

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Percutaneous coronary interventions (PCI) are globally increasing, hence recurrent ischemia and cardiac events after PCI are also increasing. Thus, strategies for early detection of ischemia and prediction of cardiac events in patients who undergo PCI have been investigated. Functional testing after PCI is not routinely recommended in asymptomatic patients.123 Earlier guidelines recommend that routine functional testing after PCI should be performed in only selected high-risk patients with decreased left ventricular function, multiple-vessel disease (VD), proximal left anterior descending disease, previous sudden cardiac death, diabetes mellitus, hazardous occupations, and suboptimal PCI results.1 Among the various types of functional testing, exercise treadmill testing (ETT) is simple and is widely performed. However, the sensitivity of this test is significantly lower than nuclear and imaging modalities such as single-photon emission computed tomography (SPECT) or exercise echocardiography. Nevertheless, ETT is considered a first option for functional testing due to its cost effectiveness. Initial data from the Routine versus Selective Exercise Treadmill Testing after Angioplasty (ROSETTA) registry showed that routine functional testing after percutaneous transluminal coronary angioplasty is associated with reduced frequency of follow-up clinical events including acute coronary syndrome (ACS) and death.4 However, only 58% of patients who underwent coronary stenting were enrolled in the ROSETTA registry.4 Other studies showed controversial results on the usefulness of early routine ETT and stress imaging tests after PCI for predicting clinical outcomes.5678910 Therefore, we aimed to investigate the clinical utility and implications of early routine ETT. We compared clinical outcomes between ETT positive (+) and ETT negative (−) according to the presence of multi-VD and residual Synergy Between PCI With Taxus and Cardiac Surgery (SYNTAX) score in post-PCI patients from a single-center prospective registry.
Go to : 
METHODS
Study population
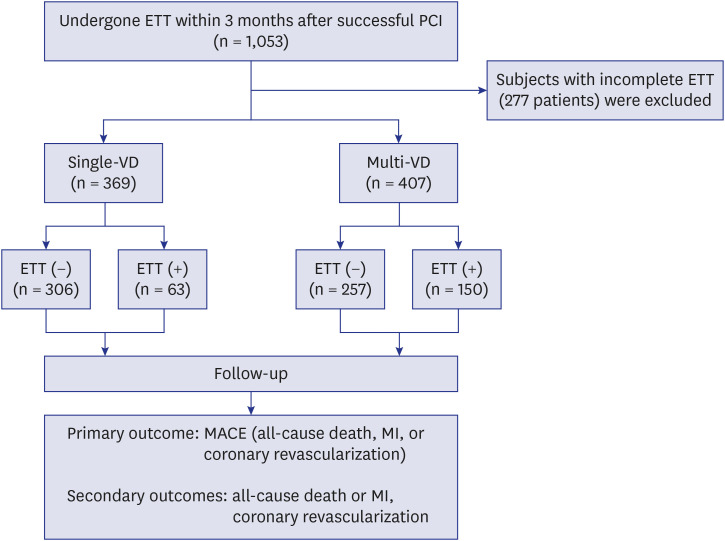
A total of 1,053 patients who underwent ETT within 3 months after successful index PCI from January 2007 to December 2013 at Samsung Medical Center were enrolled and analyzed. Successful PCI was defined as < 20% residual stenosis with thrombolysis in myocardial infarction (TIMI) 3 flow at target lesion. We excluded 277 patients with incomplete ETT. Patients were divided according to single-VD or multi-VD and ETT (+) or ETT (−) (Fig. 1).
Index coronary angiography, PCI, and ETT
PCI was performed according to standardized technique by certificated interventional cardiologist from Korean society of interventional cardiology.2 Implanted drug eluting stents were the Cypher (Cordis Corporation, Johnson & Johnson, Warren, NJ, USA), Taxus (Boston Scientific Corp, Natick, MA, USA), Endeavor, Endeavor Resolute, Endeavor Sprint (Medtronic, Minneapolis, MN, USA), Xience, Xience Prime (Abbott Vascular, Abbott Park, IL, USA), Promus, Promus Element (Boston Scientific Corp), Nobori (Terumo Corporation, Tokyo, Japan), Biomatrix (Biosensors Europe, Morges, Switzerland) or Orsiro (Biotronik, Buelach, Switzerland). A significantly diseased artery was defined as having ≥ 50% stenosis at least one segment at index PCI. Thrombotic occlusion lesions during index PCI were defined as having heavy thrombotic burden requiring suction catheter. To calculate SYNTAX scores, pre-PCI and post-PCI coronary angiograms were analyzed. Each coronary lesion with ≥ 50% stenosis in vessels ≥ 1.5 mm was scored using a previously described algorithm.11 A residual SYNTAX (RS) score was calculated for lesions remaining after PCI.12 All cine coronary angiograms were reviewed and analyzed quantitatively at an angiographic core laboratory (Cardiac and Vascular Center, Samsung Medical Center, Seoul, Korea) using an automated edge-detection system (Centricity CA 1000; GE Healthcare, Waukesha, WI, USA). Two experienced technicians who were blinded to patient information reviewed the cine angiograms; interobserver variability was 0.81 (0.73–0.87), and intraobserver variability was 0.97 (0.97–0.98).
ETT was performed and interpreted according to standard criteria and definitions.113 The standard Bruce protocol was used in patients who reported no limitations in their functional capacity at baseline. The modified Bruce protocol was used in patients with limited functional capacity. Exercise duration, blood pressure, heart rate, functional capacity, and electrocardiographic change with exercise were recorded. ETT results were classified as ETT (+) (electrically positive with or without clinically positive), ETT (−) (electrically and clinically negative), or incomplete (inability to achieve ≥ 85% maximum predicted heart rate with no electrocardiography changes). Electrically, ETT (+) was defined as horizontal or down-sloping ≥ 1 mm ST-segment depression or horizontal or upsloping ≥ 1 mm ST-segment elevation in ≥ 3 consecutive beats. Clinically, ETT (+) was defined as development of angina or angina equivalent during exercise.
Clinical outcomes
The primary outcome was MACE, defined as a composite of all-cause death, myocardial infarction (MI), and coronary revascularization. All-cause death or MI and coronary revascularization were assessed for secondary outcomes. All-cause deaths were considered cardiac unless a definite non-cardiac cause could be established. MI was defined as elevated levels of cardiac enzymes such as troponin I or MB fraction of creatine kinase that was greater than the upper limit of normal range with either ischemic symptoms or electrocardiographic changes implicating ischemia or MI at readmission that required subsequent hospitalization.14 Coronary revascularization was defined as any revascularization of the epicardial coronary arteries by PCI including target lesion revascularization (TLR), non-TLR target vessel revascularization, non-target vessel revascularization, or bypass graft surgery. Clinical, procedural, and outcome data were collected prospectively in our PCI registry by research coordinators. Patients were routinely followed up at 1, 6, and 12 months after the index procedure and annually thereafter. Further information was collected by telephone contact or medical records if necessary. In this study, follow-up was considered complete if mortality was confirmed from the National Population Registry of the Korea National Statistical Office using a unique personal identification number or if the patient was contacted at the planned follow-up interval. All end points were identified by the attending physicians, and reviewed by two authors who had full access to the patient’s clinical and laboratory records. Complicated cases were discussed and adjudicated with two other authors.
Statistical analysis
Categorical variables were expressed as percentage and compared using χ2 or Fisher's exact tests. Continuous variables were presented as mean ± standard deviation (SD) and compared using t-test or Wilcoxon rank sum test. Survival curves were constructed using Kaplan-Meier estimates and compared using the log-rank test. Differences in adjusted risk were evaluated using multivariate Cox regression analysis. Clinically relevant variables included in multivariate models were age, sex, diabetes mellitus, hypertension, previous PCI, chronic total occlusion PCI, thrombotic occlusion PCI, metabolic equivalents of task, and left ventricular ejection fraction. Multivariable logistic regression analysis was performed to determine independent factors associated with ETT (+), starting with a model of clinically relevant factors and covariates, which are P value less than 0.1 in univariable analysis, including age, sex, acute coronary syndrome, diabetes mellitus, hypertension, dyslipidemia, chronic kidney disease, previous PCI, chronic total occlusion PCI, thrombotic occlusion PCI, bifurcation PCI, 2nd-generation drug-eluting stent, multi-VD, and RS score ≤ 8. All p-values were two-tailed, and P < 0.05 was considered statistically significant. SPSS 20.0 (IBM, Armonk, NY, USA) was used for statistical analyses.
Ethics statement
The Samsung Medical Center Institutional Review Board approved this study and waived the requirement for written informed consent for access to an institutional registry (IRB No. 2014-03-012).
Go to :
RESULTS
Baseline clinical, angiographic, and ETT characteristics
Patients were divided into four groups according to single-VD or multi-VD and ETT results: single-VD with ETT (−) (n = 306) or ETT (+) (n = 63) and multi-VD with ETT (−) (n = 257) or ETT (+) (n = 150) (Fig. 1). Baseline clinical characteristics are in Table 1. In multi-VD patients, compared with the ETT (−) group, the ETT (+) group was older. The ETT (+) group had a higher prevalence of previous PCI in both the single-VD and multi-VD patients. Other variables were not significantly different between the ETT (+) and ETT (−) groups in either single-VD or multi-VD patients. Angiographic and procedural characteristics at index PCI are in Table 2. Compared with the ETT (−) group, the ETT (+) group had lower prevalence of thrombotic occlusion lesion during index PCI and higher RS scores in both single-VD and multi-VD patients. In single-VD patients, bifurcation and left main PCI were more frequently performed in the ETT (+) than the ETT (−) group. In multi-VD patients, the ETT (+) group had higher proportions of lesions at the left circumflex artery and more chronic total occlusion lesions; they had higher SYNTAX scores than the ETT (−) group. ETT characteristics after index PCI are in Table 1. The modified Bruce protocol was more frequently used in the ETT (−) group than the ETT (+) group in both single-VD and multi-VD patients. In addition, the Duke treadmill score was significant lower in the ETT (+) group than the ETT (−) group in both single-VD and multi-VD patients. However, the metabolic equivalents of tasks indicating functional capacity were not significantly different between the ETT (+) and ETT (−) groups for both single-VD and multi-VD patients.
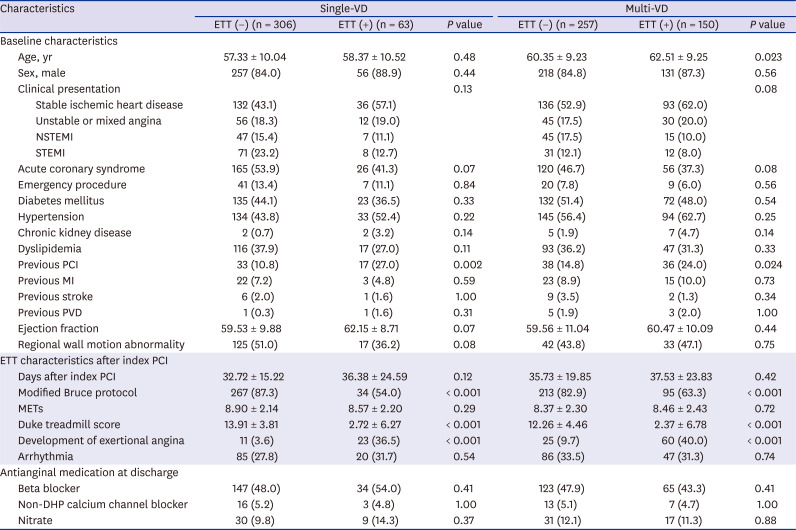
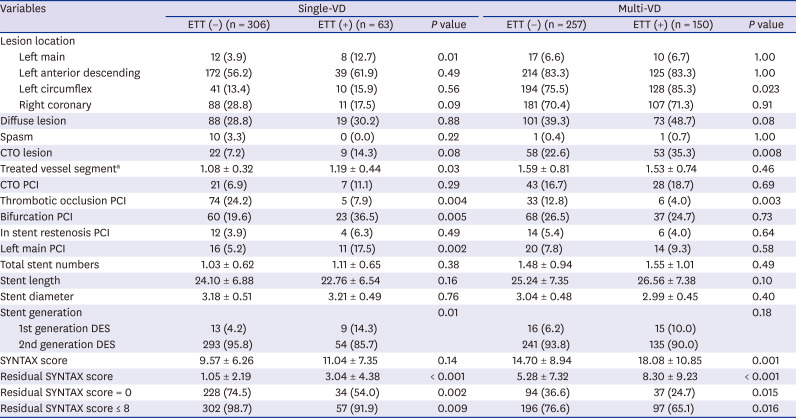
Table 1
Baseline characteristics and exercise treadmill test characteristics after index PCI
Values are mean ± standard deviation or number (%).
PCI = percutaneous coronary intervention, VD = vessel disease, ETT = exercise treadmill testing, NSTEMI = non-ST segment elevation myocardial infarction, STEMI = ST segment elevation myocardial infarction, MI = myocardial infarction, PVD = peripheral vascular disease, METs = metabolic equivalents of task, DHP = dihydropyridine.
![]()
Table 2
Angiographic and procedural characteristics at index PCI
Values are mean ± standard deviation or number (%).
PCI = percutaneous coronary intervention, VD = vessel disease, ETT = exercise treadmill testing, CTO = chronic total occlusion, DES = drug-eluting stent, SYNTAX = Synergy Between PCI With Taxus and Cardiac Surgery.
aTreated vessel segment was defined as stenting or ballooning at left main, left anterior descending, diagonal branch, left circumflex, obtuse marginal branch, right coronary, posterior lateral branch, or posterior descending artery.
![]()
Independent factors associated with ETT (+) and clinical outcomes
In the overall population, independent factors associated with ETT (+) were previous PCI (odds ratio [OR], 1.84; 95% confidence interval [CI], 1.19–2.83; P = 0.006), thrombotic occlusion lesion during index PCI (OR, 0.38; 95% CI, 0.19–0.78; P = 0.008), multi-VD (OR, 2.11; 95% CI, 1.44–3.09; P < 0.001), and RS score ≤ 8 (OR, 0.59; 95% CI, 0.38–0.93; P = 0.02) (Table 3).
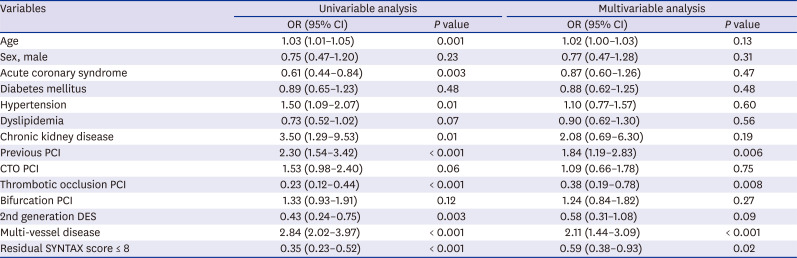
Table 3
Logistic regression analysis for factors associated with ETT positive test
ETT = exercise treadmill testing, OR = odds ratio, CI = confidence interval, PCI = percutaneous coronary intervention, CTO = chronic total occlusion, DES = drug-eluting stent, SYNTAX = Synergy Between PCI With Taxus and Cardiac Surgery.
![]()
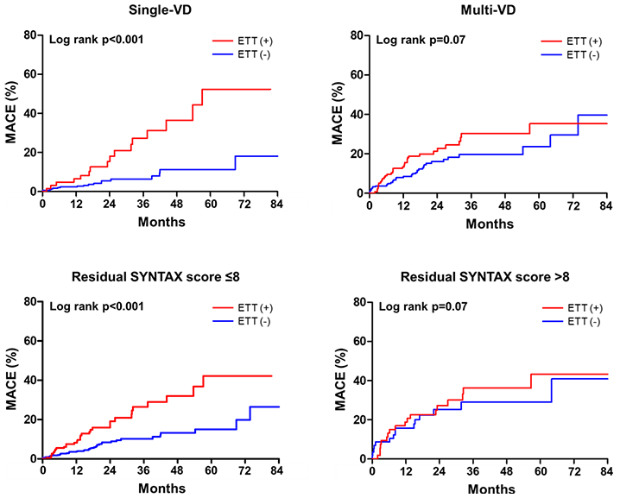
The median follow-up duration was 19.6 months (interquartile range, 15.4 to 33.5 months). In single-VD patients, the ETT (+) group was associated with an increased risk of major adverse cardiac events (MACE) (adjusted hazard ratio [HR], 2.67; 95% CI 1.10–6.49; P = 0.03) (Fig. 2A and Table 4), however not associated (adjusted HR, 1.34; 95% CI, 0.80–2.23; P = 0.26) in multi-VD patients (Fig. 2B and Table 4) compared with the ETT (−) group. The risks for all-cause death or MI and coronary revascularization were not significantly different between the ETT (+) and ETT (−) groups for single-VD or multi-VD patients (Table 4). Similarly, the ETT (+) group was associated with an increased risk of MACE (adjusted HR, 1.90; 95% CI 1.09–3.30; P = 0.02) in patients with RS score ≤ 8 (Fig. 3A and Table 5), however not associated (adjusted HR, 1.22; 95% CI, 0.58–2.57; P = 0.59) in patients with RS score > 8 (Fig. 3B and Table 5) compared with the ETT (−) group. The risks for all-cause death and for MI were not significantly different between the ETT (+) and ETT (−) groups in patients with RS score ≤ 8 or > 8 (Table 5). The event rate of coronary revascularization was significantly increased in the ETT (+) compared with the ETT (−) group in patients with RS score ≤ 8, but not in patients with RS score > 8 (Table 5).


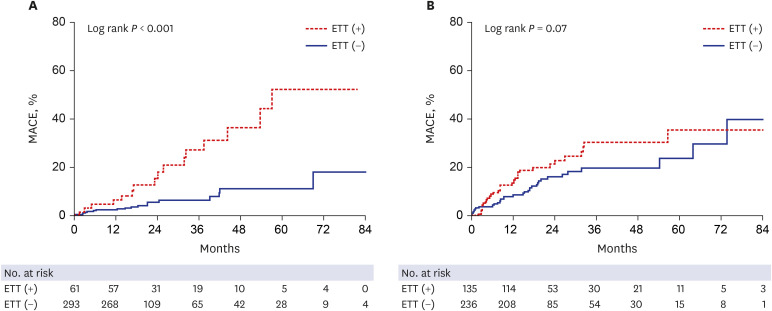 | Fig. 2Kaplan-Meier curves for MACE according to ETT (−) and ETT (+) groups. (A) single-VD and (B) multi-VD.MACE = major adverse cardiac events, ETT = exercise treadmill testing, VD = vessel disease.
|
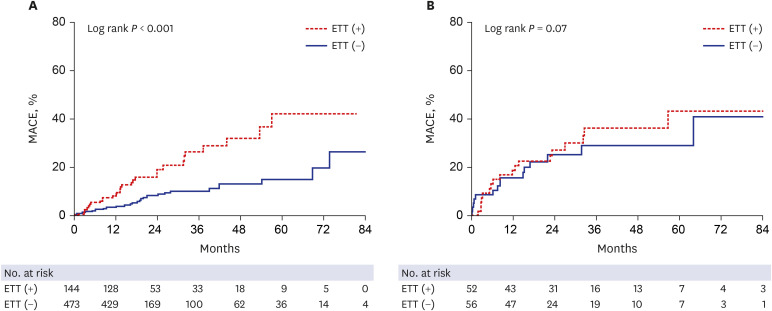 | Fig. 3Kaplan-Meier curves for MACE according to ETT (−) and ETT (+) groups. (A) residual SYNTAX score ≤ 8, or (B) > 8.MACE = major adverse cardiac events, ETT = exercise treadmill testing, PCI = percutaneous coronary intervention, SYNTAX = Synergy Between PCI With Taxus and Cardiac Surgery.
|
Table 4
Clinical outcomes according to single- and multi-VD
Values are expressed as number (%, Kaplan-Meier estimates).
VD = vessel disease, ETT = exercise treadmill testing, HR = hazard ratio, CI = confidence interval.
aAdjusted for age, sex, diabetes mellitus, hypertension, previous PCI, chronic total occlusion PCI, thrombotic occlusion PCI, metabolic equivalents of task, and left ventricular ejection fraction.
![]()
Table 5
Clinical outcomes according to residual SYNTAX score ≤ 8 and > 8
Values are expressed as number (%, Kaplan-Meier estimates).
SYNTAX = Synergy Between PCI With Taxus and Cardiac Surgery, ETT = exercise treadmill testing, HR = hazard ratio, CI = confidence interval.
aAdjusted for age, sex, diabetes mellitus, hypertension, previous PCI, chronic total occlusion PCI, thrombotic occlusion PCI, metabolic equivalents of task, and left ventricular ejection fraction.
![]()
Go to :
DISCUSSION
We investigated the clinical implications of early routine ETT in asymptomatic patients who underwent PCI. We found that previous PCI history, absence of thrombotic occlusion lesion during index PCI, multi-VD, and RS score > 8 were independently associated with early routine ETT (+). Furthermore, we showed that, compared with the ETT (−) group, the ETT (+) group was associated with increased risk of MACE in patients with single-VD and RS score ≤ 8, but not in patients with multi-VD and RS score > 8.
Whether routine early ETT has prognostic value for predicting clinical events after PCI remains unclear. Previous studies investigating the role ETT after PCI showed that it may predict restenosis, but most other observational studies suggest that it does not. The current American College of Cardiology/American Heart Association guidelines for exercise stress testing state that routine early ETT after PCI is not indicated. However, evidence on the clinical utility of early ETT after PCI in the stenting era, especially after drug-eluting stent implantation, is lacking. To the best of our knowledge, this study included the largest number of patients for evaluating the clinical impact of early routine ETT after PCI in the drug-eluting stent era. Our study suggested that ETT results might be interpreted differently according to high-risk factors and ischemic burdens such as multi-VD and RS score. Our data showed that, compared with the ETT (−) group, the ETT (+) group was associated with increased risk of MACE in single-VD patients, but not in multi-VD patients. Generally, multi-VD is a high risk of restenosis after PCI; it was considered routine ETT according to previous guidelines.1 However, previous data from the ROSETTA registry showed that routine functional testing is not associated with significant benefits during a 6-month follow-up of patients after multi-VD PCI15 and these findings are consistent with our result. Therefore, previous and our data indicated that early routine ETT may not be useful in multi-VD patients.
In addition, previous studies demonstrated that RS score > 8 is associated with worse clinical outcome,16 therefore we determined the RS score cut-off value of 8 in this study. Our data indicated that, compared with the ETT (−) group, the ETT (+) group was associated with increased risk of MACE in patients with RS score ≤ 8, but not in patients with RS score > 8. If single-VD or multi-VD reflect existing ischemic burden and RS score reflects remnant ischemic burden, our data suggested that early routine ETT after PCI may not be helpful in patients above a certain ischemic burden.
We showed that the ETT (+) group was associated with increased risk of a composite outcome for MACE in patients with single-VD and RS score ≤ 8. This result was mainly due to increased coronary revascularization. Although the ETT (+) group had increased risks of all-cause death or MI in single-VD patients, the increases were not statistically significant. Similarly, a previous report showed that early positive ETT results might be associated with soft endpoints such as diagnosis of unstable angina and a higher rate of repeat cardiac procedures. Early positive ETT results, however, were a poorer predictor of the hard endpoints of death and MI.5 Therefore, previous work and our data suggested that the results of an early routine ETT after PCI might be helpful mainly for predicting coronary revascularization.
In our study, previous PCI history, absence of thrombotic occlusion lesion during index PCI, multi-VD, and RS score > 8 were independently associated with early routine ETT (+). In contrast to other predictors that represent large, existing, and remnant ischemic burden, absence of thrombotic occlusion lesions during index PCI was also an independent predictor of ETT (+). We interpreted this result as indicating that although acute thrombotic occlusion lesions were seen during index PCI, rapid resolution of thrombotic occlusion might not have affected remnant ischemic burden. Therefore, our data suggested that remnant chronic atherosclerotic lesions might be important for affecting ETT results after PCI.
Our study has several limitations. First, the nonrandomized nature of the registry data could have resulted in selection bias. This study might not be representative of the study population because only 10% of the total patients were included in this analysis, and it might be underpowered to confirm the efficacy of early routine ETT due to the small sample size of each group. Furthermore, the selection of treatment strategy and conduction of ETT after PCI were influenced by patient characteristics and patient and doctor preferences. Second, our data showed that a considerable number of patients (27.3% of the total population) were ETT (+) within 3 months after PCI. Because ETT has only 75% specificity and about 80% sensitivity, a certain number of patients with false-positive results might be included among the ETT (+) patients. Third, coronary revascularization is a soft end point and depends on physician's discretion. In real-world practice, ETT (+) in patients with single-VD or RS score ≤ 8 may have led physicians to perform coronary angiography to identify a recurrence of target lesion, but not in patients with multi-VD and RS score > 8. Because the result of ETT in patients with multi-VD and RS score > 8 might be mainly affected by residual ischemia rather than a recurrence of treatment lesions, we suspect that the physician did not determine coronary angiography based on the result of ETT. Thus, ETT (+) in patients with single-VD or RS score ≤ 8 might be associated with the occurrence of MACE, but not in multi-VD patients with RS score > 8. Finally, evaluating remnant ischemia after PCI by using only ETT might be difficult, especially in patients with multi-VD. To determine the exact remnant ischemia after PCI, further invasive or imaging modalities such as functional fractional reserve, stress echocardiography, and SPECT might be performed simultaneously with ETT in a large-population study.
In conclusion, early routine ETT after PCI predicts MACE mainly due to coronary revascularization in patients with single-VD and RS score ≤ 8 rather than multi-VD and RS score > 8. Therefore, early routine ETT after PCI might be considered in selected patients who are suspicious of having an anatomically lower ischemic burden.
Go to :
 XML Download
XML Download