

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Parkinson's disease (PD) and essential tremor are common neurological disorders associated with tremors. The estimated prevalence of the disorders, with a lower frequency in PD, has ranged from 0.4% to 5% of the global population.12 In the Korean population, the prevalence of PD among individuals aged 65 and older has been reported to be 0.4%,3 while that of essential tremor was 3.6%.4 Unlike patients with essential tremor, those with PD present with asymmetric rest tremor, and nearly all of them have one or more non-motor symptoms (NMS).56 Certain NMS, such as olfactory dysfunction, rapid eye movement (REM) sleep behavior disorder (RBD), depression, constipation, and pain can even antedate the development of motor symptoms of PD.56 Although not yet confirmed, Braak's7 hypothesis illustrates NMS preceding the motor signs of PD; α-synuclein and its aggregates called Lewy bodies, the principle pathology of PD, form in the olfactory bulbs and the lower brainstem involving the dorsal motor nucleus of the vagus, nucleus ambiguous, raphe nucleus, and locus coeruleus, thereby affecting olfactory and autonomic functions as well as sleep. These structures correspond to Braak stages I–II and may precede the motor manifestations that are resulted from ascending pathology reaching the midbrain (Braak stage III).7 The pathology also extends into the peripheral autonomic nervous system, thereby affecting cardiovascular and gastrointestinal functions.8 In terms of neurotransmitters, degeneration of dopaminergic, serotonergic, and cholinergic neurons in the central, peripheral, and autonomous nervous systems are implicated in the mechanism of NMS in PD.6910 This evidence suggesting multisystem involvement may account for various non-motor phenomena of PD. Moreover, the multifactorial causes may be responsible for non-responsiveness to levodopa in the treatment of NMS, unlike motor symptoms of PD.911 This article reviews diverse NMS of PD manifesting as multiple organ dysfunction aside from typical neurological or neuropsychological presentations. For neuropsychological presentations, such as cognitive dysfunction, dementia, depression, anxiety, and psychosis, we have published a review article in the previous issue of this journal,12 and the current article concentrates on NMS in other fields than cognitive and psychiatric problems. This article will be useful for physicians to recognize the necessity of a multidisciplinary and collaborative approach for the management of patients with PD.
Go to : 
SLEEP DISORDERS
Sleep disturbances are one of the most common NMS in PD, affecting 60%–90% of the patients.61314 The spectrum of sleep disorders in PD varies (Table 1); insomnia, excessive daytime somnolence (EDS), RBD, non-REM parasomnias, restless legs syndrome (RLS), and periodic leg movements in sleep (PLMS) are sleep disorders causing sleep disturbances in patients with PD.61314 The pathophysiology of sleep disturbances in PD is attributed to neurodegenerative changes (α-synuclein and Lewy body formation) in the brainstem areas, such as the raphe nucleus and locus coeruleus.15 The degeneration of these nuclei that play a significant role in thalamocortical arousal and the sleep-wake cycle can lead to the disruption of sleep architecture, thereby manifesting insomnia, EDS, and parasomnias in patients with PD.1516 Insomnia including difficulty falling asleep, sleep fragmentation, and frequent awakenings occurs in 40%–80% of patients with PD.1417 In the sleep structures, underactivity of the ventrolateral preoptic area (sleep-promoter) and overactivity of the hypocretin neurons in the hypothalamus (wake-promotor) have been implicated in the development of insomnia in patients with PD.18 Upregulation of arousal systems including serotonergic, noradrenergic, and cholinergic neurons in the brainstem nuclei is also suggested to contribute to insomnia.19 In addition to this, motor disability and some NMS of PD, such as nocturnal akinesia, dystonia, pain, nocturia, depression or anxiety, RLS, and respiratory disorders can contribute to sleep maintenance problems in patients with PD.20 On the other hand, excessive sleepiness during the daytime occurs in 20%–50% of patients with PD.2122 EDS and involuntary dozing result from damage to the arousal system, presumably due to hypothalamic hypocretin cell loss and impairment in the above-mentioned brainstem nuclei that serve to maintain wakefulness.19 Furthermore, disrupted nighttime sleep, cognitive impairment, depression, and anti-parkinsonian drugs can contribute to the daytime somnolence.2123 In particular, dopamine agonists may have an important role in the development of EDS and sleep attacks.2425 RBD, characterized by vocalizations and/or dream-enactment behavior (e.g., talking, shouting, punching, or kicking) during REM sleep occurs in about a third of patients with PD.26 In longitudinal studies, up to 50% of patients showed RBD heralding the motor symptoms of PD.262728 The pathogenesis of RBD in PD is thought to be caused by α-synuclein pathology involving REM sleep generation in the brainstem, especially the sublaterodorsal nucleus, magnocellular reticular formation, and peri-locus coeruleus area.2930 Because these REM sleep structures are connected to dopamine neurons in the ventral tegmental area, a dopaminergic deficit has also been suggested to be related to RBD in patients with PD.15 Non-REM parasomnias, such as vivid dreams, nightmares, night terrors, nocturnal hallucinations, confusional arousals or arousal-related episodes mimicking RBD can also occur in patients with PD.3132 The cholinergic changes in the brainstem and brainstem-subcortical circuits have been implicated in the development of parasomnias in patients with PD.3133 Certain drugs that include selective serotonin reuptake inhibitor, serotonin-norepinephrine reuptake inhibitor, and tricyclic antidepressant can trigger both RBD and non-REM parasomnias.34 RLS, characterized by uncomfortable sensations in the legs, an urge to move, and a transitory decrease after moving, as well as PLMS, rhythmical extension of the big toe and dorsiflexion of the ankle, have been reported in 15%–20% of patients with PD.35 Although it is debatable, dysregulated circadian patterns in the dopaminergic system may influence the development of RLS and PLMS.1536 Impaired central dopaminergic transmission has also been suggested to be involved, with evidence of the efficacy of dopaminergic drugs in the treatment of RLS and PLMS.373839 The prevalence of obstructive sleep apnea in patients with PD ranges 20%–60%.204041 Although a few studies have demonstrated that its prevalence in patients with PD is similar to that of the general population, incoordination of respiratory muscle, autonomic dysfunction, and reduced respiratory drive in PD have been suggested to contribute to the obstructive sleep apnea.204041
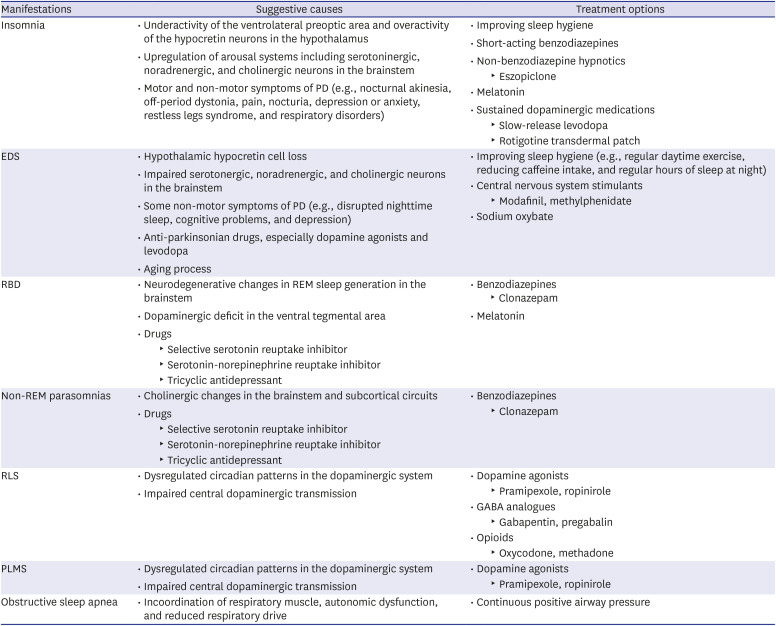
Table 1
Sleep disorders in PD
PD = Parkinson's disease, REM = rapid eye movement, RBD = rapid eye movement sleep behavior disorder, GABA = gamma-aminobutyric acid, EDS = excessive daytime somnolence, RLS = restless legs syndrome, PLMS = periodic leg movements in sleep.
![]()
Before initiating pharmacological treatment, the above-mentioned potential contributors that have a secondary effect on sleep, such as comorbid NMS or drug-induced sleep disorders should be ruled out. Then, insomnia may be improved with good sleep hygiene, administration of short-acting benzodiazepines, non-benzodiazepine hypnotics (eszopiclone), and melatonin (Table 1).114142 Sustained dopaminergic stimulation by using slow-release levodopa or long-acting dopaminergic agonists (rotigotine patch) may also improve insomnia as well as nighttime motor symptoms of PD.114143 EDS may be managed by improving sleep hygiene, for example, regular daytime exercise, reducing caffeine intake, and regular hours of sleep at night.1141 If these are not effective, wake-promoting agents (modafinil and methylphenidate) or sodium oxybate can be used.114144 For the treatment of RBD and parasomnias, clonazepam is usually used as the first-line therapy.41 Melatonin, in combination with clonazepam can also be useful for symptoms of RBD.1141 Additionally, it is important to maintain a safe bedroom and to remove potentially dangerous objects that might injure the patients during dream enactment.41 Both RLS and PLMS symptoms can be relieved by low doses of dopamine agonists (pramipexole and ropinirole).41 Furthermore, gamma-aminobutyric acid (GABA) analogues (gabapentin and pregabalin) or opioids (oxycodone and methadone) can also be used as treatments for RLS.41 The gold standard therapy for obstructive sleep apnea is continuous positive airway pressure, which can improve nighttime oxygenation and sleep maintenance.45
Go to :
OCULAR DISORDERS
Patients with PD may experience ocular surface irritation such as burning or gritty sensation, intermittent tearing, blurred vision or red eyes caused by dry eye syndrome, and blepharitis (Table 2).46 The estimated prevalence of dry eyes and blepharitis in patients with PD are approximately 60% and 20%, respectively.4647 This is attributed to decreased blink rates and considered as a form of hypokinesia in patients with PD.4849 Another contributor is decreased tear production in PD, caused by dysfunction of the parasympathetic nerves that innervate the lacrimal gland.50 Diplopia has been reported in 10%–30% of patients with PD.4651 This is caused mainly due to convergence insufficiency, characterized by failure of convergence and exotropia while fixating on a near object, and blurred vision during reading and near tasks.4751 Diplopia might be associated with levodopa-related motor fluctuations, which has been observed during end-of-dose “off” period and has been improved with dopaminergic medication, albeit with unclear etiology.4751 Other oculomotor abnormalities, occurring in patients with PD are impairment of saccadic and smooth pursuit eye movements, which has been reported in up to 75% of patients with PD,52 square wave jerks, and ocular oscillations.5354 Patients with PD could exhibit blurred vision due to dry eyes, accommodation disorders, or medications that include anticholinergics and monoamine oxidase inhibitors (selegiline and rasagiline).51 In addition, an N-methyl-D-aspartate-receptor antagonist (amantadine) can cause blurry vision as a result of corneal endothelial edema.51 Blepharospasm is usually found in patients with advanced PD, which has been reported in 1%–13% of patients with PD.5556 While blepharospasm is believed to be related to a loss of inhibition within the sensorimotor cortico-basal ganglia, ocular surface irritation with dry eyes may partly contribute to paradoxical excessive blinking.465556 Contrast sensitivity, the ability to distinguish subtle differences of an object from its background at low contrast, and color discrimination are both commonly impaired early in the course of the disease, although the exact prevalence is not known.5157 Deficiency of retinal dopamine or deficits in the primary visual pathway have been suggested as causes of diminished color discrimination and contrast sensitivity.575859 Stereopsis, the ability to perceive a three-dimensional image by both eyes, is also impaired early in the disease and is associated with visuospatial impairments in patients with PD, of which pathophysiology might be related to non-dominant extrastriate cortical atrophy.6061 The presence of visual hallucinations has been found in up to 60% of patients with PD,6263 and may occur spontaneously with multifactorial contributors, being associated with decreased visual acuity as in Charles Bonnet syndrome, impaired color discrimination and contrast sensitivity, and cognitive impairment.6465 In addition, several anti-parkinsonian medications, such as anticholinergics, dopamine agonists, levodopa, amantadine, and monoamine oxidase inhibitors can exacerbate visual hallucinations.51
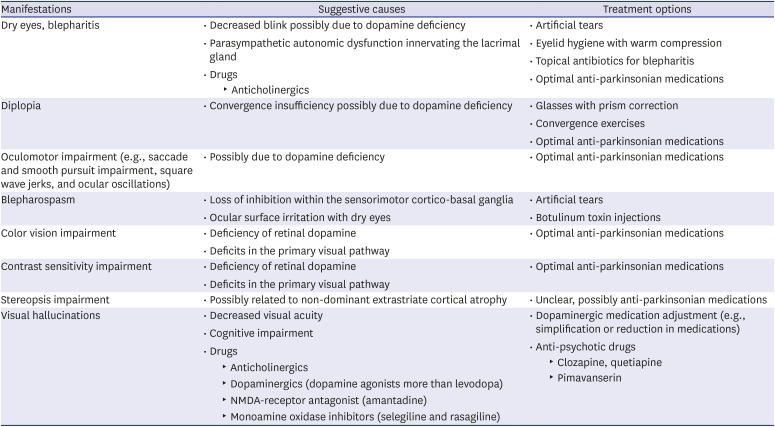
Table 2
Ocular disorders in PD
![]()
The treatment of ocular disorders depends on symptomatology (Table 2). Artificial tears to provide corneal lubrication for dry eyes as well as eyelid hygiene with warm compression and topical antibiotics for blepharitis can be helpful.46 Diplopia due to convergence insufficiency can be corrected with base-in prisms or convergence exercises.4751 Improvements in smooth pursuit eye movements and convergence have been observed with the use of dopaminergic drugs.66 Blepharospasm can be relieved by botulinum toxin injections if it is not relieved with artificial tears or if ocular surface irritation persists.464751 Impaired color discrimination, contrast sensitivity, and stereopsis may be improved with dopaminergic therapy although the improvements are variable.596167 Visual hallucinations do not always require dose reduction of dopaminergic drugs because of an unacceptable increase in motor disability.46 However, in cases of distressing visual hallucinations, a simplification or reduction in antiparkinsonian medications may be effective, and further treatments with anti-psychotic drugs (clozapine and quetiapine) or recently developed serotonergic drug (pimavanserin) may need to be considered.1112
Go to :
NOSE, MOUTH, AND THROAT DISORDERS
Olfactory dysfunction causing hyposmia or anosmia (Table 3) occurs in 70%–90% of patients with PD.6869 This has been shown to be associated with α-synuclein pathology in the olfactory bulbs, olfactory tract, and olfactory nuclei, as previously discussed in Braak's hypothesis.770 A decrease in dopaminergic input from the ventral tegmentum to the olfactory tubercle and a decrease of dopaminergic neurons in the olfactory bulb are also related to olfactory dysfunction in PD.6871 Ageusia (loss of taste) has also been reported in patients with PD at varying frequencies ranging 9%–54%,7273 but its pathophysiology remains unclear. Unlike the pathogenesis of olfactory dysfunction, the gustatory nucleus in the brainstem of patients with PD showed an absence of α-synuclein pathology, even in those with late-stage PD.7 However, taste receptor genes have been found to be dysregulated in patients with PD.74 Dribbling of saliva from the corner of the mouth occurs in 35%–75% of patients with PD, which is caused by infrequent swallowing, as a result of reduced activity of the epiglottis and decreased motor coordination for swallowing.75 This results in angular cheilitis and foul odor.7677 Furthermore, difficulties in maintaining oral hygiene due to motor disability and neurocognitive or affective symptoms (e.g., dementia, apathy, or depression) increase the chances of periodontal diseases.7677 Xerostomia (dry mouth) due to decreased salivary production is also reported in up to 60% of patients with PD.78 This is a likely autonomic symptom of patients with PD, with supportive evidence of salivary gland involvement by α-synuclein pathology.7980 Dysphagia can occur in patients with PD, especially in those with a late stage of the disease.81 More than 80% of patients with PD develop dysphagia during the course of the disease,81 and a study reported that around one-third of patients with PD aspirated silently.75 This has been attributed to pharyngoesophageal motor abnormalities.8182
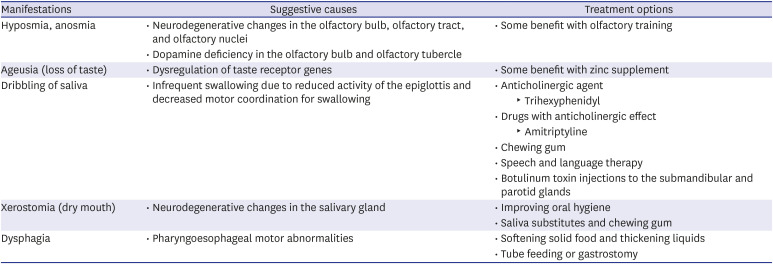
Table 3
Nose, mouth, and throat disorders in PD
![]()
Unlike other NMS, olfactory dysfunction and ageusia do not respond to anti-parkinsonian or other medications (Table 3). Olfactory training has been shown to improve olfactory dysfunction,83 and zinc supplementation provided some benefits in those with age-related taste dysfunction.84 However, there are currently no cures for patients with PD who have olfactory dysfunction and ageusia. For symptoms of excessive drooling, there are several treatment options including anticholinergics (trihexyphenidyl) or drugs with anticholinergic effects (e.g., amitriptyline); however, these drugs may cause xerostomia or other adverse effects such as constipation, urinary retention, memory impairment, and hallucinations.1085 Other options include chewing gum, and speech and language therapy.1085 Injection of botulinum toxin to the submandibular and parotid glands has been shown to improve drooling.85 To manage dysphagia, softening solid foods and thickening liquids before consumption may help, but in patients with advanced stages of the disease, tube feeding or gastrostomy may be needed.86
Go to :
CARDIOVASCULAR DISORDERS
Cardiovascular autonomic dysfunction, specifically orthostatic hypotension, blood pressure variability, and heart rate variability, is commonly observed in patients with PD (Table 4).8788 Orthostatic hypotension, defined as at least a 20 mmHg decrease in systolic pressure and/or 10mmHg decrease in diastolic pressure within three minutes of standing, is the most well-known autonomic symptom, occurring in 20%–60% of patients with PD.89 Those symptoms of dysautonomia are likely due to dysfunction of the central nuclei (dorsal motor nucleus of the vagus, nucleus ambiguous, and other medullary nuclei) located at the lower brainstem, which controls the sympathetic preganglionic neurons.90 Dysfunction of the peripheral, postganglionic sympathetic nerves also contributes to cardiac and extra-cardiac noradrenergic denervation as well as failure of the arterial baroreflex.91 Furthermore, it can also be triggered by antiparkinsonian medications including levodopa, dopamine agonists, and monoamine oxidase inhibitors (selegiline and rasagiline).92
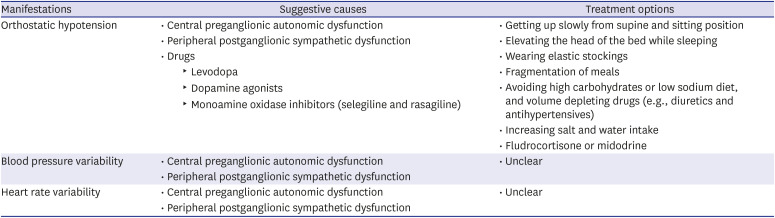
Table 4
Cardiovascular disorders in PD
![]()
Recommendations for patients with orthostatic hypotension include standing up gradually in order to decrease sudden blood pressure changes, sleep with head-up position, wearing elastic stockings, fragmentation of meals, avoidance of high-carbohydrate foods, cautious use of volume-depleting drugs (e.g., diuretics or antihypertensives), and increasing salt and water intake (Table 4).93 In severe cases, medications such as fludrocortisone or midodrine may be needed to improve postural hypotension.93 However, drugs acting on postsynaptic adrenoreceptors should be used in consideration of underlying cardiovascular diseases and supine arterial hypertension.93 On the other hand, treatment for blood pressure variability and heart rate variability remains uncertain.8788
Go to :
SKIN DISORDERS
Sweating disorders consisting of hyperhidrosis, and to a lesser extent, hypohidrosis can be seen in patients with PD (Table 5).9495 The estimated prevalence of hyperhidrosis ranges 20%–60% in patients with PD, and that of hypohidrosis is less than 40%.9495 Dopamine deficiency has been suggested as a mechanism of sweating disorders in patients with PD based on the fact that dopamine is one of the neurotransmitters in hypothalamus-driven thermoregulation.9697 Moreover, fluctuating hyperhidrosis in patients with PD is often associated motor fluctuations, and modulating dopaminergic medication has been shown to be effective for the symptom.9697 Axial hyperhidrosis, which can be observed in patients with PD is explained as compensatory mechanism for reduced sympathetic function in the extremities, leading to hypohidrosis in the hands and feet.95 In addition, the cutaneous autonomic nerves that innervate sweat glands have been found to be affected by α-synuclein pathology.9899

Table 5
Skin disorders in PD
![]()
For hyperhidrosis, non-pharmacological interventions, such as avoiding hot and humid environments and foods that may trigger sweating, wearing well-ventilated clothes, and staying well-hydrated can be beneficial (Table 5).95 Sweating disorders related to motor complications can be managed by optimizing dopaminergic medications.9495 Anticholinergics are often considered for excessive sweating, but its effectiveness is limited and controversial.95
Go to :
GASTROINTESTINAL DISORDERS
Gastrointestinal symptoms, including heartburn, nausea, vomiting, and constipation, are common NMS of PD (Table 6). Among them, constipation is the most frequently encountered problem, occurring in 50%–60% of patients with PD.10 These gastrointestinal hypomotility symptoms are thought to be derived from parasympathetic autonomic dysfunction due to damaged dorsal motor nucleus of the vagus nerve in the brainstem along with α-synuclein pathology in the peripheral autonomic ganglia and enteric nervous system.100101 Drugs with anticholinergic effects, such as anticholinergics, tricyclic antidepressants, and opiates, may secondarily worsen bowel hypomotility, manifesting as constipation.1085
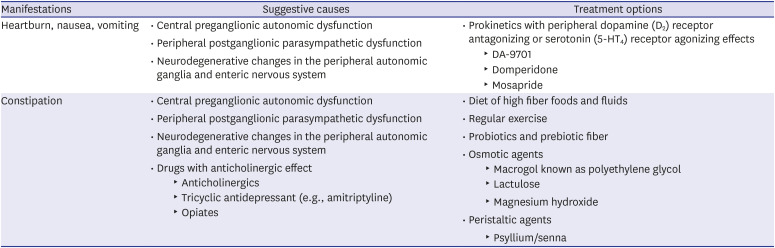
Table 6
Gastrointestinal disorders in PD
![]()
Heartburn, nausea, or vomiting can be improved by prokinetics having peripheral dopamine (D2) receptor antagonizing or serotonin (5-HT4) receptor agonizing effects, such as domperidone and mosapride (Table 6).102 A recent study has shown that DA-9701, a novel prokinetic drug, can be useful in patients with PD by enhancing gastric motility without aggravating PD symptoms.103 In contrast, certain prokinetics, such as levosulpiride, metoclopramide, and clebopride, which act on the central D2 receptor, can worsen motor symptoms of PD.104 Constipation can be improved by diet with high fiber foods and fluids along with regular exercise.11105 The use of probiotics and prebiotic fibers can be helpful for bowel mobility.11105 If these are ineffective, laxatives such as osmotic agents or peristaltic agents (e.g., macrogol, lactulose, or magnesium hydroxide) can be used.11105
Go to :
GENITOURINARY DISORDERS
Lower urinary tract symptoms including urinary frequency, nocturia, urgency, and incontinence have been reported in approximately one-half of patients with PD (Table 7).106107108 These overactive bladder symptoms in patients with PD are thought to be caused by an altered dopamine-basal ganglia circuit in the urinary system since basal ganglia has an inhibitory effect on micturition.109110111 Additionally, about two-thirds of patients with PD who exhibit urinary symptoms have urodynamically defined impaired detrusor contractility, resulting in voiding phase symptoms such as weak stream, hesitancy, and feelings of incomplete voiding.112 Symptoms of sexual dysfunction including decrease in libido, erectile dysfunction in males, and decrease in lubrication in females are also frequent NMS, occurring in one-half to two-thirds of patients with PD.111113114115116 Hypothalamic dysfunction due to altered dopamine-oxytocin circuit is thought to be responsible for the sexual dysfunction in PD because oxytocinergic neurons in the hypothalamus inhibit prolactinergic neurons that have an inhibitory effect on sexual function.111117 Symptoms of depression also play a role in sexual dysfunction in patients with PD.118 In contrast, hypersexuality or aberrant sexual behaviors can be present in susceptible patients with PD, which is linked to dopaminergic drugs, especially dopamine agonists.118
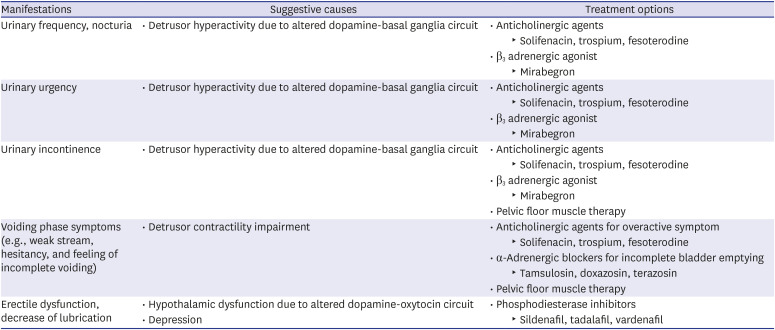
Table 7
Genitourinary disorders in PD
![]()
Despite the dopaminergic pathophysiology above, overactive bladder symptoms do not respond to levodopa therapy (Table 7).11111 Anticholinergics (solifenacin, trospium, or fesoterodine) are generally used as a first-line treatment, but they should be cautiously used particularly among elderly patients with psychiatric symptoms or cognitive decline.11111 For these patients who have an overactive bladder, mirabegron, which is a β3 adrenergic agonist, is an alternative therapeutic option.11111 α-Adrenergic blockers (tamsulosin, doxazosin, or terazosin) can be used for the sensation of incomplete bladder emptying and an intermittent urinary stream.111119 Phosphodiesterase inhibitors (sildenafil, tadalafil, or vardenafil) are used to treat sexual dysfunction in patients with PD, but they are not generally recommended for patients with cardiovascular disease.11111
Go to :
MUSCULOSKELETAL DEFORMITIES
Musculoskeletal deformities, especially posture and spinal deformities, and striatal hand and foot, are common manifestations in PD (Table 8).120121122 Health-related quality of life is significantly affected by musculoskeletal problems in PD.123 Among them, striatal hand or foot, characterized by ulnar deviation of the hand, flexion of the metacarpophalangeal joints, extension of the interphalangeal joints, and extension of the great toe, have been reported as the most common deformities, which has been estimated to occur in 10%–40% of patients with PD.120121122 Postural deformities that include antecollis, camptocormia (forward flexion of the thoracolumbar spine), Pisa syndrome (dystonia leading to lateral flexion of the spine), and scoliosis have also been described in patients with PD, and patients with an advanced stage of PD have more postural abnormalities.120121122 The pathophysiology for these musculoskeletal deformities in PD is not well-understood, but dopaminergic deficiency or dopaminergic-cholinergic imbalance might contribute to these deformities.120121122 In addition, sensorimotor dysfunction, alterations in the perception of postual alignment, and imbalances in the muscles in the trunk have been suggested as a mechanism of the dynamic postural deformities for camptocormia and Pisa syndrome.124125
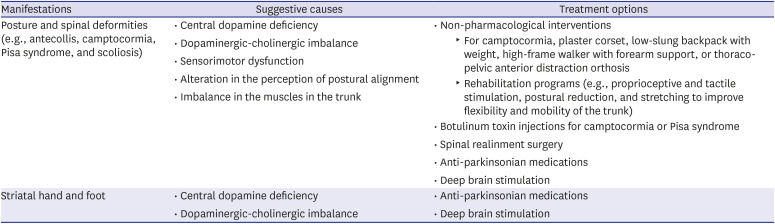
Table 8
Musculoskeletal deformities in PD
![]()
Although the evidence level is low, non-pharmacological approaches can be considered for the treatment of postural deformity (camptocormia and Pisa syndrome) (Table 8). To correct the sagittal malalignment in the camptocormia, a plaster corset, low-slung backpack with weight, high-frame walker with forearm support, or thoracopelvic anterior distraction orthosis can help.126127128129 Rehabilitation programs with proprioceptive and tactile stimulation, postural reduction, and stretching to improve flexibility and mobility of the trunk can reduce malalignment.130131 Botulinum toxin injections to hyperactive paraspinal or quadrartus lumborum muscles in patients with Pisa syndrome,132133134 and to hyperactive rectus abnominis and iliopsoas muscles in patients with camptocormia have resulted in beneficial effects.135136137 However, the efficacy of botulinum toxin injection is inconclusive due to the small sample sizes and lack of standard clinical outcome assessments. Spinal realinment surgery might be considered in severe cases of camptocormia or Pisa syndrome, but possible common postoperative complications should be considered.138 Treatment with dopaminergic medication has been attempted for patients with PD who have these deformities, but the treatment resulted in variable responses.120121122139 Neurosurgical interventions, such as deep brain stimulation, have also been attempted to treat postural deformities; the results have been limited but promising.140
Go to :
PAIN AND FATIGUE
The various forms of pain that can be categorized as musculoskeletal pain, dystonia-related pain, neuropathic pain, and central pain have been reported in approximately 40%–60% of patients with PD (Table 9).141142143 Musculoskeletal pain, a common type of pain, can result from multiple factors such as parkinsonian rigidity, stiffness, immobility, and the above-mentioned musculoskeletal deformities.141142143 Dystonia-related pain has been reported in 40% of patients with PD and may fluctuate with levodopa-related motor fluctuations, featuring as end-of-dose, diphasic, or early morning painful dystonia.141144 Radicular or neuropathic pain that is well localized to the territory of a nerve or nerve root has been attributed to a nerve or root entrapment.141142143 Patients with PD may have central pain, characterized as persistent pain or paresthesia (e.g., burning or tingling sensations) without other causative etiologies.145 This primary pain has been suggested to be related to disrupted pain perception as a result of dopaminergic deficits, based on that the nociceptive threshold is decreased in patients with PD, but levodopa treatment has been shown to increase the threshold and relieve the pain.141146 However, this finding is not consistently observed, and other neurotransmitters such as noradrenalin, serotonin, and glutamate could also contribute to pain in patients with PD.141142143 Fatigue has been reported in about one-third of patients with PD,147148149 occurring even in those with an early stage of PD.150 Dopaminergic deficiency has been suggested to play a role in the development of fatigue,151152 but serotonergic deficiency in the basal ganglia and limbic systems has been proposed as a reason for chronic fatigue syndrome in patients with PD.153154 Indeed, severity of fatigue correlated with the presence of depression and sleep disturbances rather than disease duration or severity of motor disability, suggesting the role of the serotonergic system.155156
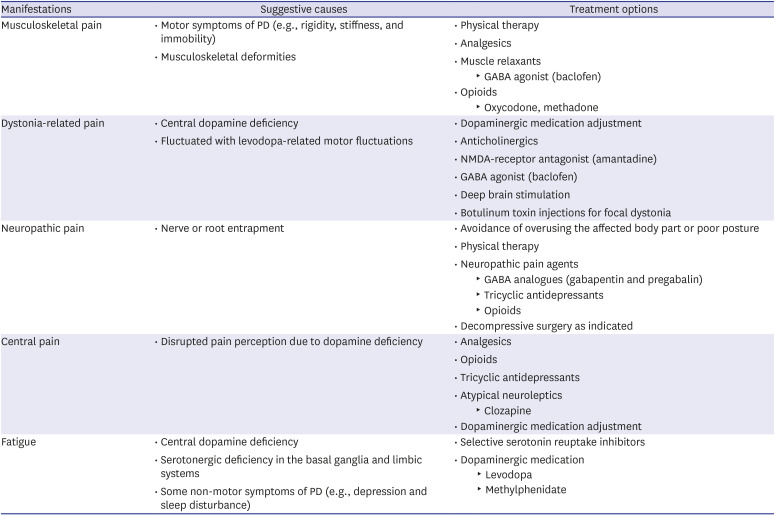
Table 9
Pain and fatigue in PD
![]()
Musculoskeletal pain can be treated with physical therapy, analgesics, muscle relaxants, or opioids (Table 9).141142143 Dystonia-related pain can be relieved by adjustment of dopaminergic drugs, administration of anticholinergics, amantadine, or muscle relaxants, deep brain stimulation, and with botulinum toxin for focal dystonia.141142143 For neuropathic pain, avoidance of overusing the affected body part or poor posture with physical therapy may alleviate the pain.141142143 Otherwise, neuropathic pain agents that include GABA analogues, tricyclic antidepressants, and opioids, or decompressive surgery as indicated may be beneficial.141142143 Central pain is often not alleviated by dopaminergic treatment, but analgesics, opiates, tricyclic antidepressants, and atypical neuroleptics (clozapine) may help.141142143 In case of pain as a non-motor fluctuating symptom during wearing-off, anti-parkinsonian medication, rather than analgesics, may alleviate the pain during the “off” period.141142 Chronic fatigue in patients with PD is commonly treated with selective serotonin reuptake inhibitors, whereas studies have indicated a beneficial effect of dopaminergic agents on fatigue, including levodopa and methylphenidate, which is a dopamine transporter blocker.157
Go to :
CONCLUSION
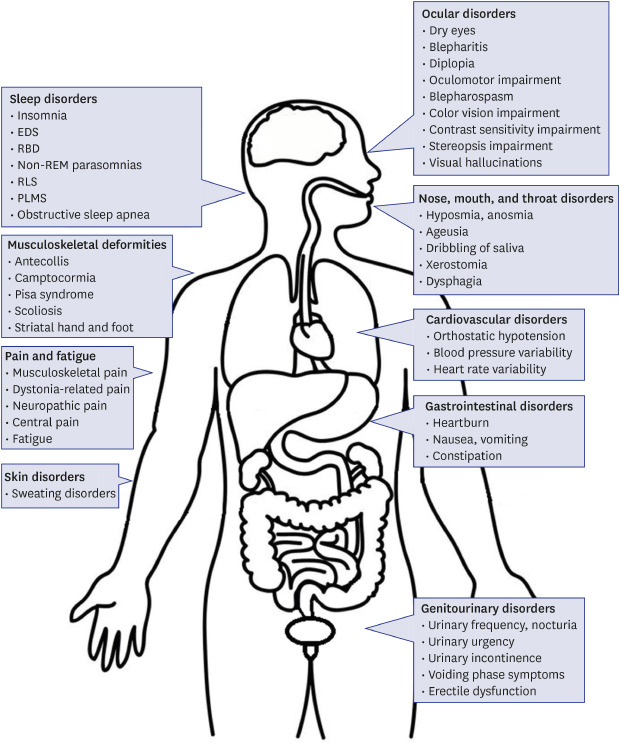
We reviewed the clinical features of NMS in patients with PD, characterized by multi-organ involvement, as summarized in Fig. 1, and briefly reviewed the pathophysiology and treatment options for NMS. Although more studies are needed to determine the exact mechanism and to manage NMS more effectively in clinical practice, our review emphasized the importance of a multidisciplinary approach for the care of patients with PD. In consideration of the fact that many NMS greatly impact the quality of life of patients with PD,158 and NMS are often unresponsive to conventional dopaminergic therapy,911 recognition and proper management of NMS by physicians cannot be overemphasized.
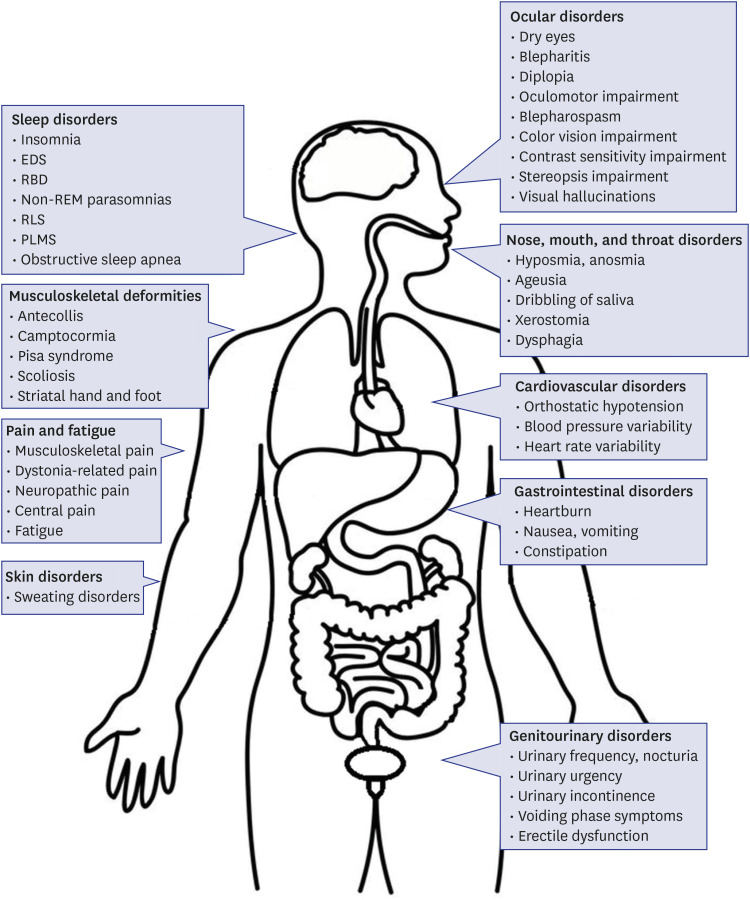 | Fig. 1Summary of multi-organ involvements in PD. In addition to motor symptoms, various NMS manifest in patients with PD. These NMS may pose a diagnostic and therapeutic challenge for physicians and surgeons in many different fields.PD = Parkinson's disease, NMS = non-motor symptoms, EDS = excessive daytime somnolence, REM = rapid eye movement, RBD = rapid eye movement sleep behavior disorder, RLS = restless legs syndrome, PLMS = periodic leg movements in sleep.
|
Go to :
 XML Download
XML Download