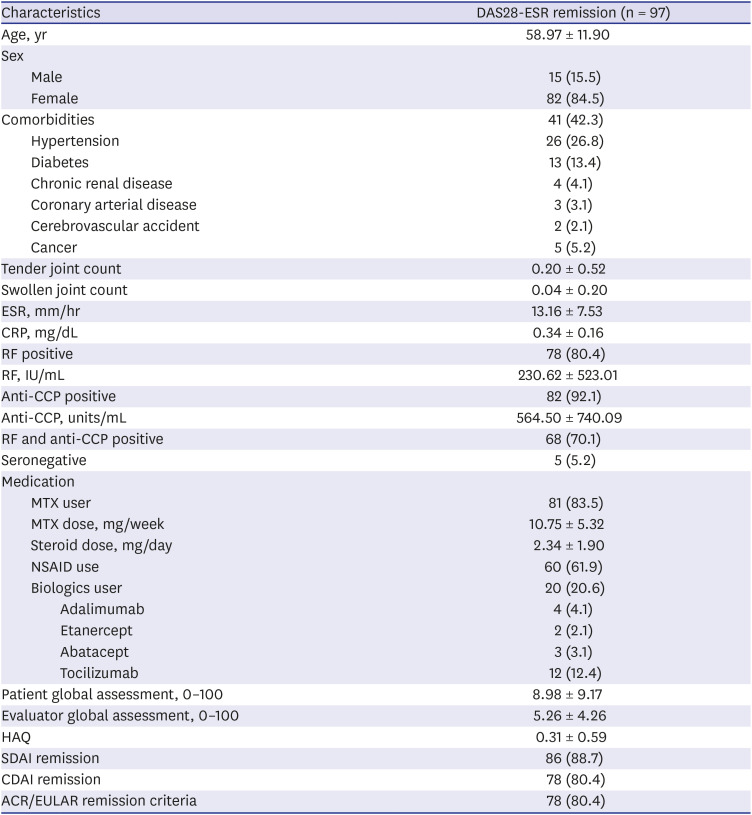
Table 1
Clinical and demographic characteristics of enrolled patients
Data are presented as mean ± standard deviation or number (%).
ESR = erythrocyte sedimentation rate, CRP = C-reactive protein, RF = rheumatoid factor, anti-CCP = anti-cyclic citrullinated peptide, MTX = methotrexate, NSAID = non-steroidal anti-inflammatory drugs, HAQ = health assessment questionnaire, SDAI = simple disease activity index, CDAI = clinical disease activity index; ACR/EULAR = American College of Rheumatology/EUropean League Against Rheumatism.
![]()
US findings
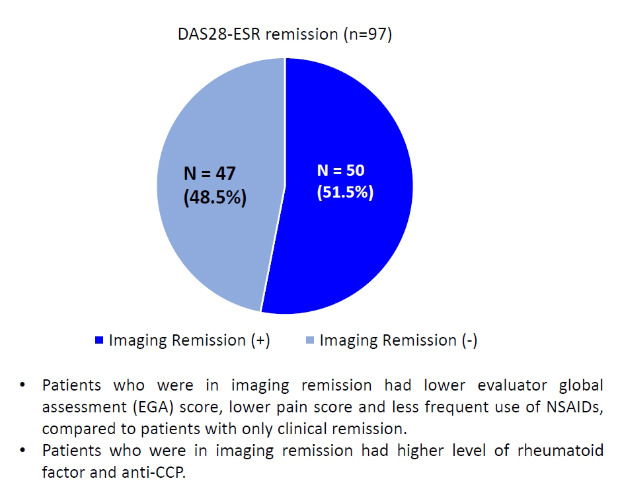
The achievement rate of imaging remission was 51.5% (50/97) among patients with RA that had attained clinical remission defined as DAS28-ESR < 2.6. Forty-seven patients (48.5%) were PDUS positive. PD was detected most frequently in the right RC joint (n = 40, 41.2%). Eleven patients complained of pain in other joints that were not included in the US assessment core set. Ten of these 11 patients (91%, 10 of 11), were PDUS positive at the additional joint that was painful. The achievement rates of imaging remission in terms of the other clinical remission criteria were 55.8% for SDAI (48/86), 57.7% for CDAI (45/78), and 55.1% for ACR/EURLAR Boolean remission criteria (43/78).
Clinical features of patients who achieved imaging remission
Table 2 shows the differences in the clinical features of those that attained and did not attain imaging remission. The patients who reached imaging remission, as well as clinical remission, had lower EGA scores (P < 0.001, 95% confidence interval [CI], −5.60, −2.27), and clinical disease activity scores, including the SDAI and CDAI (P = 0.025, 95% CI, −1.47, −0.33; P = 0.002, 95% CI, −1.47, −0.33, respectively). Patients who did not reach imaging remission tended to have higher active joint counts, patient global assessments, and HAQ scores. However, these were not statistically significant. The imaging remission group had higher RF levels. Patients who had not attained imaging remission tended to use more non-steroidal anti-inflammatory drugs (NSAID). The imaging remission achievement rates of subgroups divided by key clinical characteristics were analyzed. The seropositive group achieved higher levels of imaging remission than the seronegative group (1/5, 20.0%). The imaging remission achievement rate of the seropositive group was 52.7% (49/93). The imaging remission achievement rate of those, that were positive for RF and anti-CCP was, 59.4% (41/69). The imaging remission achievement rate of patients that used conventional synthetic disease-modifying antirheumatic drugs was 50.0%, and biologics was 52.4% (Table 3).
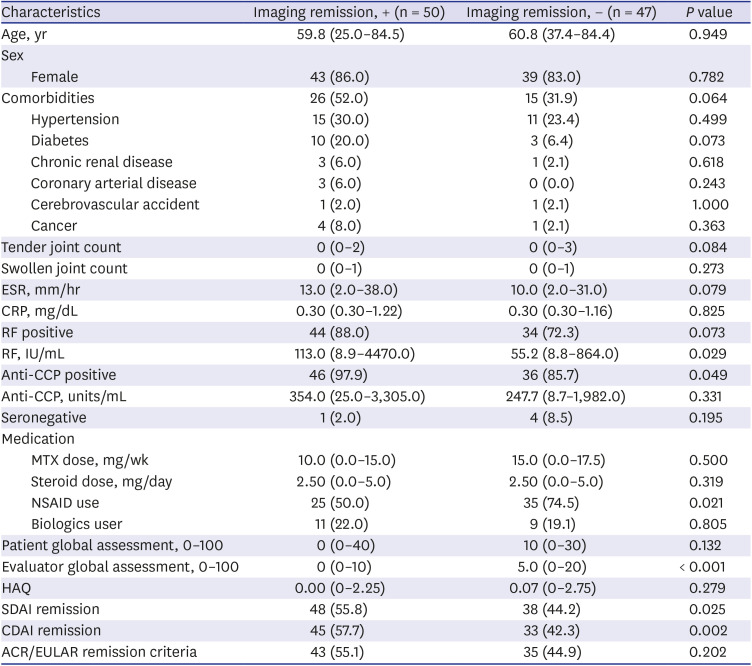
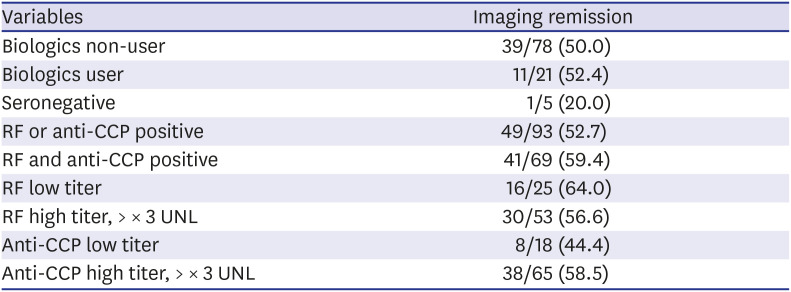
Table 2
Comparison of demographic and clinical characteristics of patients with rheumatoid arthritis that had or had not attained imaging remission
Data are presented as median (range) or number (%).
ESR = erythrocyte sedimentation rate, CRP = C-reactive protein, RF = rheumatoid factor, anti-CCP = anti-cyclic citrullinated peptide, MTX = methotrexate, NSAID = non-steroidal anti-inflammatory drugs, HAQ = health assessment questionnaire, SDAI = simple disease activity index, CDAI = clinical disease activity index, ACR/EULAR = American College of Rheumatology/EUropean League Against Rheumatism.
![]()
Table 3
Subgroup analysis of the imaging remission achievement rate
Data are presented as number (%).
RF = rheumatoid factor, anti-CCP = anti-cyclic citrullinated peptide.
![]()
Predictors of imaging remission
The results of the multivariable analysis, which used the baseline variables demonstrating statistical significance (P < 0.05) on univariable analysis, are shown in Table 4. Only the EGA score was identified as a significant predictor (P < 0.001) for the achievement of imaging remission in patients who had attained clinical remission.
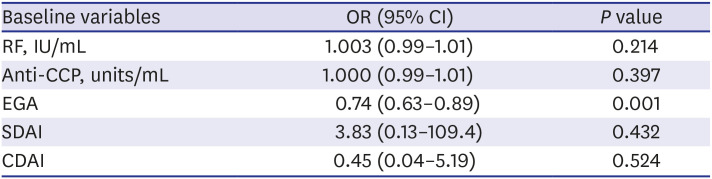
Table 4
Multivariable analysis of the baseline variables that could be predictive of imaging remission achievement
| Baseline variables | OR (95% CI) | P value |
|---|---|---|
| RF, IU/mL | 1.003 (0.99–1.01) | 0.214 |
| Anti-CCP, units/mL | 1.000 (0.99–1.01) | 0.397 |
| EGA | 0.74 (0.63–0.89) | 0.001 |
| SDAI | 3.83 (0.13–109.4) | 0.432 |
| CDAI | 0.45 (0.04–5.19) | 0.524 |
The model included RF (IU/mL), anti-CCP (units/mL), non-steroidal anti-inflammatory drugs use, patient global assessment, EGA, health assessment questionnaire, SDAI score, and CDAI score.
OR = odds ratio, CI = confidence interval, RF = rheumatoid factor, anti-CCP = anti-cyclic citrullinated peptide, EGA = evaluator global assessment, SDAI = simple disease activity index, CDAI = clinical disease activity index.
![]()
Go to :
DISCUSSION
In this study, 48.5% of the patients with RA that had attained clinical remission as per the DAS28-ESR had positive Doppler signals. The results were similar when other remission criteria were applied (SDAI, 44.2%; CDAI, 42.3%; ACR/EULAR Boolean remission criteria, 44.9%). It is expected that the imaging remission rate is the highest when the ACR/EULAR Boolean remission criteria are applied, which is the strictest criteria. However, in this study, the highest was founded when the CDAI was applied. However, the imaging remission achievement rate was less than 60% regardless of which criteria was used. The discordance between clinical and imaging remission observed in our study is consistent with previous studies. In patients with early RA that achieved DAS44 remission, the persistence of any PD was identified in 42% of 48 patients among 10 joints (the wrists, second and third MCPs and PIPs),12 and 41% of 43 patients that underwent a 44 joint US assessment.21 These results help to explain why there is a high probability of relapse when medication is reduced or discontinued even if a patient attained clinical remission.
PDUS can detect subclinical synovitis. PDUS can be used to detect increased microvascular blood flow, which is a sign of active synovitis.20 Several previous studies have reported the usefulness of PDUS. In a study by Brown et al.,21 102 patients in clinical remission were assessed with various imaging modalities. Despite being in clinical remission, 19% of patients deteriorated radiographically, and this progression was primarily explained by the PDUS signal. In other reports, it was found that a persistent PD signal over time had prognostic value for the development of radiographic articular damage in patients with RA.2223 As mentioned, US detected synovitis could be used to predict a radiographic progression in RA. Several prospective studies, the ARCTIC study24 and TaSER study,25 have investigated whether the intensive early RA T2T strategy could be improved by using a musculoskeletal US assessment of disease activity. Contrary to expectation in these 2 studies, the US-driven T2T strategy was not associated with significantly better clinical or imaging outcomes than a DAS28-driven strategy. However, both studies have some limitations in that they enrolled only patients with early RA, and the PD cut off values were too strict at ≤ 0. In a study by Scirè et al.,26 106 early RA patients that had attained clinical remission were followed for 24 months. They found that a positive PDUS signal, even in a single joint, was a predictor of disease relapse.21 US-detected subclinical synovitis may have a role in guiding dose tapering or withdrawal when applied to clinical practice. US offers an exciting extension to the management of patients with RA.
Our study has several limitations. First, due to the retrospective nature of the study design, it is impossible to demonstrate a causal relationship between variables. Second, there could be some selection bias. Because, of patients who attained clinical remission, only those who received an US were enrolled in this analysis. Nevertheless, a strength of our study is that the sample size was larger than previous studies. There have been few studies that have focused on the indicators of imaging remission. In this study, a low EGA score was found to be a predictor of imaging remission. Besides, RF levels and anti-CCP positivity correlated with imaging remission. Patients who did not attain imaging remission tended to have a higher count of tender and swollen joints, and a higher patient global assessment score. These patients also used more NSAIDs. In 2016, Horton et al.27 reported that a lack of osteoarthritis and objective signs of less severe disease (RF and anti-CCP negativity, fewer clinically swollen joints and lower CRP and baseline PD) were associated with more favorable imaging outcomes. So far, each study has shown different outcomes for the predictors. Further prospective studies are needed to examine about these discrepancies.
In conclusion, just over half of the patients achieved both DAS28-ESR remission and the absence of PD. A low EGA score can predict the achievement of imaging remission. Therefore, physicians should carefully evaluate patients who have attained clinical remission, particularly when considering whether to reduce or withdraw a specific therapy.
Go to :
 XML Download
XML Download