

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Peripheral facial nerve palsy refers to lower motor neuron lesion of the facial nerve and can occur as a result of various medical conditions such as infection, cholesteatoma, trauma, malignancy, autoimmune issues, and pregnancy. The most common disease causing peripheral facial nerve palsy is idiopathic Bell's palsy.1 For the pathogenesis of idiopathic Bell's palsy, reactivation of Herpes simplex virus type 1 is presumed to be the most relevant infection. Other viral infections such as varicella zoster virus and human herpes virus 6 are quite common. However, in most cases etiologies are not revealed, though various serological tests using paired serum or saliva, blood, and cerebrospinal fluid are performed.23 In relation to the time course, this can be classified into acute, subacute, and chronic lesions.4 In relation to terminology, ‘paresis’ is used to describe incomplete lesions and ‘paralysis’ is generally employed if the palsy is complete. For laterality, the condition occurs unilaterally in most cases, but bilateral facial palsy is also possible, though uncommon.
The American Academy of Neurology (AAN) and the American Academy of Otolaryngology-Head and Neck Surgery (AAO-HNSF) published clinical practice guidelines for Bell's palsy in 2012 and 2013, respectively.56 In addition, a similar guideline was also issued in Canada in 2014.7 Since then, a number of randomized controlled trials (RCTs) and meta-analyses have been conducted on matters which may or may not have been covered in these guidelines. The present study reviewed not only the recommendations that were made in these guidelines, but also the results of any systematic reviews and meta-analysis studies published between 2011 and 2019. In addition, interesting findings that could not be verified by RCTs because of the specificities of the situation, were also reviewed. For convenience, we have used the AAO-HNSF guidelines as the backbone for this study and appended further details, descriptions and findings as appropriate.
Go to : 
METHODS
Literature search strategy
Electronic database searches were performed (using MEDLINE, EMBASE, Scopus, and Cochrane) in order to identify recent guidelines dealing with facial nerve palsy, systematic reviews and recent meta-analyses between 2011 and 2019. The literature search was conducted using the search terms “Bell’s palsy,” “Ramsay-Hunt syndrome,” “Facial palsy,” “Facial paralysis,” “Facial paresis,” “Guideline,” “Meta-analysis,” “Systematic review,” and “Randomized controlled trial.” Only studies written in English were utilized in this study. Institutional Review Board approval was not required due to the nature of this study.
Selection of studies
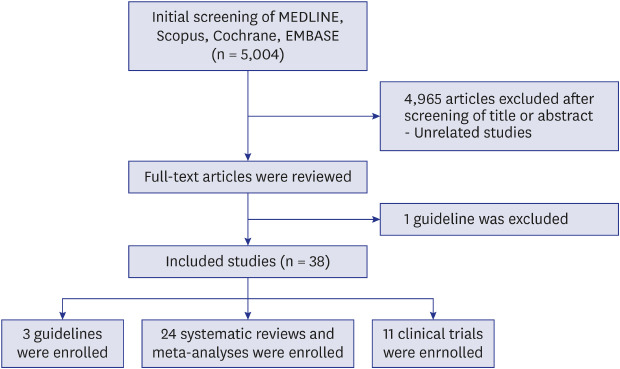
All titles and abstracts for studies located through searches were initially screened for relevance, and the full text of each study that was potentially of importance was reviewed in detail. Clinical practical guidelines by official otolaryngologist or neurologist societies during the search period were also eligible for review and the results of recent meta-analyses were similarly incorporated into this study. Studies were excluded if the content did not target the management of peripheral facial palsy and/or epidemiologic characteristics (Fig. 1).
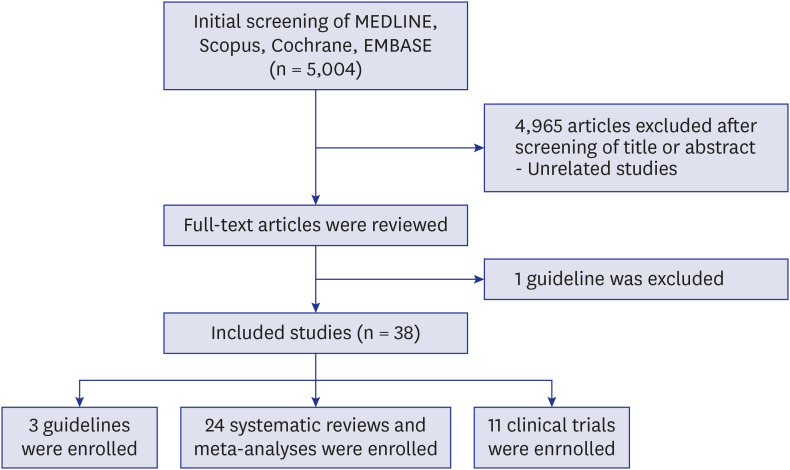 | Fig. 1Research parameters. An electronic database search was performed to retrieve facial nerve guidelines and recent randomized trials until 28th February 2020. One guideline (please refer to [4]: Rath B, Gidudu JF, Anyoti H, Bollweg B, Caubel P, Chen YH, et al. Facial nerve palsy including Bell's palsy: Case definitions and guidelines for collection, analysis, and presentation of immunisation safety data. Vaccine 2017;35(15):1972-83.) was excluded on the basis of our exclusion criteria, because this was not intended to target the practical management of peripheral facial palsy, but rather reporting methods.
|
Go to :
RESULTS
Medical history
The AAO-HNSF guidelines strongly recommend a close examination of the medical history of the patient presenting alongside a physical examination. Through the medical history, the clinician should be able to identify possible causes of acute-onset facial paresis or paralysis.5 In the latter guidelines, “acute” is defined as an onset within less than 72 hours.5 In addition, for a diagnosis of Bell’s palsy, no other identifiable causes should be confirmed and, in general, patients should present with unilateral facial nerve paresis or paralysis.5 The use of the latter terms is quite strictly differentiated; facial “paralysis” should be used in cases of complete inability to move the face and, for cases with incomplete ability to move the face, “facial paresis” should be used.5 Other guidelines, meta-analyses, and systematic reviews observed during this study period did not differ from the AAO-HNSF guidelines in recommendations in these regards.
Facial nerve grading systems
Various facial nerve grading systems have been proposed including; the House-Brackmann grading system, the Facial Nerve Grading System 2.0, the Yanagihara grading system, the Sunnybrook facial grading system and eFACE. The most widely used grading system appears to be the House-Brackmann grading system. However, the Sunnybrook facial grading system and eFACE have been gaining in prominence during the study period.8 Though the latter two grading systems show moderately strong agreement, eFACE has a shorter testing time, higher test-retest reliability and the ability to be used as a smartphone test. However, the Sunnybrook facial grading system is now recommended by the Sir Charles Bell Society (Please kindly refer to the following website for more information concerning the Sunnybrook facial grading system: https://sunnybrook.ca/uploads/FacialGradingSystem.pdf).9
Laboratory testing & electrodiagnostic testing
The AAO-HNSF guidelines recommend against the use of routine laboratory testing for new-onset Bell's palsy.5 This is due to low detection rates for the herpes simplex virus, or varicella zoster virus, even with the use of polymerase chain reaction, enzyme-linked immunosorbent assay (ELISA), western blot, and cerebrospinal fluid tapping. In a recent meta-analysis of hematologic markers, the neutrophil-to-lymphocyte ratio (NLR), which reflects the severity of inflammation, was higher in Bell's palsy, while a lower NLR was observed in patients with more favorable outcomes.10 In addition, positive ELISA to Borrelia species were also quite common in residents with facial palsy living in Mexico.11 Obtaining a precise travel history to identify visits to endemic areas may thus be helpful for a consideration of the most appropriate laboratory testing procedures.
According to the AAO-HNSF guidelines, electrodiagnostic tests for those presenting with incomplete paralysis is not recommended, though offering these tests to those with complete paralysis may be justifiable.5 For facial palsy after temporal bone trauma, serial electroneuronography (ENoG) may be helpful for the confirmation of a deterioration in facial nerve function in patients who have not recovered during observation.12 During the study period, high quality randomized trials or other well-designed studies dealing with various kinds of laboratory testing were not performed.
Diagnostic imaging & radiologic testing
The AAO-HNSF guidelines recommend against routine diagnostic imaging for new-onset Bell’s palsy.5 In contrast, the Canadian guidelines strongly advocate imaging to rule out neoplasm in patients with no improvement or progressive weakness after treatment.7 High resolution computed tomography findings demonstrated that the labyrinthine segment of the affected side was narrower than the healthy side in Bell's palsy, and the severity of facial palsy was correlated with facial canal diameter.13 However, high quality randomized trials that might have more widely justified the use of diagnostic imaging for facial palsy were not performed during the study period.
Medical conditions associated with facial palsy
The following conditions were reported to be related to the occurrence of facial palsy (Table 1).1567111415
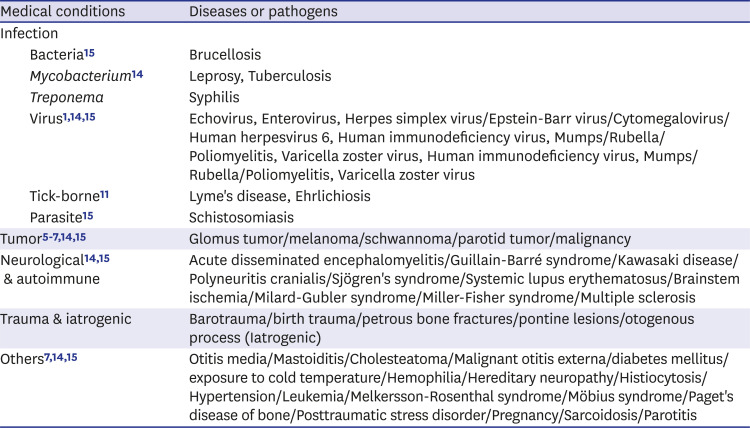
Table 1
Medical conditions associated with facial palsy
| Medical conditions | Diseases or pathogens | |
|---|---|---|
| Infection | ||
| Bacteria15 | Brucellosis | |
| Mycobacterium14 | Leprosy, Tuberculosis | |
| Treponema | Syphilis | |
| Virus11415 | Echovirus, Enterovirus, Herpes simplex virus/Epstein-Barr virus/Cytomegalovirus/Human herpesvirus 6, Human immunodeficiency virus, Mumps/Rubella/Poliomyelitis, Varicella zoster virus, Human immunodeficiency virus, Mumps/Rubella/Poliomyelitis, Varicella zoster virus | |
| Tick-borne11 | Lyme's disease, Ehrlichiosis | |
| Parasite15 | Schistosomiasis | |
| Tumor5671415 | Glomus tumor/melanoma/schwannoma/parotid tumor/malignancy | |
| Neurological1415 & autoimmune | Acute disseminated encephalomyelitis/Guillain-Barré syndrome/Kawasaki disease/Polyneuritis cranialis/Sjögren's syndrome/Systemic lupus erythematosus/Brainstem ischemia/Milard-Gubler syndrome/Miller-Fisher syndrome/Multiple sclerosis | |
| Trauma & iatrogenic | Barotrauma/birth trauma/petrous bone fractures/pontine lesions/otogenous process (Iatrogenic) | |
| Others71415 | Otitis media/Mastoiditis/Cholesteatoma/Malignant otitis externa/diabetes mellitus/exposure to cold temperature/Hemophilia/Hereditary neuropathy/Histiocytosis/Hypertension/Leukemia/Melkersson-Rosenthal syndrome/Möbius syndrome/Paget's disease of bone/Posttraumatic stress disorder/Pregnancy/Sarcoidosis/Parotitis | |
![]()
Oral steroids
The AAO-HNSF guidelines strongly recommend the prescription of oral steroids within 72 hours of symptom onset for Bell's palsy cases aged 16 years or older.5 Similarly, the AAN guidelines also report that steroids are effective in increasing the possibility of complete facial functional recovery.6 However, the latter guidelines do not specify the correct timing for the onset of treatment, nor the type of treatment, nor do they indicate the preferred method of administration. In the Canadian guidelines, corticosteroids were strongly recommended for all patients with Bell's palsy.7 For the appropriate dosage, a recent meta-analysis demonstrated that 100 mg or more of initial high-dose prednisolone reduced non-recovery more when compared with 50–60 mg of an initial standard dosage in Bell's palsy.16
Antiviral therapy & combined antiviral-steroid treatment
Both the AAO-HNSF and the Canadian guidelines strongly recommend against antiviral treatment alone for new-onset Bell's palsy.57 For Ramsay Hunt syndrome, no RCTs were performed during the study period. However, a Cochrane review published in 2008 reported no evidence that supported the use of anti-viral agents, such as those widely used for other herpes zoster infections in other parts of the body.17
According to the AAO-HNSF guidelines, the clinician may use a combined treatment within 72 hours of symptom onset for Bell's palsy.5 The AAN guidelines also state that combined treatment may be offered to increase the probability of the recovery of facial function.6 However, the latter also mentions the necessity of counselling regarding the modest effects of potential benefits of additional antivirals and steroids.6 In the Canadian guidelines, combined treatment is recommended, although the suggested dosage strength is weak irrespective of the degree of paresis.7 A recent Cochrane review published in 2015 reported that combined treatment reduced sequelae of Bell's palsy when compared with steroids alone, though the quality of the evidence was moderate.18 In contrast, a more recent review demonstrated that a combination of antivirals and corticosteroids for Bell's palsy may have little or no effect on a complete recovery when compared to corticosteroids alone.19 Taken together, there is still debate on the effectiveness of combined antiviral-steroid treatments for acute facial palsy. However, in severe cases, these could still be considered.
Other promising drugs & novel treatments
Nimodipine is a calcium channel blocker which has a neuroprotective effect via the decrease of cellular apoptosis after neuronal injury, and also promotes axonal sprouting at the nodes of Ranvier.20 A recent meta-analysis published in 2019 demonstrated that it significantly increased the likelihood of facial motion recovery.20 However, high-quality evidence justifying the use of nimodipine is still lacking. Low-level laser therapy (LLLT) plus physiotherapy was reported to yield significant improvements when compared with physiotherapy alone.21 The hypothesis for the treatment effects of LLLT is as follows; it enhances the regeneration of neurons and the healing of damaged peripheral nerves; it increases microcirculation by dilating arterial and capillary vessels, and; it enhances cellular function and cell proliferation rates by stimulating the photoreceptors on the mitochondria and cell membranes. In addition, it has anti-inflammatory and inhibitory activities via the decreasing of pro-inflammatory cytokines.21 In an animal study, mycophenolate mofetil, an immunosuppressive drug, was found to be effective for traumatic facial palsy, and is assumed to be available for those who cannot make use of steroidal therapy.22
Eye care
Both the AAO-HNSF guidelines and the Canadian guidelines strongly recommend that eye care should be implemented for the treatment of Bell's palsy.57 For treatment of lagophthalmos after facial palsy, the feasibility of lid loading with gold-weight, autogeneous temporalis fascia and platinum chains has been recently reported.2324
Surgical decompression of the facial nerve
In 1999, Gantz et al.25 advocated surgical decompression medial to the geniculate ganglion be performed within two weeks when ENoG exceeds 90% of degeneration. However, in both the AAO-HNSF guidelines and the Canadian guidelines, no recommendations for surgical decompression for Bell's palsy are made.57 A Cochrane review published in 2013 mentioned the low-quality and insufficient nature of evidence supporting the feasibility of surgical intervention for Bell's palsy.26 In contrast, a recent meta-analysis advocated for surgical decompression, reporting that the rate of complete recovery was higher in those who underwent facial nerve decompression than in the control group.27 However, no differences were shown for those with fair recoveries and failed recoveries in their study.26 Another meta-analysis also reported similar results; middle fossa decompression (MFD) within 14 days of onset yielded better outcomes than MFD after 14 days.28 However, transmastoid decompression did not result in better outcomes.28 For traumatic facial palsy, surgical decompression within two weeks of onset had good results, and surgical exploration within two months lead to acceptable outcomes.29
Acupuncture and physical therapy
Electrostimulation is not recommended in either the AAO-HNSF or the Canadian guidelines.57 In addition, a recent meta-analysis on acupuncture reported insufficient evidence to support the efficacy and safety of acupuncture due to the poor quality and the heterogeneity of relevant research.3031
In the AAO-HNSF guidelines, no recommendations are made in relation to physical therapy other than that physiotherapy for acute illness is specifically not recommended.5 Interestingly though, the Canadian guidelines weakly advocate physiotherapy for chronic patients with persistent weakness.7 A Cochrane review published in 2011 mentioned that facial exercise decreases sequelae in acute cases, though the quality of the evidence was low.32
Muscle & nerve transfer for long-standing facial paralysis
Free functioning muscle transplant has been used for the restoration of smiles in long-standing facial paralysis. The candidates for muscle transfer include the pectoralis minor, latissimus dorsi, serratus anterior, external digitorium brevis, rectus abdominis, and the gracilis.33 In accordance with the donor nerve, a single-stage (using an ipsilateral non-facial cranial nerve, such as the masseter nerve, spinal accessory nerve, or hypoglossal nerve), or a two-stage surgery, which consists of a first-stage cross-facial nerve grafting and a second-stage free muscle transfer, are employed for facial reanimation.33 When comparing single-stage with two-staged operations, single-stage operations have tended to yield better smile reanimations.33
In a recent meta-analysis, gracilis transfer was reported to be effective for regaining oral commissure motion in facial palsy.34 The lengthening of the temporalis myoplasty was reported to be a less extensive procedure than one using the gracilis flap for facial reanimation, while possessing similar results with gracilis flap procedures.35 In addition, masseteric nerve transfer has some merits including the ease of dissection and low morbidity, but spontaneous smile recovery is achieved in only a quarter of patients.36
In a comparative study between VII-to-VII and XII-to-VII coaptation for facial nerve reanimation, XII-to-VII showed a higher probability of functional restoration, but also had higher complication rates and required second-stage surgery.29
Issues with parotidectomy
In a comparative study between harmonic scalpel and electrocautery use during parotidectomy, the former was superior in terms of shorter operation times, less intraoperative blood loss, shorter hospital stays, lower rates of salivary fistula, and less transient facial paralysis.37 For the surgical technique for pleomorphic adenoma and benign parotid tumors, a meta-analysis reported that superficial parotidectomy lead to more frequent facial paralysis as well as higher recurrence rates and more frequent Frey syndrome when compared to extracapsular dissection.38 In contrast, another meta-analysis found no difference in tumor recurrence and the occurrence of permanent facial paralysis between the two techniques.39 For facial nerve dissection during benign parotid surgery, the occurrence of facial nerve paralysis was not seen to differentiate in accordance with which dissection technique was used, be it classical antegrade, or retrograde facial nerve dissection.40
Issues with postparetic synkinesis
One of the most frustrating complications is synkinesis after facial palsy. Its prevalence was reported to be 21.3% in Bell's palsy cases, and in moderate-to-severe synkinesis cases was observed at 6.6%.41 For an assessment of synkinesis, the Sunnybrook facial grading system is most commonly used.42 In an RCT study, a composite score and the symmetry of voluntary movement at one month were predictors for the occurrence of synkinesis.41 For the management of synkinesis, various kinds of options have been tried including botulinum toxin injections, surgery, physical therapy and a combination of botulinum toxin and physical therapy and biofeedback.4143 However, a high level of evidence is still lacking as to what the best treatment options for the management of synkinesis are.42
Patient follow-ups
In the AAO-HNSF guidelines, reassessment by referral to a facial nerve specialist is recommended if there is a worsening of neurological findings at any point, if ocular symptoms develop, or in cases of incomplete recovery three months after onset.5 Similarly, the Canadian guidelines also recommend referral for patients with no improvement or progressive weakness.7 Other randomized trials were not performed during study period.
Go to :
DISCUSSION
In this review, changes in treatment trends in cases of facial palsy have been reviewed for the past ten years. The most prominent change observed may be the move from the conventional House-Brackmann facial nerve grading system to those of Sunnybrook and eFACE. In addition, results of serial meta-analyses reveal that there are now more advocates of surgical decompression of the facial nerve. Beyond steroids or combined steroid-antiviral treatments, various drugs and new treatment options have also been explored. For long-standing facial paralysis and postparetic synkinesis sequelae after facial palsy, facial reanimation has been highlighted and the necessity of new paradigms has been raised.
Taken together, various changes have been made, not only in the facial nerve grading systems, but also in medical treatments, from surgical procedures to rehabilitation, for treatment of acute peripheral facial palsy during the last decade.
Go to :
 XML Download
XML Download