

 PDF
PDF Citation
Citation Print
Print




INTRODUCTION
All cirrhotic patients should be screened for varices at diagnosis.1 An upper endoscopy is the recommended procedure to screen varices, but it is uncomfortable. Moreover, some patients with cirrhotic echotexture may not have significant portal hypertension.2 The term ‘compensated advanced chronic liver disease (cACLD)’ is used to define the population of asymptomatic patients with severe fibrosis/compensated cirrhosis.3 There is also considerable interest in developing non-invasive models to predict the presence of varices in patients with cACLD. Liver stiffness measurements (LSMs) with transient elastography (TE) have been widely evaluated in patients with chronic liver disease.4567
Baveno VI consensus recommends the combined use of liver stiffness (< 20 kPa) by TE and a platelet count (> 150 × 103/mm3) as criteria to determine if patients can safely avoid an endoscopy.3 Several studies have validated Baveno VI consensus using TE. Following that validation, 10% to 30% of screening endoscopies were spared with a low risk of missing high-risk varices (HRVs).89101112131415 Although correlations between liver stiffness using TE and esophageal varices (EVs) have been found, TE has limited effectiveness, especially in patients with ascites and obesity.16 Recently, 2 dimensional shear-wave elastography (2D-SWE) has been developed as another method for measuring liver stiffness and is based on the combination of a radiation force impulse induced in tissues by focused ultrasonic beams and an ultrasound (US) acquisition of the propagated shear waves imaging sequence,17 unlike TE, liver elasticity values can be obtained based on anatomic information. While previous studies have validated Baveno VI consensus using TE, mostly with hepatitis C virus (HCV) or hepatitis B virus (HBV), Baveno VI consensus has not been validated for the diagnostic performance of 2D-SWE.
Therefore, further studies are needed to validate these non-invasive markers in other etiologies especially alcoholic liver disease. In this study, we aimed to validate these criteria using 2D-SWE in cACLD patients with alcohol as the main etiology.
METHODS
Study cohort
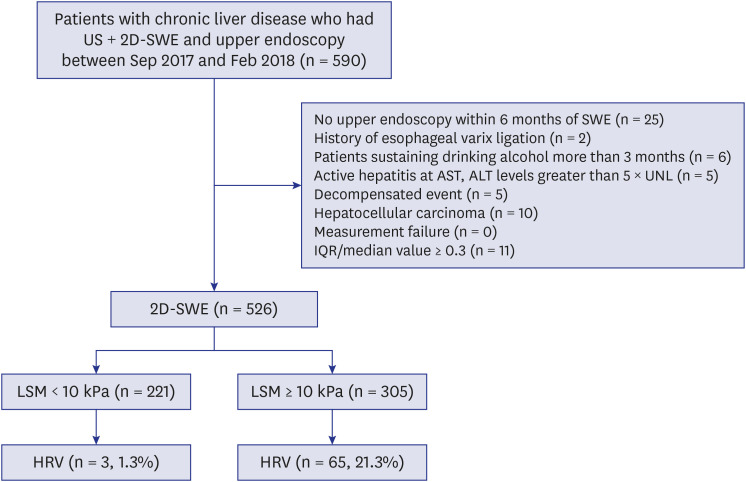
Data from 590 consecutive patients, who were diagnosed with chronic liver disease and who underwent a LSM with 2D-SWE at a single tertiary hospital from September 2017 to February 2018, were extracted from a database retrospectively. We excluded patients if they: 1) had not undergone an upper endoscopy within 6 months of 2D-SWE; 2) had a history of EV ligation; 3) had not stopped drinking alcohol for more than 6 months, 4) had conditions that might interfere with LSM such as active hepatitis, aspartate aminotransferase (AST) or alanine aminotransferase levels greater than 5 times the upper normal limit, or 5) had a history of decompensated cirrhosis or hepatocellular carcinoma (Fig. 1). Patients who either failed their LSM tests (10 valid measurements with a success rate < 60%, n = 0) or who had an unreliable LSM (interquartile range [IQR]/median LSM > 30% with median liver stiffness, n = 11) were also excluded. In total, 526 patients in the 2D-SWE group were included in our study.
Fig. 1
Patient flow diagram.
US = ultrasound, 2D-SWE = 2 dimensional shear-wave elastography, SWE = shear-wave elastography, AST = aspartate aminotransferase, ALT = alanine aminotransferase, UNL = IQR = interquartile range, LSM = liver stiffness measurement, HRV = high-risk varix.
Among them, cACLD was defined as an LSM ≥ 10 kPa, a Child-Pugh class A, and the absence of a prior decompensation event.3 We used LSMs and platelet counts to determine whether patients had a risk of varices that required treatment according to Baveno VI consensus: Baveno VI criteria (LSM < 20 kPa and platelet count > 150 × 103/mm3); expanded Baveno VI criteria (LSM < 25 kPa and a platelet count > 110 × 103/mm3);10 and modified Baveno VI criteria (LSM < 25 kPa and a platelet count ≥ 150 × 103/mm3). Data extracted from medical charts included sex, age, weight, height, liver disease etiology, platelet count, liver biochemistry, serum creatinine, and prothrombin time. We classified the etiology as HBV, HCV, alcohol, or others based on viral markers and the clinical history.
LSM with SWE
A professionally trained operator estimated liver stiffness using 2D-SWE with a dedicated US machine (APLIO 500; Toshiba, Tokyo, Japan). 2D-SWE was performed on the right lobe of the liver through the intercostal space with the patient lying in the supine position after an overnight fast. In 2D-SWE measurements, US was first performed using the conventional B mode, with the patient's right arm elevated above the head for optimal intercostal access. The 2D-SWE box was approximately 4 × 3 cm and was placed 1–2 cm under the liver capsule in the parenchymal area of the right hepatic lobe (7th to 10th intercostal) space, which was free of large bile ducts and vessels. The region of interest (mean diameter, 20 mm) was positioned inside the elasticity image (mainly in the center of the box where the elasticity image was more homogeneous) after each acquisition to obtain the mean LSM. The stiffness value (kPa) was automatically displayed by the US system. Each value was recorded, and the final stiffness value was calculated as the mean of the recorded acquisitions.
Screening of EV
Endoscopy for EV screening using a video endoscope was performed by experienced endoscopists with more than 5 years of experience. EVs were classified into four groups according to their shape and size in accordance with Baveno VI consensus: No varix; F1: straight, small-caliber varices; F2: moderately enlarged, beady varices; and F3: markedly enlarged, nodular, or tumor-shaped varices.3 The presence of red wale marks on the esophageal variceal wall was described as a red sign. HRV were defined as F2/3 varices or an F1 varix with red wale signs.
Statistical analyses
We analyzed the no/low risk varices and HRV cohorts separately in the 2D-SWE groups. We used the χ2 test and the independent t-test to evaluate differences in the clinical variables. To identify risk factors for HRV, variables that were significantly different by the independent t-test were used in a logistic regression using the entry method. The discrimination of the prediction for any varices or HRV was assessed by the overall C-index, defined as a natural extension of the receiver operating characteristic area and its 95% confidence interval. Cut-off values for diagnosing EVs and HRV were determined as the maximum combined values of sensitivity and specificity. We compared the patients' LSM, platelet count, Baveno VI criteria, and expanded Baveno VI criteria with the binary outcome measures with and without HRV. We also evaluated sensitivity, specificity, positive predictive value, negative predictive value (NPV), positive likelihood ratio (LR+) and negative likelihood ratio (LR−). A P value < 0.05 was considered statistically significant. The statistical analyses were performed using SPSS for Windows, version 23.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
Baseline characteristics
The baseline characteristics of the 526 patients in the 2D-SWE group are summarized in Supplementary Table 1. The patients were also divided into two groups according to their EV grade (low/no varix or HRV). HRV was identified in 68 patients (12.9%) in the 2D-SWE group. Patients with HRV included those with alcoholic liver disease who had lower hemoglobin, lower platelets, higher AST, higher bilirubin, and a larger spleen size. LSM was significantly higher in patients with HRV. The distribution of liver stiffness values by 2D-SWE was as follows: low/no varix, 10.1 kPa (IQR, 8.2–15.2); HRV, 21.7 (IQR, 14.8–30.5).
Among the 526 patients, 305 were patients with cACLD (58.0%). The baseline characteristics of the 305 patients with cACLD in the 2D-SWE group are summarized in Table 1. HRV was identified in 21.3% (n = 65) of patients with cACLD in the 2D-SWE group.
Table 1
Baseline characteristics of patients with cACLD in 2D-SWE performance
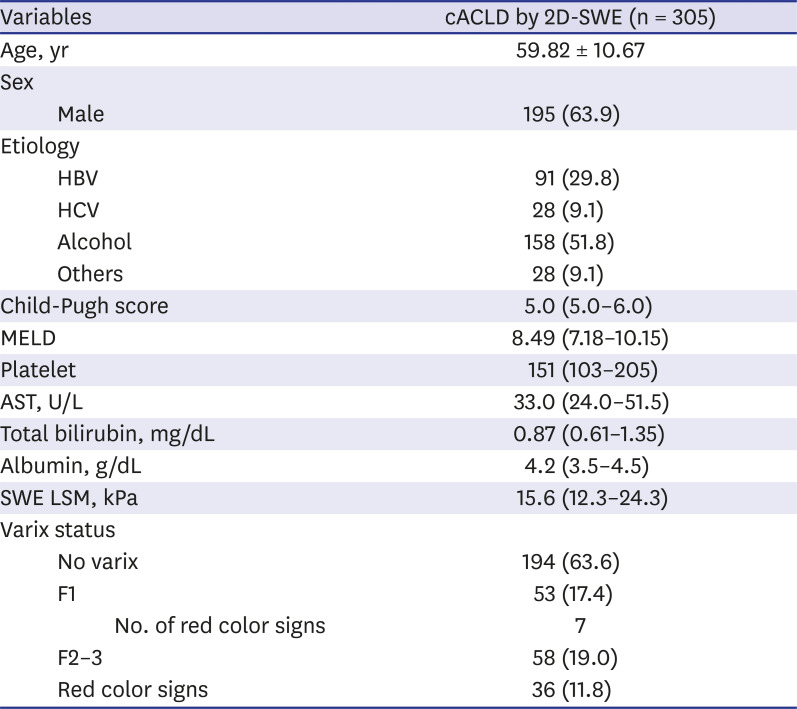
Data are presented as mean ± standard deviation, number (%), or median (interquartile range).
AST = aspartate transaminase, cACLD = compensated advanced chronic liver disease, 2D-SWE = 2 dimensional shear-wave elastography, HBV = hepatitis B virus, HCV = hepatitis C, LSM = liver stiffness measurement, MELD = Model for End-Stage Liver Disease, SWE = shear-wave elastography.
Prediction of any varices or HRV
The discrimination of the prediction for any varices or HRV was assessed by calculating the C-statistic. In the presence of EV, the C-index of LSM by 2D-SWE, spleen size, and platelet count were 0.79, 0.77 and 0.27, respectively (Table 2). The optimal liver stiffness cut-off value for 2D-SWE was 14.5 kPa. In the prediction for HRV, the C-index of LSM by 2D-SWE, spleen size, and platelet count were 0.73, 0.78 and 0.25, respectively. The optimal liver stiffness cut-off value for 2D-SWE was 15.1 kPa.
Table 2
C-index of the LSM with 2D-SWE, spleen size and the platelet count in the presence of EVs and high-risk EVs in patients with cACLD
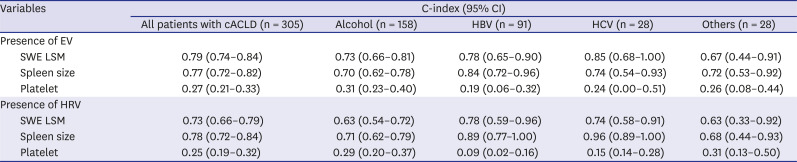
In the cACLD etiologies subgroup analysis, the C-index of 2D-SWE for the prediction of any varices was 0.73 in alcohol liver disease vs. 0.78 (HBV) and 0.85 (HCV) in viral-related liver diseases. The C-index prediction of HRV was 0.63 in alcohol liver disease vs. 0.78 (HBV) and 0.74 (HCV) in viral-related liver diseases. As a result, 2D-SWE in alcohol liver disease tend to have a lower C-index for the prediction of any varices or HRV compared to viral-related liver diseases.
Diagnostic performance of Baveno VI and expanded Baveno VI criteria in cACLD
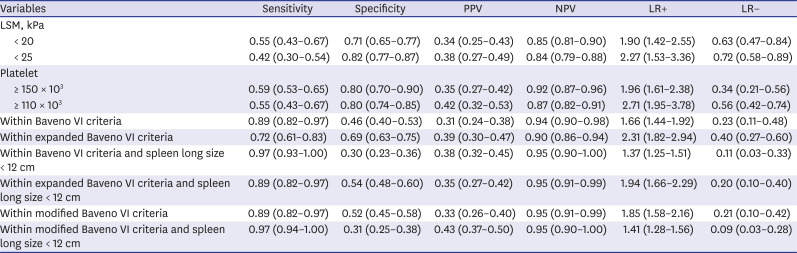
In total, 118 of the 305 (38.7%) patients in the 2D-SWE group were spared endoscopy using Baveno VI criteria (Table 3). Among these 118 patients, 14 (11.9%) had low-risk varices and seven (5.9%) presented with HRV and were therefore missed. Expanded Baveno VI criteria spared more endoscopies (60.0%) but missed more HRV (9.8%) compared with Baveno VI criteria. Sensitivity (0.89 vs. 0.72) and NPV (0.94 vs. 0.90) were higher for Baveno VI criteria than for expanded Baveno VI criteria (Table 4).
Table 3
Prediction of any or high-risk varices by criteria in 2D-SWE performance, n = 305
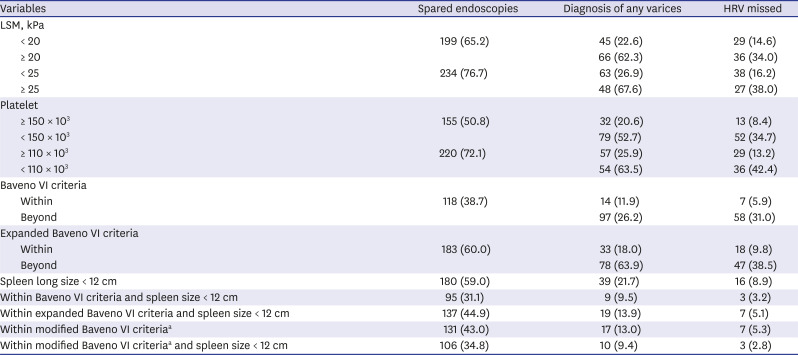
Table 4
Performance of criteria in the prediction of high-risk esophageal varices with 2D-SWE, n = 305
Diagnostic performance of the modified Baveno VI criteria in cACLD
Overall, the risk of missing HRV in this study was high when using Baveno VI and expanded Baveno VI criteria (5.9% and 9.8%). A total of 131 of the 305 (43.0%) patients evaluated in the 2D-SWE group were within the modified Baveno VI criteria (LSM < 25 kPa and a platelet count ≥ 150 × 103/mm3), of whom seven (5.3%) had missed HRV. The NPV of the modified Baveno VI criteria (0.95) was slightly higher than that of Baveno VI criteria (0.94) and expanded Baveno VI criteria (0.90).
Adding spleen diameter to Baveno VI and the modified Baveno VI criteria
We also tested the possibility of applying long spleen diameters to identify patients with HRV in the cACLD group. The number of spared endoscopies decreased slightly to 95/305 (31.1%) after adding long spleen diameters (< 12 cm) to patients who met Baveno VI criteria, with only three (3.2%) presenting with HRV which represented a decrease in the miss rate. However, when long spleen diameter (< 12 cm) was added to the expanded Baveno VI criteria, the number of saving endoscopy (44.9%) was increased, but the risk of missing HRV (5.1%) was still high. Then, after adding long spleen diameters (< 12 cm) to the modified Baveno VI criteria, the number of spared endoscopies slightly increased by 106 of 305 (34.8%) with three (2.8%) presenting with HRV indicating that the risk of missing an HRV was low. The NPV of adding long spleen diameters to the modified Baveno VI criteria (0.95) was similar to the modified Baveno VI criteria (0.95). The area under the receiver-operating characteristic curve curves for the detection of HRV indicated better performance of modified Baveno VI criteria compared with Baveno VI criteria (See more information in Supplementary Result, Supplementary Data 1).
Diagnostic performance of Baveno VI and expanded Baveno VI criteria by the etiology of cACLD
A cACLD etiology subgroup analysis in all patients from the 2D-SWE group was performed (Table 5). The main etiology was alcoholic liver disease, followed by HBV and HCV.
Table 5
Performance of criteria in the prediction of high-risk esophageal varices according to etiology with 2D-SWE, n = 305
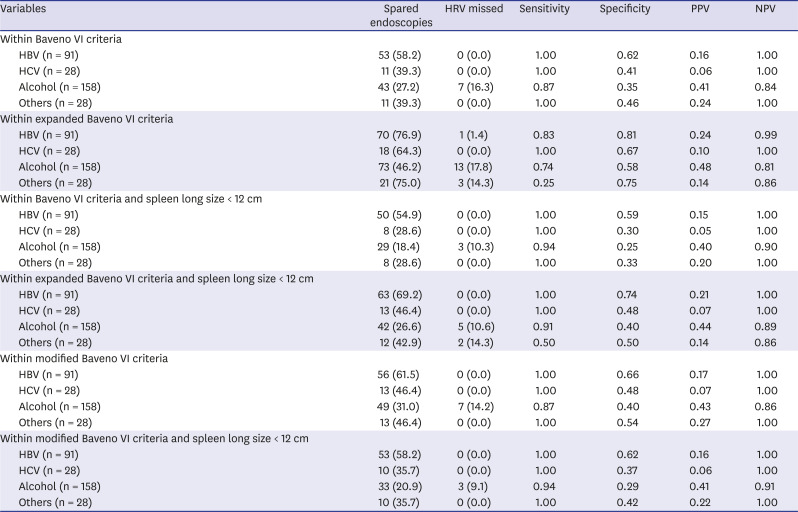
The risk of missing an HRV in the 2D-SWE group was < 5% in HBV-related liver disease, whilst the miss rate was > 10% for patients with alcoholic liver disease which met Baveno VI and expanded Baveno VI criteria. However, using a higher LSM cut-off (< 25 kPa) and platelet counts ≥ 150 × 103/mm3 (modified Baveno VI criteria) together with long spleen size (< 12 cm) slightly decreased the HRV miss rate (16.3% vs. 9.1%) compare to Baveno VI criteria. The numbers in the subgroups for the other etiologies were too low to reach robust conclusions (hepatitis C and other diseases).
DISCUSSION
This study validated Baveno VI and expanded Baveno VI criteria for using noninvasive methods (2D-SWE) to identify those who are at low risk of varices and can safely avoid endoscopies. Several studies have validated these criteria with TE. 2D-SWE is a promising new technique for measuring liver stiffness, which is integrated into conventional US images and is easy to comprehend.18 Our study was the first to validate Baveno VI criteria with 2D-SWE. The secondary objective was to validate these criteria by 2D-SWE in cACLD patients with alcohol as the main etiology.
We demonstrated that Baveno VI criteria and 2D-SWE reduced the number of surveillance endoscopies by approximately 38.7%, but missed 5.9% of HRV. The risk of missing HRV was higher than that reported in previous studies.89101112131415 Several reasons might explain this discrepancy. First, the discrepancies could be due to differences in the patient populations. Our study comprised patients with alcohol as the main etiology which is understated in previous studies. Baveno VI criteria were introduced and validated in Western countries, where HCV is the main etiology of chronic liver disease. Since most of the available validated results involve patients with HBV and HCV, the accuracy of Baveno VI criteria in patients with alcoholic liver disease remains to be elucidated. In this study, the NPV of Baveno VI criteria was lower in patients with alcoholic liver disease (0.84) than in those with HCV (1.00) or HBV (1.00). A high incidence of complication-related portal hypertension has been reported in patients with alcoholic liver disease.1920 In our study, an alcohol etiology was more common in patients with HRV than in those without. These results indicate the possibility for a lower performance of Baveno VI criteria among patients with alcoholic liver disease than in those with viral liver diseases.
Next, the cut-off values of liver stiffness for liver fibrosis or cirrhosis vary according to the etiology of the liver disease.21 Meta-analyses demonstrated that the etiology of liver disease is one of the most important factors leading to the heterogeneity of LSM results, indicating that different chronic liver diseases should be analyzed separately.2122 Moreover, compared with other etiologies, few studies have assessed a group of patients with alcoholic liver disease or, if assessed, they only represented a small percentage of the entire group.232425 Previous studies have reported that the median liver stiffness value of patients with alcoholic cirrhosis is higher than that measured in patients with viral cirrhosis. This may be explained by the different pathological distributions of alcoholic fibrosis which develops in the centrilobular and perisinusoidal areas as well as in the periportal regions.26 Therefore, the optimal cut-off value of liver stiffness for the HRV rule-out criteria differs according to the etiology of the liver disease.27 Thus, we examined the LSM cut-off of 25 kPa in combination with a platelet count > 150 × 103/mm3 defined as the modified Baveno VI criteria. These criteria spared additional endoscopies (38.7% vs. 43.0%) with a slightly lower number of missed HRV (5.9% vs. 5.3%) when using 2D-SWE.
Although non-invasive investigations such as LSM and spleen size by 2D-SWE had a high C-index for diagnosing varices and HRV, LSM by 2D-SWE in alcohol liver disease had the lowest C-index in the cACLD etiologies subgroup analysis. Instead, variables of spleen size were more able to discriminate HRV than LSM when using 2D-SWE. In fact, the combination of LSM with other spleen-related parameters resulted in an increased diagnostic accuracy for predicting varices. This hypothesis was derived from the finding that spleen parameters reflect extra-hepatic hemodynamic changes. A previous study on patients with compensated cirrhosis showed that LSM by TE, in combination with platelet count and spleen diameter, had a high NPV (0.95) for excluding HRV.2829 All predictors were effective in predicting varices that accompany splenomegaly. Our cohort data clearly indicated that applying long spleen diameters (< 12 cm) to patients beyond Baveno VI criteria can be safely done with a lower number of missed HRV when using 2D-SWE (5.9% vs. 3.2%). Moreover, adding long spleen diameters together with an LSM cut-off of 25 kPa was an even better tool because it spared additional endoscopies compared with Baveno VI criteria and long spleens (31.1% vs. 34.8%) with the lowest HRV miss rate (2.8%). Thus, spleen size was a promising tool when added to Baveno VI or modified Baveno criteria. In this aspect, 2D-SWE is a better tool because it measures spleen size in addition to liver stiffness which is integrated into conventional US images.
Previous studies have shown that expanded Baveno VI criteria improved the original criteria. The number of spared endoscopies could almost be doubled when applying the expanded Baveno VI criteria using 2D-SWE (from 38.7% to 60.0%); however, they were not safe with about a 10% varices needing treatment missing rate under most conditions. Our data comprised patients with alcohol as the main etiology, indicating that Baveno VI criteria or modified Baveno VI criteria are more acceptable than expanded Baveno VI criteria.
Several limitations should be considered when interpreting our findings. First, because this study was based on retrospectively collected variables, selection bias may have affected the results. Second, upper endoscopy, platelet count, and 2D-SWE were not performed on the same day. However, these variables do not change significantly within a short period of time and most likely did not affect any outcomes.
In conclusion, Baveno VI criteria were validated using 2D-SWE in patients with alcohol as the main etiology. Although 2D-SWE and Baveno VI criteria provided a high NPV for HRV, it was insufficient with an HRV miss rate of over 5%. However, using the modified Baveno VI criteria (LSM cut-off < 25 kPa) together with long spleen size (< 12 cm), more endoscopies were spared with a minimal risk of missing HRV in cACLD patients with alcohol as the main etiology. If our results are confirmed and validated in larger cohorts, they may be useful in identifying patients with cACLD who can safely avoid a screening endoscopy.
 XML Download
XML Download