

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Coronavirus disease 2019 (COVID-19), a disease caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), was first detected in December 2019 in Wuhan, Hubei Province, China.1 SARS-CoV-2 is a member of the coronavirus family, which includes the SARS-CoV and the Middle East respiratory syndrome coronavirus (MERS-CoV), both of which caused outbreaks in 2003 and 2015, respectively. COVID-19 is mainly transmitted via respiratory droplets and has been widely and rapidly spreading to other countries outside mainland China since January 2020. As of 19 June 2020, more than 455,000 deaths have been recorded worldwide, and the number of confirmed patients and deaths has been rising.
Several drugs have been administered in an attempt to treat COVID-19, but no treatment guidelines have been established thus far. Drugs such as lopinavir/ritonavir2 and hydroxychloroquine3 have been used since the emergence of the disease without proven benefits. Remdesivir has recently been identified as a promising treatment candidate and has been reported to lower hospitalization and mortality rates.4 However, large-scale clinical studies are needed to establish its efficacy and safety.5 Although many attempts have been made to reposition drugs that can delay the replication or the entry of SARS-CoV-2 into the cell, or for immune modulation, their effects are still difficult to predict.67 In addition, considering the reports on the genetic variations of SARS-CoV-2,8 it is difficult to predict when a vaccine will become available. Therapeutic effects of convalescent plasma (CP) have been reported in various respiratory viral infections.9 As no effective treatment is currently available, CP has also been used for the treatment of COVID-19.101112 However, due to various barriers, CP is not yet widely used in Korea. Here, we describe a case report with CP therapy, and comment on the obstacles in the use of plasma therapy.
Go to : 
CASE DESCRIPTION
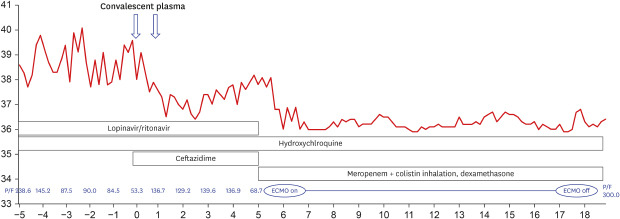
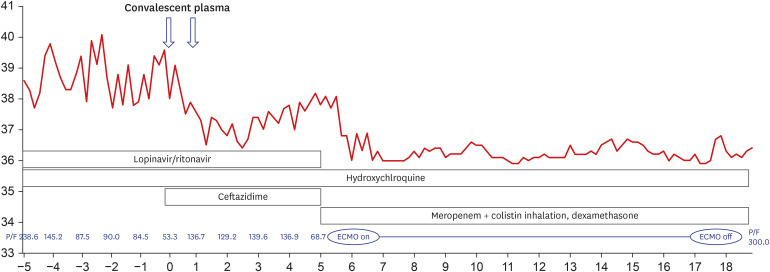
On March 27, 2020, a 68-year-old man came to our hospital for fever that occurred 7 days before admission. He was diagnosed with COVID-19 infection by polymerase chain reaction (AllplexTM 2019-nCoV Assay™; Seegene Co., Seoul, Korea) cycle threshold (CT) value of E gene: 20.1, RdRp: 20.8l, and N: 22.83 from nasopharynx), and although pneumonia could not be detected in the chest roentgenogram (CXR), his body temperature rose to 40°C. From the first day of hospitalization, he received hydroxychloroquine (200 mg every 12 hours) and lopinavir/ritonavir (400/100 mg every 12 hours); pneumonia was detected in his CXR on the third day of hospitalization. His respiratory distress progressed gradually, and a high-flow nasal canula was applied on the 5th day of hospitalization. On the 9th day of hospitalization, his pneumonia had progressed (E gene: 27.71, RdRp: 29.17, and N: 29.98 from nasopharynx; RdRP: 37.08 and N: 35.62 from sputum), and his PaO2/FiO2 ratio had deteriorated to 53. CP transfusion treatment was conducted with mechanical ventilation. His ABO blood group was B (Rh-positive), and he received 250 mL of CP for 2 consecutive days from a donor with ABO blood group A (Rh-positive). The donor's anti-B titer was 1:32. The patient showed clear improvement in respiratory distress and fever symptoms for 3 days after the plasma transfusion. On the third day after plasma transfusion, his PaO2/FiO2 ratio improved to 146, and CXR and fever also improved. There was no evident acute adverse effect of the ABO mismatch. However, 4 days after the plasma transfusion, he presented respiratory distress again. With a sudden oxygen exchange dysfunction, his d-dimer rose to 35.04 μg/mL. As there was no prominent
symptom or laboratory findings that were suggestive of disseminated intravascular coagulation, we initiated intravenous heparin infusion for suspicious pulmonary vein thromboembolism. Colistin inhalation (75 mg every 12 hours) and meropenem (1 gram every 8 hours) were empirically used with extracorporeal membranous oxygenation (ECMO) and dexamethasone (20 mg for 5 days, then 10 mg for 5 days, and tapered in half every 5 days) (Fig. 1). The patient was able to leave after 12 days of ECMO and was discharged without any other complication. When the patient was discharged, all N genes, RdRp, E were not detected in the secretion of the upper respiratory tract. The cut off-value was the 40-CT.
Go to :
DISCUSSION
In this case, the improvement after CP was short-lived, and it was difficult to assess the effects of CP clearly when ECMO, steroid, heparinization, and antibiotic were considered to treat re-exacerbation. However, this experience highlighted several points to be addressed for the widespread use of CP.
In Korea, there was a demand for CP therapy during the outbreak of MERS-CoV in 2015 and COVID-19 in 2020. However, the following problems hindered the widespread application of this therapy: 1) a lack of guidelines, 2) a lack of donors, 3) concerns about adverse effects, and 4) difficulties in matching donors and recipients. Guidelines were recently announced on April 13, 2020, for the use of CP for COVID-19 and were distributed to physicians. Although the number of COVID-19 donors seems sufficient compared to the low number of patients with MERS-CoV during the earlier outbreak, concerns about adverse effects and optimal matching of patients remain unaddressed.
ABO blood group mismatching can be a major problem for whole blood transfusion, but not for plasma transfusion. The most important concern among physicians in the use of CP is transfusion-related acute lung injury (TRALI). TRALI is defined as an acute respiratory distress syndrome that occurs within 6 hours of blood administration.13 Some clinicians have vague concerns about TRALI when performing ABO-mismatch CP, but TRALI is rarely associated with ABO mismatch.14 To reduce TRALI, we recommend avoiding previously pregnant female donors.15 Transfusion-associated circulatory overload is another important complication in CP transfusion. In particular, in severe COVID-19 patients, vascular permeability is increased by cytokines16; hence, it is necessary to be careful about volume overload. In our case, the plasma transfusion was performed over 2 days because of concerns regarding volume overload.
Immediate intravascular hemolytic transfusion reactions (IHTR) are considered the most severe complication of ABO-incompatible plasma transfusion. However, the likelihood of IHTR occurring during a transfusion is estimated to be between 1:2,000 and 1:9,000 in patients with severe systemic diseases, and fatalities are extremely rare.17 Although it is advisable to avoid the transfusion of ABO blood group O plasma to individuals with group AB, there is no official contraindication. Quantitative analysis of anti-A and anti-B should be considered in predicting hemolysis. The isoagglutination test is a method for the evaluation of immunoglobulin M levels,18 with a titer above 1:100 indicating a potential for hemolysis.17
The scheduling of the donor is another challenge in the use of plasma therapy for COVID-19. Currently, fresh liquid plasma is collected from the donor at the recipient’s hospital. However, most donors are young and often cannot visit hospitals because of distance or time constraints. Frozen plasma could be considered as a method to overcome these constraints. Frozen plasma also has the advantage of reducing the delay associated with donor preparation and allows for more flexibility in the timing of administration. It may be helpful to administer early in the disease, before patient's neutralizing antibodies to COVID-19 are produced,19 but there is insufficient CP supply to administer to patients with mild symptoms. Therefore, the onset of the acute exacerbation period should be considered as the time point of CP administration. In particular, the immune modulation effect of CP20 may be beneficial early in the exacerbation process. Frozen storage can help with administering CP at the appropriate time.
The distance between the donor candidate and the patient in need of CP may also be a problem. It is not easy to address distance-related challenges as the current Blood Management Law makes it difficult to collect plasma from a donor in a nearby hospital and send it to the hospital where the patient is located. Therefore, the government needs to modify relevant laws to help facilitate the transport of CP between medical institutions. Eventually, the introduction of systems such as CP banks should be considered.
To date, given the ongoing efforts for mass production of antibodies, there is no randomized controlled study of CP, as it is viewed as a temporary and limited treatment. However, it is necessary to keep in mind that new emerging infectious diseases might spread without established treatments and that CP could again be one of the few available options to fight against a new pathogen.
In conclusion, we recommend the implementation of an effective CP system that can combat COVID-19 and other infectious diseases that may emerge in the future.
Go to :
 XML Download
XML Download