

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Helicobacter pylori is a risk factor of peptic ulcer, atrophic gastritis, and gastric carcinoma.1 Environmental, host-related, and virulent factors associated with the bacterium, including cytotoxin-associated gene A (CagA), vacuolating cytotoxin A (VacA), and outer inflammatory protein (OipA) are involved in the development of H. pylori-related diseases.2 Of these factors, CagA protein is associated with a severe clinical outcome. Most strains of H. pylori isolated in East Asia, including Korea, have been confirmed CagA-positive.345
It is thought that approximately half of the world's population harbors H. pylor
6 and H. pylori-related diseases represent a significant medical burden.78 Although the prevalence of H. pylori infection in developed countries has declined over recent decades, infection rate in the rest of the world remains high.6910 In Korea, H. pylori infection of late adolescents and adults has decreased due to rapid socio-economic growth and improved housing.111213 However, the previous studies had been designed to diagnose H. pylori infection using enzyme linked immunosorbent assay (ELISA), some of which used crude antigens of H. pylori isolated outside Korea and had enrolled populations aged 16 years and older due to the limitations of its use in diagnosing H. pylori infection in children.1112131415
H. pylori infection can take hold during infancy or early childhood and colonization generally persists for life if left untreated.161718
H. pylori induces systemic and mucosal immune responses in most infected patients. Serologic tests can detect H. pylori infection, and serum immunoglobulin (Ig) G, A, and M antibodies may indicate whether infection is acute or chronic.1920
H. pylori CagA antigen might be one of the major antigens that produce the strongest antibody responses and might be related to high levels of anti-H. pylori antibodies in infected humans.21 The patients remain positive for anti-CagA antibodies longer than other anti-H. pylori antibodies even after eradication of H. pylori.322
Jinju is a city of around 340,000 inhabitants that lies in the southern part of Korea and is surrounded by rural areas. Compared with other cities in Korea, the inflow and outflow of citizens are relatively low (www.index.go.kr). The relatively low migration rate (0.1% during 2006–2016) makes Jinju suitable for evaluating the lifetime trend of H. pylori infection, together with birth cohort effects. Few reports have examined the prevalence of H. pylori infection in the general population, including infants and children, along with lifetime trends.23 Thus the aim of the present study was to investigate changes in the seroprevalence of CagA positive H. pylori infection over the last 20 years in the general population of Jinju, ranging from neonates to the elderly. In addition, the lifetime trend of H. pylori infection was estimated by western blot analysis of IgG, IgA, and IgM antibodies against H. pylori CagA.
Go to : 
METHODS
Study population
Three retrospective cross-sectional analyses using collected serum samples were conducted concurrently. These cross-sectional analyses covered 1994–1995, 2004–2005, and 2014–2015, respectively, spanning a total of 20 years. A total of 1,305 serum samples matched with age, sex and collection period were obtained from the Gyeongsang National University Hospital (GNUH) Biobank, a member of the Korea Biobank Network and analyzed. All of the serum samples were preserved in the deep freezer before analysis. To evaluate the age when acute or initial H. pylori infection occurs, and to differentiate serologic positivity due to infection from that due to transplacental transmission of anti-H. pylori CagA IgG antibodies during infancy and early childhood, samples were grouped according to age as follows: neonate, 1–6 months, 7–12 months, 13–24 months, 2–4 years, and 5–9 years (infants and children), and 5 to10-year intervals thereafter (Table 1).
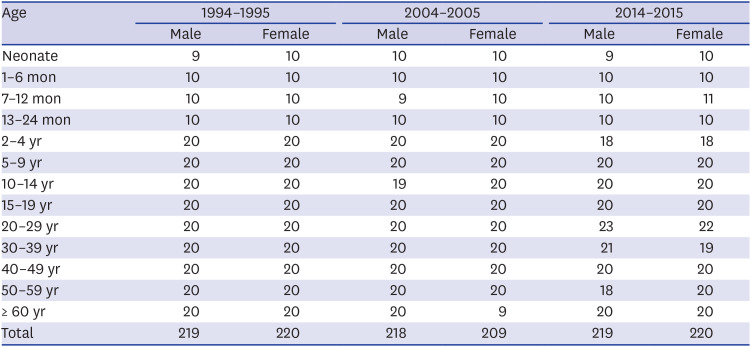
Table 1
Numbers and age distribution of subjects
![]()
Antigen preparation and western blot analysis
Whole cell extracts of CagA positive-H. pylori strain 51 (obtained from the Korean type Culture Collection; HpKTCC; http://hpktcc.knrrc.or.kr, NCBI Taxonomy ID: 290847) were prepared as described previously.24
H. pylori strain 51 was isolated from a patient with duodenal ulcer at GNUH in 1988 and has been studied extensively since then.1415182224252627 Briefly, H. pylori strain 51 was cultured for 18 hours under the environment of 37°C, 5%–10% CO2 and 100% humidity on Mueller-Hinton agar supplemented with 10% bovine serum. Bacterial cells from each plate were harvested and pelleted by centrifugation at 4,000 × g for 15 minutes. These cells were then suspended in sterile phosphate buffer, broken by ultrasonic treatment using an Ultrasonic W380 (Sonics & Materials Inc., Danbury, CT, USA), and stored at −70°C. The sonicated H. pylori whole cell lysate was then used as an antigen. The presence of anti-CagA IgG, IgA, and IgM antibodies in the serum was then examined by western blot analysis. Briefly, cell lysates were run on 10%–20% sodium dodecyl sulfate-polyacrylamide gels overlaid with a 3% stacking gel, as described by Laemmli.28 These gels were loaded with samples containing 100 μg of antigen along with molecular mass markers (Bio-Rad Laboratories Inc., Philadelphia, PA, USA). Proteins were separated under a constant current of 15 mA for 60 minutes until the bromophenol blue dye migrated out of the gel. Proteins were then transferred onto pre-wetted nitrocellulose (NC) membranes (0.2 micron, Bio-Rad Laboratories Inc.). These membranes were then cut into strips. Strips were incubated with 1:20 diluted serum for 30 minutes at 37°C, rinsed three times with Tris buffered saline containing Tween-20 (TBST; 50 mM Tris-HCl, 150 mM NaCl, 0.05% Tween-20, pH 7.5), and incubated at 37°C for 30 minutes with alkaline phosphatase-conjugated goat anti-human IgG, IgA, or IgM antibodies (Bethyl Laboratories Inc., Montgomery, TX, USA). Three different NC membrane strips incubated with one serum sample were used for incubation with goat anti-human IgG, IgA and IgM antibodies, respectively. After washing with TBST buffer, these strips were incubated with 5-bromo-4-chloro-3-indolyl phosphate as a substrate and nitroblue tetrazolium as a chromogenic indicator. Reactions were stopped after 15 minutes by rinsing these strips several times with buffer (20 mM Tris-HCl, 50 mM EDTA, pH 8.0). These strips were then dried before mounting. Samples showing a band at 116–120 kDa were considered positive for H. pylori CagA IgG, IgA, or IgM antibody (Fig. 1).1415 Results were analyzed by two investigators who were blinded to information about the serum samples including age and sex of subjects, and collection time. The authors interpreted results of western blotting based on Fig. 1 to avoid inconsistency.
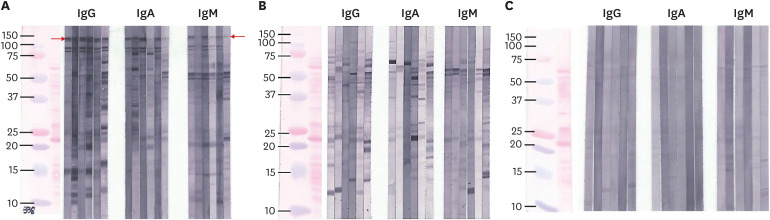 | Fig. 1Three different western blot patterns (A, B, and C) were identified. Only (A) showed reactivity with a 116–120 kDa band (red arrow).Thus it was considered positive for IgG, IgA, and IgM anti-CagA-H. pylori antibodies. (B) showed several other bands after reacting with whole cell lysate of H. pylori 51. No definitive band was observed in (C). (C) Phosphate buffered saline was used as a negative control.Ig = immunoglobulin, CagA = cytotoxic-associated gene A, H. pylori = Helicobacter pylori.
|
Statistical analysis
The χ2 or Fisher's exact test was used to compare differences in seropositivities for anti-CagA IgG, IgA, and IgM antibodies according to age, sex, and study period. All statistical analyses were performed using SPSS ver 25.0 (IBM, Armonk, NY, USA). The level of significance was set at 0.05. GraphPad Prism 8 (Graph-Pad Software, San Diego, CA, USA) was used for graphics.
Ethics statement
The study protocol was approved by the Institutional Review Board at Gyeongsang National University Hospital (GNUH 2015-06-010). Informed consent was waived by the board.
Go to :
RESULTS
A total of 1,305 serum samples were tested, of which 656 were from males and 713 were from subjects younger than 20 years old. Of these samples, 439, 427, and 439 were obtained from 1994 to 1995, 2004 to 2005, and 2014 to 2015, respectively (Table 1).
Anti-H. pylori CagA IgG antibody seropositivity according to age and study period
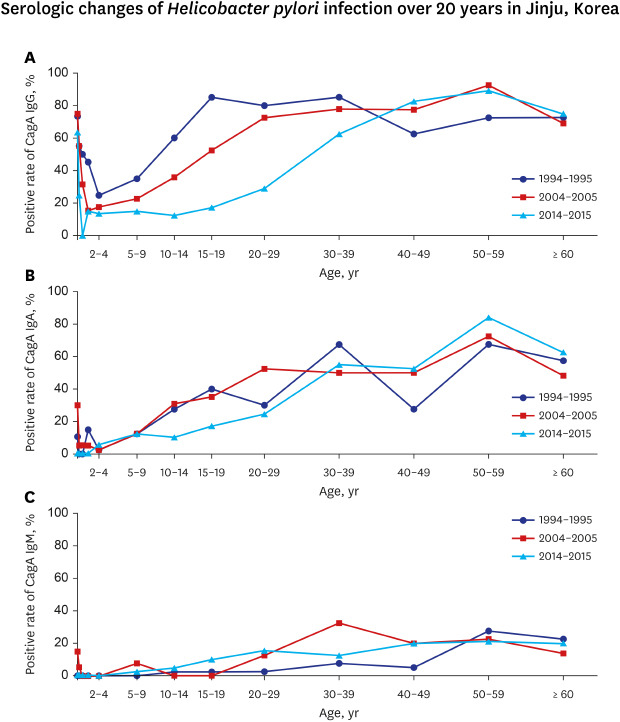
The overall seropositive rate, except for the anti-CagA IgG positive rate in infants aged 0–12 months, was 63.2% from 1994 to 1995, 54.9% from 2004 to 2005, and 42.5% from 2014 to 2015 (P < 0.001), respectively. There was no difference in overall anti-CagA IgG positive rate between males and females (male, 54.9%; female, 50.4%; P = 0.108).
Age-specific seropositive rates of anti- CagA IgG antibodies in each study period are plotted in Fig. 2. Anti-CagA IgG antibody seropositivities according to age in the three cross-sectional periods were decreased from newborn to 7–12 month-old group or 2–4 year-old group and then increased with age (Fig. 2). Seropositive rate of neonates was 73.7% in 1994–1995, 75.0% in 2004–2005, and 63.2% in 2014–2015 (P = 0.765). The lowest seropositive rate in each study period was 25.0% in those age 2–4 years in 1994–1995, 15.0% in those age 13–24 months in 2004–2005, and 0.0% in those age 7–12 months in 2014–2015. Significant reductions in age-specific anti-CagA IgG seropositivities, particularly in those aged between 7 and 12 months, 10 and 14 years, 15 and 19 years, and 20 and 29 years were presented over 20 years (P < 0.05) (Fig. 2 and Table 2). The age when the seropositivity for anti-CagA IgG reached a plateau was delayed over the 20 years and occurred in the 15–19 year-old group in 1994–1995 (85.0%), the 20–29 year-old group in 2004–2005 (72.5%), and the 40–49 year-old group in 2014–2015 (82.5%), respectively. And then the highest rate in each study period occurred in the 15–19 year-old group in 1994–1995 (85.0%), and the 50–59 year-old group in 2004–2005 (92.5%) and 2014–2015 (89.5%), respectively. Seropositivities in early childhood (2–4 years old) during the three study periods decreased numerically from 1994 to 2015 (25% in 1994–1995, 17.5% in 2004–2005 and 13.9% in 2014–2015). However, the decrease was not statistically significant (P = 0.484) (Table 2). According to the birth cohort of the 2–4 year-old group in 1994–1995, positive rates were not significantly changed until individuals were in their 20s in 2014–2015 (25.0% in 1994–1995, 35.9% in 2004–2005 and 28.9% in 2014–2015, P = 0.587) (Table 2).
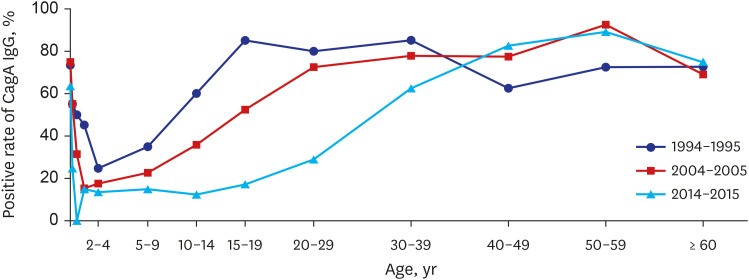 | Fig. 2Changes in anti-CagA IgG antibody seropositivity according to age during a 20-year study in Jinju. Each line connects values for each study period: 1994–1995 (line with circle), 2004–2005 (line with square), and 2014–2015 (line with triangle). There were significant differences in age specific seropositivity with time (from 1994 to 2015) between those aged 7–12 months and 10–29 years (P < 0.05). Anti-CagA IgG seropositivity in early childhood (age, 2–4 years) remained low and stable over 20 years.CagA = cytotoxic-associated gene A, Ig = immunoglobulin.
|
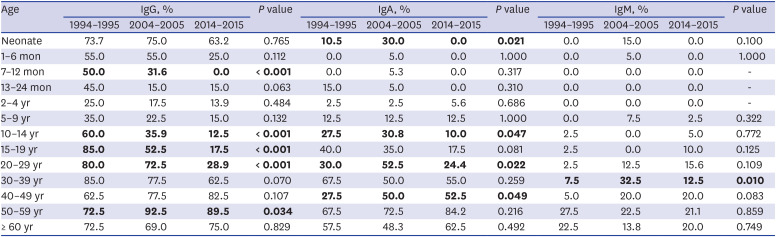
Table 2
Positive rate of anti-CagA IgG, IgA, and IgM according to age and year
Statistically significant differences according to age and study period are shown in bold.
CagA = cytotoxic-associated gene A, Ig = immunoglobulin.
![]()
Anti-H. pylori CagA IgA seropositivity according to age and study period
The overall rate of anti-CagA IgA seropositivity in each study period was 31.4% in 1994–1995, 34.0% in 2004–2005, and 29.4% in 2014–2015 (P = 0.354). The anti-CagA IgA seropositive rate was relatively low in infancy and early childhood (2–4 years old group) in each study period. After early childhood, anti-CagA IgA positive rate appeared to increase with age (Fig. 3).
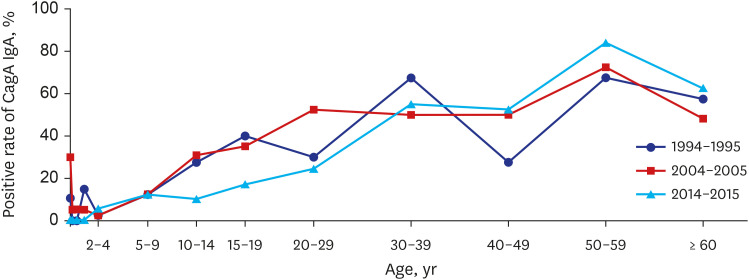 | Fig. 3Changes in anti-CagA IgA seropositivity according to age over the 20-year study period. Each line connects values for each study period: 1994–1995 (line with circle), 2004–2005 (line with square), and 2014–2015 (line with triangle). There was no significant reduction in seropositivity according to age over time.CagA = cytotoxic-associated gene A, Ig = immunoglobulin.
|
Anti-H. pylori CagA IgM seropositivity according to age and study period
Overall seropositivities for anti-CagA IgM antibodies in 1994–1995, 2004–2005, and 2014–2015 were 6.4%, 10.8%, and 9.8%, respectively (P = 0.060). Overall seropositive rates of anti-CagA IgM over the last 20 years were generally low compared with those of anti-CagA IgG and anti-CagA IgA (Fig. 4). According to age, anti-CagA IgM seropositive rates were generally lower in individuals younger than 20 compared with those in adults ≥ 20 years old.
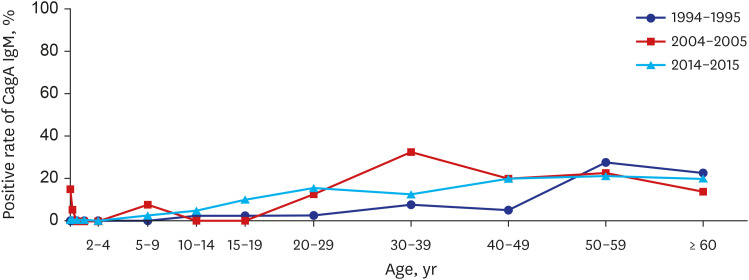 | Fig. 4Changes in anti-CagA IgM seropositivity according to age during the 20-year study period in Jinju. Each line connects values for each study period: 1994–1995 (line with circle), 2004–2005 (line with square), and 2014–2015 (line with triangle). There was no significant reduction in seropositivity according to age over time.CagA = cytotoxic-associated gene A, Ig = immunoglobulin.
|
Go to :
DISCUSSION
The present study showed that the overall seroprevalence of anti-H. pylori CagA IgG antibodies in Jinju, Korea, decreased from 63.2% to 42.5% between 1994 and 2015. Recent decline in the incidence of H. pylori infection with time was similar to a previous study.11 However, the rate of H. pylori in adolescents and adults aged 15 years and older was higher in Jinju (73.8% in 2004–2005) than other regions of Korea (59.6% in 2005).
Anti-CagA IgG seropositivity increased with age from early childhood. Subjects older than 10 years of age in 1994–1995, 20 years of age in 2004–2005 and 30 years of age in 2014–2015 showed seropositive rates of over 60% (Table 2 and Fig. 2). Age-related increase of seropositivity observed in each study period in the present study may represent a cohort phenomenon2329 rather than newly acquired H. pylori infections as individuals get older. Previous studies have also noted that birth cohort effects can lead to an increasing seroprevalence of H. pylori infection with age and decreasing seroprevalence observed in subsequent generations.1130 In this study, the age to a plateau of anti-CagA IgG positive rate tended to be delayed by 10–20 years of age for each study period (Fig. 2). The shifts of age to a plateau over 20 years and the marked reduction of positive rates in the 10–20s age groups in the present study suggests that the prevalence of CagA positive H. pylori infection in Jinju will decline further in the coming decades. However, the relatively stable positive rate in the cohort of children aged 2–4 years in 1994–1995 (25%) over 20 years (35.9% of 10–14 year-old group in 2004–2005 and 28.9% of 20–29 year-old group in 2014–2015, P = 0.587) (Table 2 and Fig. 2) may contribute to persistently stable colonization of H. pylori and the incidence of H. pylori-associated disease in Jinju in the future, albeit low. Further studies on incidences of CagA positive H. pylori-associated diseases are warranted.
During the three study periods, neonates and infants showed high rates of anti-CagA IgG seropositivity (Table 2 and Fig. 2). However, such high rates could not be evidence of H. pylori infection in newborns and infants. Rather, they could represent positive rates in femalesof childbearing age. This was supported by the finding that rates of anti-CagA IgG seropositivity in those younger than 6 months of age was similar to those in females aged 15–49 years in each study period. The rate of anti-CagA IgG seropositivity in those younger than 6 months of age was 64.1% in 1994–1995, 65.0% in 2004–2005, and 43.6% in 2014–2015. Corresponding rates in females aged 15–49 years were 78.8%, 66.3%, and 46.9%, respectively. Transplacental transmission of anti-CagA IgG might cause high positivities in neonates and infants because IgG can transfer passively from a mother to a fetus. Therefore, the overall seropositive rates of anti-CagA IgG in this study were calculated excluding neonates and infants. Serum samples from babies and females aged 15–49 years were randomly assigned and the mother-infant relationship was unknown in the present study. Further studies with paired serum samples from babies and their mothers would be necessary.
Overall rates of anti-CagA IgA seropositivity were similar among the three study periods (P = 0.354). Unlike those measured in a previous study,30 the authors found that the anti-CagA IgA seropositivity during each study period gradually increased with age, particularly after 2–4 years of age (Fig. 3). Anti-CagA IgG and IgA seropositivities around 1–4 years of age showed lower rates than others. And IgG and IgA seropositivities in those older than 5 years increased along with age for each period. Thus, the authors tentatively estimated the time of H. pylori infection for each period might have occurred in early childhood, especially of those younger than 4 years old in Jinju, Korea (Figs. 2 and 3).
Generally, IgM and IgA antibodies could be produced as a primary response. Greater quantity of IgG antibodies could be produced as a secondary response after antigen exposure. Specific IgG could persist several months or years. Positive anti-CagA IgA could represent mucosal immune response in H. pylori infection. In addition, mucosal immune response in a person infected with H. pylori might occur repeatedly.21 Based on humoral immune response sequences and our results of higher anti-CagA IgG positivities in the older birth cohort and anti-CagA IgA seropositivity patterns along with age, especially in those older than 5 years, anti-CagA IgA antibodies might be repetitively produced by the active mucosal immune response of already existing bacteria rather than acute infection.192021 Our findings could support that H. pylori infection is acquired during early childhood while new infections during adulthood are rare (Figs. 2 and 3).161731
Humoral IgA response in newborns and infants is usually weak. The low rate of anti-CagA IgA seropositivity in neonates and infants younger than 2 years of age in the present study might represent sporadic acute H. pylori infection.21 Rates of anti-CagA IgA seropositivity in those aged 60 years and older were lower than those in subsequent generations during the three study periods (Fig. 3). Development of atrophic gastritis, intestinal metaplasia, or gastric cancer in the elderly may have contributed to the lower anti-CagA IgA seropositivity because H. pylori disappears from the gastric mucosa after these diseases develop.1617 However, further studies are warranted to determine the relationship between anti-H. pylori CagA IgA seropositivity and mucosal inflammation or histologic status of the gastric mucosa. In children and adolescents, anti-CagA IgA seropositivity might reflect inflammation of the gastric mucosa caused by H. pylori based on our unpublished research, which showed that 81.5% (202 of 247) of anti-CagA IgA-positive subjects aged less than 20 years in Jinju had active gastritis.
The present study showed that age-specific rates of anti-CagA IgM seropositivity during the three study periods were very low compared with those of anti-CagA IgG and IgA seropositivity (Fig. 4). Anti-CagA IgM antibody has not been well established as a meaningful marker of H. pylori infection yet.20 However, a small number of acute H. pylori infections could be acquired sporadically at any age including the newborn period. In addition, H. pylori might invade the gastric mucosa or re-infect an already infected person during their lifetime, although this is likely to be uncommon.32
This study has several limitations. First, any information regarding housing or economic circumstance was not provided. Neither medical information such as H. pylori eradication nor clinical outcome of subjects associated with CagA-positive H. pylori was provided. Second, this was a retrospective cross sectional cohort study based on limited geography. Regional limitation may account for our finding of a higher seroprevalence of H. pylori infection than that of a previous nationwide survey.11 Third, the authors used western blotting for qualitative analyses of IgG, IgA and IgM antibodies. However, western blotting has been extensively validated as a method for the detection of several antibodies at the same time. And it is, in fact, more sensitive and specific for anti-H. pylori antibodies in younger children including infants than an ELISA.1533 Finally, presence of CagA negative H. pylori among the study population and change in antigenicity of CagA over 20 years might be possible. However, since CagA positive H. pylori comprises a large proportion of strains identified in Korea so far,4 CagA negative H. pylori might account for a small portion in the present study. Nevertheless, the present study has a strength; it examined temporal changes in CagA positive H. pylori infection in a relatively constant population from birth to old age, over a period of 20 years.
Results of this study suggest that Jinju may experience a lower prevalence of CagA positive H. pylori infection and associated diseases in the future. However, the low and stable seroprevalence of CagA positive H. pylori infection in early childhood over 20 years suggests that low, albeit constant, colonization by the bacterium may continue. Transmission of H. pylori could be highly affected by intrafamilial and environmental exposure,2431343536 and infection could occur in early childhood and persist without treatment.161718 Therefore, education regarding personal hygiene such as hand washing and eating habits in family,37 and aggressive diagnosis and eradication could help reduce colonization.3839 Establishment of a diagnostic and therapeutic strategy in children with H. pylroi infection in Korea is necessary.
Go to :
 XML Download
XML Download