

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
School-aged children and adolescents who have adverse experiences such as school violence, domestic violence, bullying, and sexual abuse are needed for psychosocial intervention.1 Among those children and adolescents who have experienced at least one trauma, 1% to 6% for boys and 3% to 15% of girls develop posttraumatic stress disorder (PTSD).2 For intervention, trauma-focused cognitive behavioral therapy (TF-CBT),3 eye movement desensitization and reprocessing (EMDR), and image rehearsal therapy (IRT) have been provided for trauma therapy.45 TF-CBT6 comprises cognitive processing and reframing, exposure, stress management, and parental treatment. Bilateral EMDR7 stimulation could activate the brain's information processing pathways, enabling more adaptive associations.8 IRT9 provides the patient with a sense of control of nightmares, reducing the frequency and distress associated with traumatic memories.10 Emotional freedom techniques (EFTs) are a form of intervention that draws on various theories of alternative intervention, including neuro-linguistic programming, acupuncture, and energy medicine.11
Stabilization is the foundation of all trauma interventions. According to a Delphi study of mental health professionals that we previously published,4 Psychological First Aid (PFA), Skills for Psychological Recovery (SPR) and Teaching Recovery Techniques (TRT) techniques such as cognitive reappraisal and imaginal exposure were recommended in Korean culture as well as TF-CBT and EMDR. These interventions need to be developed in the context of Korean culture.12 Additionally, it was reported that psychoeducation, normalization, and stabilization of posttraumatic responses should be provided as factors to be addressed in the intervention of children and adolescents after traumatic events.413
In 2015, a stabilization program using a trauma recovery protocol for adults was developed in Korea as part of a study by the National Center of Mental Health, Ministry of Health and Welfare.14 The research team, which developed adult protocols with sufficient clinical experience, comprised multidisciplinary researchers. They searched previous literature, including books, journals, conference handouts, and internet resources, and developed initial stabilizing techniques. The components comprised grounding exercises, containment exercises, distancing, safe place, survival kits, body awareness, EFT, IRT, body techniques, and timeline. They had reviewed the feedback on the usefulness of the techniques from 20 trauma therapists and excluded body awareness, body techniques, and survivor kits. Additionally, they included disposal, resource development, and psychoeducation. The trauma intervention protocol for adults is easily trainable to general therapists rather than trauma specialists and is easily reproducible and trainable.15
In the present study, we revised the trauma recovery intervention for adults14 according to the developmental stage of children and adolescents, and it was named Children in Disaster: Evaluation and Recovery (CIDER) V1.0 protocol for children and adolescents. CIDER is a community-based intervention that helps stabilize trauma response symptoms in children and adolescents and comprises eight sessions. Therefore, we aimed to evaluate the efficacy of CIDER for adolescents exposed to traumatic events.
METHODS
Development process and intervention component of CIDER Protocol V1.0
The research team comprised psychiatrists and a psychology professor with extensive experience in trauma-related intervention and child development. Researchers in this study conducted a study on the Korean Mental Health Technology R&D Project, Ministry of Health and Welfare to develop a trauma intervention protocol for children and adolescents in the study project subset.
The trauma recovery protocol for children and adolescents was named ‘CIDER V 1.0’. The CIDER protocol comprised the therapeutic factors based on TF-CBT,16 EDMR,17 EFT,11 and IRT.18 The CIDER protocol was designed to promote the self-help ability to normalize the psychological responses of children and adolescents, regulating their emotions, managing stress and enhancing coping. Psychoeducation helps children and adolescents understand the effect of the brain and how to treat traumatic reactions.51920 Stabilization skills help regulate the body,2122 which is the foundation of trauma care. Recent research findings support its importance as the most basic and crucial element of trauma therapy.14
The first version of the protocol we revised received comments from therapists and clinical professionals with multiple trauma intervention experiences, followed by consultations and expert feedback. The final contents were constructed and finalized by repeatedly reviewing the elements.
The CIDER protocol comprises eight 50-minute-long sessions with a child and adolescent group. The protocol could be applied to individual or group therapy, and the intervention setting in this study comprised small-group therapy. In-depth counseling of children, youths, families, schools, and communities could be linked through intervention. Each component of CIDER is shown in Table 1.
Table 1
Intervention component of the CIDER V1.0 protocol

The first session focuses on psychoeducation and relaxation techniques. Psychoeducation concerns understanding the brain and psychological symptoms after trauma, and it is the basic element in trauma-related intervention based on the TF-CBT protocol.15 Relaxation techniques such as deep breathing and abdominal breathing are based on EMDR and TF-CBT. The second session comprises relaxation skills using grounding exercises based on the EMDR technique.23 The third session comprises containment exercises based on the EMDR protocol of the child version.24 It could effectively control and self-regulate repetitive invasive memories, images, uncomfortable psychological and body reactions. The fourth session focuses on the taping sequence based on EFT and safe-place exercises based on the EMDR protocol for children.2526 It is an effective and self-regulating technique that helps children and adolescents reduce their discomfort when psychologically unstable. Subsequently, during the fifth session, it comprises the resource development and installation based on the EMDR protocol and TF-CBT, which strengthen their positive resources.17 The sixth session focuses on distancing skills to manage flashback or recurrent images based on the EMDR protocol for adults and children.1727 The seventh session focuses on learning how to manage repeated and uncomfortable dreams and memories by image rehearsal based on IRT.28 During the 8th session, participants review their experience with the CIDER program, imagine the desired future template based on the EMDR and TF-CBT protocols, and increase their understanding of change and growth (Table 1).717
Participants and procedures
From July to December 2017, participants were enrolled from two sites in an alternative school in Korea. These two alternative schools are established for adolescents who need alternative education due to difficulties in social adjustment and peer relationship. The students were mostly adolescents who have had traumatic experiences.29 We recruited adolescents who experienced the traumatic events between the ages of 14 and 19 years.
The inclusion criteria were as follows: participants 1) were between the ages of 8 and 19 years and 2) could understand and respond to the questionnaire. The exclusion criteria were subjects with 1) imminent suicide risk, 2) symptoms of hallucinations or delusions and 3) severe dissociation symptoms.
The researchers provided detailed explanations of the research to the participants and their caregivers. Participants' and parental consents were required. The parental consent form specified details such as the purpose of the study, research method, expected effect, possibility of withdrawing freely after agreeing to participate, human rights protection, and ethics. After determining the potential eligibility through introducing the study, the adolescents and parents provided informed consent/assent and participated in a baseline assessment. The participants understood and answered most of the questionnaire questions during the pre-assessment, however, teachers provided help when students asked. Of the 40 registered students in alternative schools, 24 participated in the study. Finally, 22 participants completed the questionnaire.
In the present study, two clinicians who developed this protocol participated in the study. During the study period, the two clinicians shared and discussed the progress and activities of each session through peer supervision and repeated the discussion to reflect it in the next session. After all sessions were completed, the entire process was analyzed and reviewed.
Measures
Korean Version of Children's Response to Traumatic Events Scale-Revised (K-CRTES-R)
The K-CRTES-R comprises 23 items and assesses intrusion, avoidance and arousal symptoms based on the Diagnostic and Statistical Manual of Mental Disorders-4th Edition (DSM-IV). The subjects should be 6–18 years old complete the questionnaire in 5–10 minutes. The K-CRTES-R deals with psychiatric symptoms from the past seven days and uses a four-point Likert scale with 0 representing “not at all,” 1 denoting “rarely,” 3 denoting “sometimes,” and 5 representing “frequent.” The overall score ranged from 0 to 115.30 In the present study, Cronbach's α was 0.91.
Beck Depression Inventory (BDI)
The BDI, first published in 1961, is a multiple-choice questionnaire self-report inventory. It is one of the most widely used psychometric tests to measure the severity of depression.31 It comprises 21 questions concerning how the subject has been feeling in the last week. Each question has a set of at least four possible responses.32 When the test is scored, a value of 0 to 3 is assigned for each answer, and then the total score is compared with a key to determine depression severity.33 In this study, Cronbach's α was 0.93.
State Anxiety Inventory for Children (SAIC)
The SAIC is a scale used to measure a child's state anxiety level. It is a version of Spielberger's adult state anxiety inventory34 that is transformed into a form that children can understand. State anxiety means a temporary state of anxiety caused by the arousal of the autonomic nervous system in a particular situation. It comprises 20 questions. In this study, Cronbach's α was 0.90.
Data analyses
Statistical analyses were conducted using IBM SPSS Statistics Version Ver. 22.0 (SPSS Inc., Chicago, IL, USA). The demographics of participants were analyzed using descriptive statistics. Cronbach's α was computed. Therefore, changes in the symptoms of trauma response, depression, anxiety, and quality of life from pre- to posttest were evaluated using the Wilcoxon signed-rank test. A P value of < 0.05 was considered to indicate statistical significance.
Ethics statement
The present study protocol was reviewed and approved by the Institutional Review Board of Eulji University Hospital (approval No. EMCS 2015-05-021-011). Informed consent was submitted by all subjects when they were enrolled.
This clinical trial is registered at the Clinical Research Information Service (CRIS, http://cris.nih.go.kr), number KCT0004681.
RESULTS
The demographic characteristics of the participants are shown in Table 2. For the evaluation, the demographic data provided included age, sex, school, psychiatric diagnosis, type of adverse experiences, academic function, and financial status.
Table 2
Demographics of participants (n = 22)
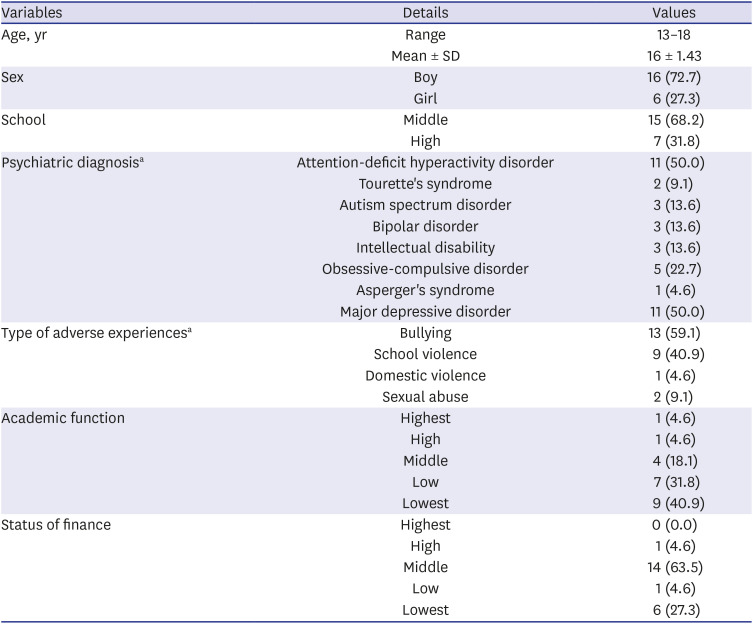
In total, 22 adolescents (mean age, 16 years; standard deviation, 1.43; range, 13–18 years) were recruited in this pilot study. Sixteen (72.7%) respondents were boys, and six (27.3%) respondents were girls. More than 68% (n = 15) of the students were in middle school (grade, 7–8), and 31.8% (n = 7) were high school students (grade, 9–12).
Attention-deficit hyperactivity disorder (ADHD) and major depressive disorder were the most common psychiatric diagnoses exhibited by the students (50.0%, n = 11). Approximately 23% of students presented with obsessive-compulsive disorder (n = 5). Diagnoses of autism spectrum disorder (ASD), bipolar disorder, and intellectual disability were reported by 13.64% (n = 3). Tourette's syndrome and Asperger's syndrome were reported by less than 10%.
The most common experience of adverse events was bullying (59.1%, n = 13). Approximately 41% of students reported experiences of school violence (40.9%, n = 9), followed by sexual abuse (9.1%, n = 2), and domestic violence (4.6%, n = 1).
More than 40% (n = 9) of students reported academic functioning at the lowest level, and more than 60% (n = 14) reported that they were in the middle level of income status (Table 2).
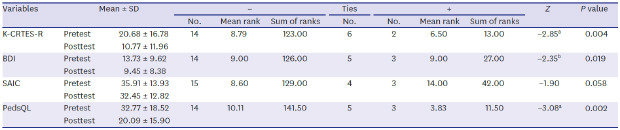
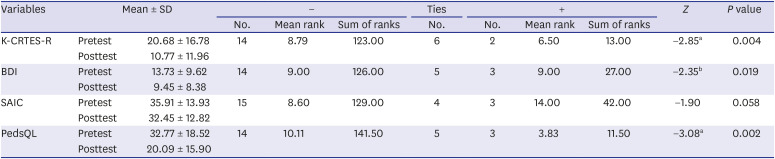
The Wilcoxon signed-rank test revealed a statistically significant improvement in trauma symptoms, depressive symptoms and quality of life as measured by K-CRTES-R (Z = −2.85, P < 0.01), BDI (Z = −2.35, P < 0.05) and PedsQL (Z = −3.08, P < 0.01). However, there was a marginally significant improvement in anxiety symptoms as measured by the SAIC (Z = −1.90, P = 0.058) (Table 3).
Table 3
Analysis of the Wilcoxon signed-rank test of variable changes pre- and posttest (n = 22)
DISCUSSION
The present study aimed to evaluate the feasibility of trauma-focused group therapy for adolescents who experienced traumatic events. Our research team revised the trauma-focused intervention protocol developed as an adult version in Korea by reorganizing the manual to suit the developmental stage of children and adolescents. We observed the feasibility of CIDER as an approach to classroom settings for 22 adolescents who were attending alternative schools that experienced trauma. After the intervention, they showed a significant improvement in trauma-related symptom scores, depressive symptom scores and quality of life scores. Additionally, a marginally significant improvement was found in anxiety symptom scores.
Our results showed a significant improvement in trauma-related symptoms assessed by K-CRTES-R. All the components in the CIDER were aimed to alleviate the trauma symptoms. To explain the effect on the trauma symptoms, we can discuss these elements in detail. First, psychoeducation was aimed to improve the understanding of symptoms and regulate trauma reactions in trauma-experienced individuals. In particular, studies that proved the therapeutic effect of psychoeducation have been reported,143738 and psychoeducation helped to relieve trauma-related symptoms in this study. Second, practicing relaxation skills could decrease trauma response symptoms.39 Reports have supported the effectiveness of stabilization. The patients experiencing childhood abuse showed improvement in trauma symptoms with the stabilization intervention.1440 In the early sessions of CIDER, various relaxation techniques were introduced and practiced, alleviating trauma response symptoms in adolescents who experienced trauma. Third, in addition to the relaxation skill, the CIDER program included components such as imagery exercise and strengthening of their inner resources. Fourth, the protocol was designed to promote self-help ability to normalize the psychological responses of children and adolescents, regulating their emotions, managing stress and enhancing coping and repeated psychoeducation and relaxation skills at the beginning and end of each session, and they were given homework to practice exercises. Therefore, these elements could help reduce trauma response symptoms and promote their self-help ability.
Our result showed significant improvement in depressive symptoms by BDI. Depression is one of the most frequent comorbid conditions with trauma-related disorders.414243 Furthermore, previous researchers have demonstrated high correlations of depressive symptoms and trauma-related symptoms.444546 Many reports have demonstrated that, as trauma symptoms improve, depressive symptoms are also improved.474849505152 Among 32 adolescents (12–18 years) after trauma-focused therapy,53 significant reductions in depressive symptoms were reported as measured by Children's Depression Inventory (CDI) along with the reduction in trauma-related symptoms as measured by The University of California at Los Angeles Posttraumatic Stress Disorder Reaction Index Adolescent version (UCLA PTSD-RI). In the CIDER sessions, it was possible to mitigate negative emotions and improve positive emotions by exploring and visualizing personal resources, supporting resources, and symbol resources. They could experience strengthening expectations and motivation for intervention and coping, as well as increase the efficiency to help cope with stress. Therefore, it seems that the trauma symptoms of participants after the CIDER intervention performed in this study were alleviated, and it was also helpful for the depressive symptoms.
Our results showed a significant improvement in the quality of life assessed by PedsQL. Quality of life is defined in terms of physical, psychological, and social elements of an important concept in health.54 Adolescence is a period of growth characterized by a comparative disturbed quality of life.54 Previous research has found that adolescents exposed to traumatic events were associated with significantly marked deficits in quality of life outcomes compared with the United States norms for healthy adolescents.55 The trauma recovery of physical, emotional, and social functioning encourages the participation of children and adolescents in an active healthy daily life.56 Prior works have found that the psychological status before trauma, age at the time of trauma, and perceived level of social support was predictive of a long-term quality of life.5758 The existing literature showed that social, school, and family support are the key factors in successful social reintegration, psychosocial recovery, and quality of life. In this study, we could speculate that the improvement of trauma response symptoms and depressive symptoms might have contributed to an improved quality of life. Because a trauma-focused intervention ultimately serves the goal of improving the quality of life of adolescents, there is a significant need for research into an adolescent's quality of life. Additionally, future research should consider the psychiatric symptoms and social environment of adolescents when analyzing their quality of life to develop a better understanding.5559
The CIDER program developed in this study is expected to provide safe psychological intervention services to children and adolescents who have experienced trauma. In particular, this protocol can be practically used according to various intervention periods, psychological responses, and developmental stages of children and adolescents after experiencing trauma. Additionally, it could be effectively applied in the field if the personnel engaged in community or clinical intervention in various roles are trained on the main therapeutic contents of the protocol for a certain period. Furthermore, this approach may be used as a guideline for psychological support and trauma-related professional training.14
The limitations of the study are related to the small sample size. Additionally, because four students had ASD, three had bipolar disorder and three had intellectual disabilities in our sample, sample heterogeneity might endanger the appropriate analysis. On the other hand, we can say that it is a real reflection of heterogenetic characters in the alternate school students. When we conduct the intervention in a crisis, we must conduct basic intervention to every student regardless of their prior history of the psychiatric illness. When we conducted this program with these participants under our inclusion/exclusion criteria, their prior psychiatric history did not bring challenges to the participation. Still, further study with a larger sample size and homogenous sample would be needed to generalize the findings of this study. It is difficult to determine the effectiveness because there is no control group, and the improvement of symptoms in this study may not be caused by CIDER but by the passage of time or by meeting a clinician. Furthermore, even if the observed symptom reductions of our findings were due to CIDER, it is unknown the degree to which those reductions were sustained. Therefore, randomized controlled studies with long term follow up are needed.
The results are informative regarding trauma-focused group therapy of school-aged adolescents with trauma. In conclusion, CIDER is the potentially effective intervention for adolescents who experienced adverse experiences and provides significant benefits for trauma-related symptoms as well as depressive symptoms and quality of life. Additionally, further studies are needed to examine whether CIDER is efficacious in treating youth exposed to more severe forms of adversity such as threatened/actual death, serious injury, natural disasters (hurricanes, earthquakes, floods, and fires) or sexual violence and to develop the system adapted to better suit children and adolescents exposed to adverse events.
 XML Download
XML Download