

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), first detected in Wuhan, China in December 2019 has rapidly led to a pandemic.12 As May 25, 2020, more than 5.3 million confirmed cases and 342,000 deaths from coronavirus disease 2019 (COVID-19) have been reported across 225 countries.3
Since the outbreak, there has been significant interest in the factors associated with the risk and severity of COVID-19. In particular, there are controversies regarding the association between hypertension or renin-angiotensin system (RAS) blockers and the risk of COVID-19 and COVID-19-related mortality. Hypertension, diabetes mellitus, and cardiovascular disease are frequent comorbidities reported in previous studies on COVID-19.456 However, it is unclear how these comorbidities are associated with risk of COVID-19 because previous findings were not fully adjusted potential confounders such as age, sex, co-morbid conditions, and medication use.
A potential plausible mechanism linking these comorbidities with COVID-19 is that SARS-CoV-2 binds to a specific enzyme called angiotensin-converting enzyme 2 (ACE2) to infect cells. ACE2 levels are increased in patients with the abovementioned comorbidities or those undergoing treatment with RAS blockers, especially certain angiotensin receptor blockers (ARBs).789 ACE2 has, therefore, been called a “double-edged sword” in the treatment of COVID-19.10 It is a receptor for intracellular entry of SARS-CoV-2; hence, increased expression of ACE2 might be associated with a higher infection risk. On the other hand, ACE2 is a counter-regulator of the RAS, which plays an adverse role through angiotensin II in the process of organ injury related to COVID-19. After SARS-CoV-2 infection, the surface expression of ACE2 is downregulated. Previous data from an animal model have shown that decreased ACE2 expression is associated with lung and/or myocardial injury.
However, the evidence regarding tissue or circulating ACE2 expression or activity after RAS blocker use in humans, especially in COVID-19 is limited. As hypertension is one of the most common chronic conditions in the general population, and as RAS blockers are commonly used for patients with hypertension or other cardiovascular diseases, this represents a significant public health issue.
There is no clinical evidence regarding whether pharmacologic regulation of ACE2 with RAS blockers may influence the infectivity of SARS-CoV-2. Observational data from a population during the COVID-19 outbreak may provide evidence on this question. Therefore, this study was conducted to assess the risk of COVID-19 in hypertensive patients with hypertension treated with antihypertensive medications in a population exposed to SARS-CoV-2.
METHODS
Study design
This retrospective cohort study included confirmed cases of COVID-19 with prescription histories of antihypertensive medication over 1-year period before the COVID-19 outbreak. We built our cohort based on population epidemiologic characteristics and medical histories extracted using big data from the Korean National Health Insurance Service (KNHIS) and linked with the COVID-19 registry data of the Korea Centers for Disease Control & Prevention (KCDC). The NHIS is a universal public health insurance system and enrollment is compulsory for nationals and registered foreigners. It offers a full coverage of health care providers including hospitals, clinics, public health centers, dental clinics, and traditional medicine clinics. Being based on a fee-for-service system, the NHIS lists all prescriptions in its claims to the Health Insurance Review and Assessment Service. Estimates of reliable risk factors for COVID-19 were based on data from Daegu Metropolitan City, the epicenter of the COVID-19 outbreak in Korea. Based on information from December 31, 2019, we estimated annual antihypertensive medication histories and COVID-19 incidences until April 2, 2020 for all adults aged over 40 or older.
In accordance with the Infectious Disease Control Act and certification procedures set out by our institutional review board, pseudonymized data were analyzed in secure and closed setting located at the Center of Big Data of the KNHIS.
Study population
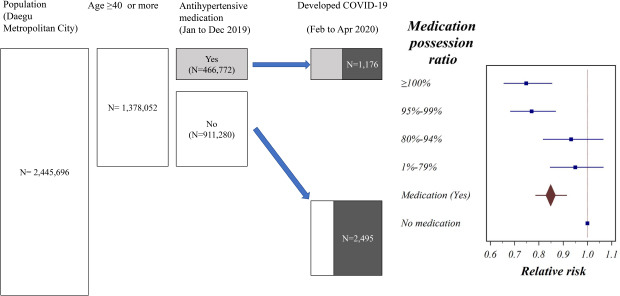
The 1,378,052 adults aged over 40 years or older living in Daegu were traced from January 1 to April 2, 2020; this sample represents 56.4% of the 2,445,696 registered residents of Daegu Metropolitan City. The first case of COVID-19 was reported in Korea on January 20, 2020 and Daegu was free from COVID-19 until the index case of a superspreading event related to a religious cult was reported on February 17. The number of confirmed cases in Daegu reached 6,725 on April 2, representing 67.4% of the 9,976 nationwide cases. A population survey was conducted on entire 9,246 enlisted members of the religious group in Daegu branch regardless of presence of symptoms, and on 15,586 citizens voluntarily reporting enlisted symptoms. An active survey was also conducted in high-risk groups (e.g., people in senior home, sanatorium, care facilities for the disabled, and long-term care facilities). Cases detected via contact tracing of confirmed cases were also included.11 These records, thus, encompass all symptomatic cases and potential contacts that occurred during the outbreak period in this area. From February 22 to March 31, the total number of tests conducted of reverse transcription polymerase chain reaction (RT-PCR) tests for COVID-19 conducted in Daegu was 119,953. The total number of patients with COVID-19 in the studied age group was 3,671 (crude incidence rate = 2.66 per 1,000). Information on sex, age, residential area, employment and income level, hospitalization history between October and December 2019 and compliance with antihypertensive medications were gathered from the KNHIS database. Compliance with antihypertensive medications was estimated using medication possession ratios (MPRs), which was calculated by dividing the total days of prescriptions by the total days of the study period. Employment status was classified into three beneficiary groups: medical benefit system, community insurance (self-employed), and workplace insurance (employee). Income level was estimated based on national health insurance (reflecting an individual's income and property) divided by the square root of the number of family members and classified into quintiles at the national level. Considering long-term prescriptions for antihypertensives, inpatient and outpatient prescription records were gathered from June 2018 to December 2019 and MPRs were estimated for the period from January 1 to December 31, 2019. For those taking combined antihypertensive medications, MPRs for each component were estimated separately.
Measurement of exposure and outcome
A total of 463,101 patients (33.7%) had been prescribed antihypertensive medication in 2019. The actual proportions of prescriptions were: 62.4% for ARBs, 58.4% for calcium channel blockers (CCBs), 34.1% for diuretics, 16.7% for beta-blockers (BBs), 2.9% for angiotensin-converting enzyme inhibitors (ACEIs), and 7.1% for others. Individual MPRs were categorized into five levels (0%, 1%–79%, 80%–94%, 95%–99%, and ≥ 100%). MPRs of ≥ 100% occurred because they were estimated based on the claims during the 1-year period. Proportions of MPR among all users were 25.6% in the 1%–79% category, 19.9% in the 80%–94% category, 30.0% in the 95%–99% category, and 24.3% in the ≥ 100% category.
According to the Guidelines of the Central Disaster Management Headquarters of the Ministry of Health and Welfare, Republic of Korea, all patients were confirmed with COVID-19 by RT-PCR testing and registered in the KCDC database.
Statistical analysis
Frequency analyses were performed to determine epidemiological characteristics and crude incidence rates (CIRs). Chi-square tests were performed to determine differences in CIRs according to demographic variables. Then, to determine effects of medication, analyses were performed and relative risks (RRs) and 95% confidence intervals (CIs) were estimated using SAS 9.4 (SAS Institute Inc., Cary, NC, USA), assuming Poisson distribution with a log (number of individuals in the study population), offset option. The statistical significance level was set at P < 0.05.
To estimate the risk of each type of medication while controlling for all potential confounders, we applied two types of analyses. At first, we considered a conventional multiple logistic regression analysis adjusting for sex, age, residential district, income level, recent hospitalization, and compliance for the total antihypertensive medication. Secondly, a difference in difference (DID) analysis comparing the effect of each antihypertensive components within the same compliance level was considered. The conceptual difference between DID and ordinary logistic regression analysis is illustrated in Supplementary Fig. 1. Unlike in conventional analyses, the relationships between total antihypertensives and each component are dependent and restrictive in DID analysis. For example, patients with a 1%–79% MPR of total antihypertensives cannot have an MPR ≥ 80% for ARBs. Further, the marginal estimates of ARBs depend on the marginal estimates of total antihypertensives and vice versa. Controlling for multicollinearity is an issue, even when many parameters with random iteration processes need to be considered, even with only two highly correlated variables. In contrast to conventional analyses, the DID analysis can control for least one variable. For example, the lower risk observed in ARBs users is estimated relative to all non-ARBs users under the control of total antihypertensive medication compliance effects on incidence.
Ethics statement
This study protocol was exempted from ethical review by the Hanyang University Institutional Review Board because the analyzed data did not contain personally identifiable information (HYU-2019-04-021). KCDC also approved using the pseudonymized case data for this study based on the Infectious Diseases Control Act.
RESULTS
Descriptive features of the study demonstrates that incidence rate is higher in females (3.42 per 1,000), in those aged over 80 or more (3.02 per 1,000), in Southern district (7.09 per 1,000), and in the recipients of Medical Benefit System (6.79 per 1,000). Moreover, individuals who were recently hospitalized just before the COVID-19 outbreak had nearly twice the incidence rate (5.56 per 1,000). Individuals who did not take antihypertensives had an incidence rate of 2.74 per 1,000. Among those individuals who were taking antihypertensives, those with poor medication compliance (MPR 1%–79%) had the highest incidence rate (2.85 per 1,000; P = 0.0026) while patients with high medication compliance (MPR ≥ 80%) had the lowest incidence rate. Patients who took ARBs and CCBs had low incidence rates (2.49 per 1,000 and 2.40 per 1,000; P = 0.0352 and P = 0.0030, respectively) (Table 1).
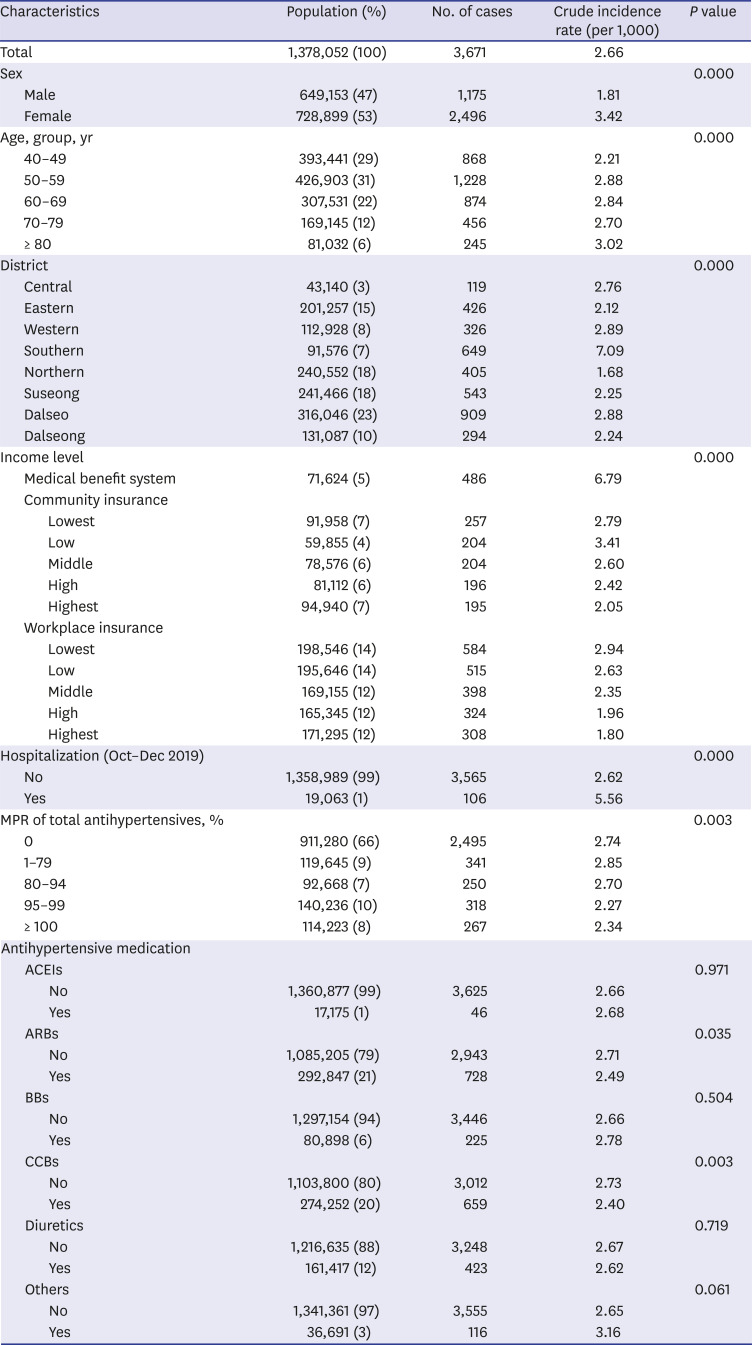
Table 1
Epidemiologic characteristics and crude incidence rates of coronavirus disease 2019 in the study population
MPR = medication possession ratio, ARBs = angiotensin receptor blockers, ACEIs = angiotensin-converting enzyme inhibitors, BBs = beta blockers, CCBs = calcium channel blockers.
![]()
The multiple regression analysis showed a lower risk for males (RR, 0.548; 95% CI, 0.511–0.588) than for females. Adults aged 50–54 years had the highest RR (1.552; 95% CI, 1.358–1.773) compared to those aged 40–44 years, but there was no age-related trend. However, lower-income earners, including their family members, had consistently higher incidence rates in the community and workplace insurance category. The incidence rate of medical benefit system recipients was 3.246 (95% CI, 2.809–3.752) times higher than that of the highest-income level group. There was spatial variability in incidence rates for districts, with a 2.4-fold difference between district with the highest and lowest incidence rates. The RR of patients who were hospitalized between October 1 and December 31, 2019 was 1.804 (95% CI, 1.484–2.193) times higher than that of other patients. Higher MPRs of antihypertensives were consistently correlated with lower incidences. Compared to individuals who were not prescribed antihypertensives, patients with 1%–79%, 80%–94%, 95%–99%, and ≥ 100% MPRs had 0.950 (95% CI, 0.846–1.067), 0.933 (95% CI, 0.817–1.066), 0.770 (95% CI, 0.682–0.870), and 0.748 (95% CI, 0.655–0.855) times lower incidence rates, respectively (Table 2).
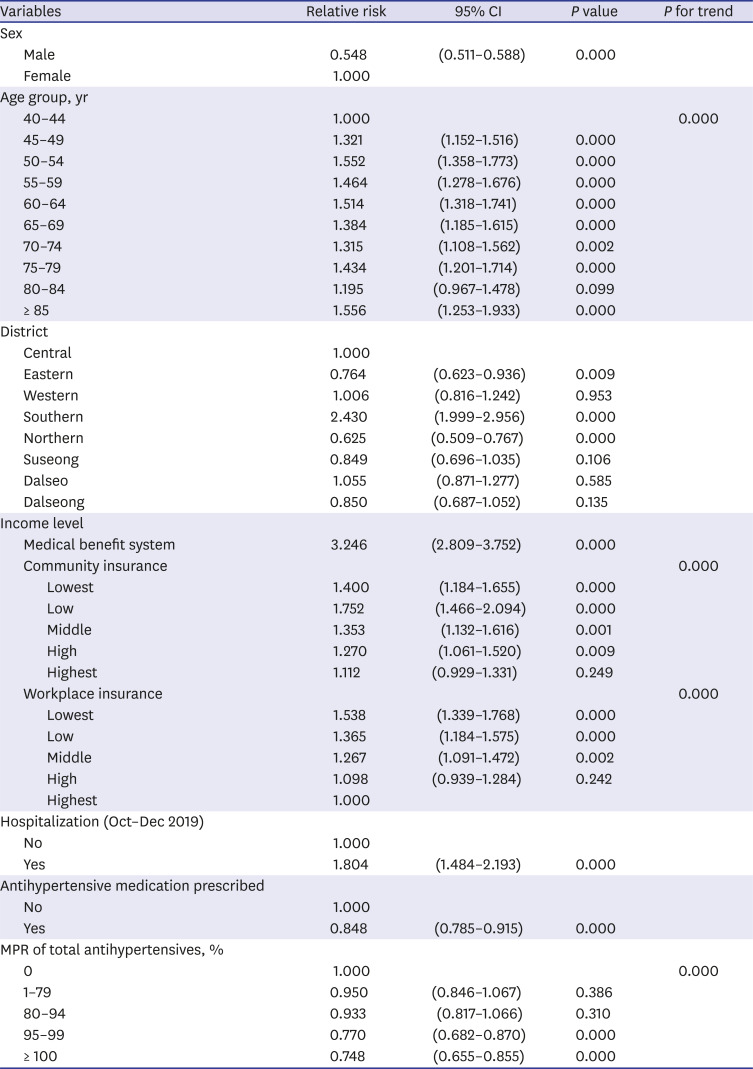
Table 2
Risk of coronavirus disease 2019 according to the risk factors, multiple regression model 1
![]()
The DID analysis showed that patients with perfect compliance had a significantly lower risk among those taking ARBs (RR, 0.751; 95% CI, 0.587–0.960) or CCBs (RR, 0.768; 95% CI, 0.601–0.980) (Fig. 1). There were some other significant findings for other antihypertensives, but these were regarded as noise (Supplementary Table 1).
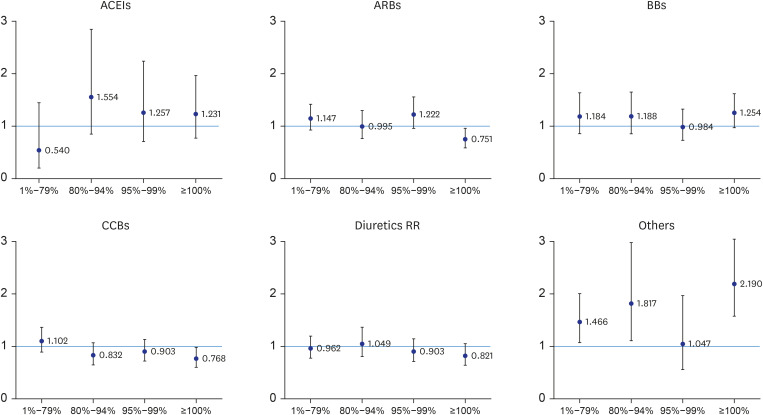
Fig. 1
Risk of coronavirus disease 2019 according to the type of antihypertensives in Daegu, Korea, difference in difference analysis. Adjusted for sex, age group, residential districts, income level, recent hospitalization, and medication possession ratio of total antihypertensives.
ACEIs = angiotensin-converting enzyme inhibitors, ARBs = angiotensin receptor blockers, BBs = beta blockers, CCBs = calcium channel blockers, RR = relative risk.
![]()
DISCUSSION
We demonstrate that antihypertensive medications including ACEIs and ARBs are not associated with an increased risk of COVID-19. In fact, the risk of COVID-19 was lower among patients who were compliant to hypertensive medications in our sample. Although there is a controversy regarding effects of RAS blockers on the risk of COVID-19, our findings indicate that there is no direct association between the two.
Early studies from China, Korea, and Italy on epidemiological characteristics of COVID-19 have reported a higher risk and a worse prognosis for people with underlying diseases such as hypertension, cardiovascular disease, and diabetes, which are all related to the potential use of RAS blockers.121314 The mechanism linking COVID-19 and RAS blockers is unclear; however, there is evidence that RAS blockers can increase ACE2 expression and that SARS-CoV-2 binds to ACE2 as a co-receptor on entry into host cells, which is expected to be harmful in lung tissue.9 Since SARS-CoV-2 is known to enter cells through ACE2, interest in the effects of medications involved in RAS and how they affect viral infections is high. Two hypotheses have been proposed that correlate SARS-CoV-2 with RAS blockers. The first is that when medications such as ACEI and ARB inhibit RAS, ACE2 on the surface of the cell is upregulated, and the entry of the virus into cells is further enhanced, thus promoting lung damage.81516 The second hypothesis is that regardless of the combination of SARS-CoV-2 and ACE2, ACEI and ARB promote the production of angiotensin-(1-7) by ACE2 to protect lung tissue.91718
In our conventional logistic regression analysis (Model 1), patients with MPRs >95% showed a lower risk trend that was, however, not statistically significant. In the DID analysis (Model 2), patients who showed perfect compliance had significantly lower incidences of COVID-19 among those taking ARBs and CCBs. These results corroborate that use of RAS blockers or other antihypertensive medications are not related to an increased risk of COVID-19. The risk of COVID-19 was lower in patients with good adherence to antihypertensive medications. Further, patients with good compliance to CCBs showed a lower risk of COVID-19. A preliminary report suggests that CCBs are associated with reduced case fatality rates in COVID-19 patients with hypertension.19 However, the association was observed for RAS blockers as well, and these findings may not be related to the mechanisms of specific antihypertensive agents. The relationship between good compliance with antihypertensive medication and a low risk of COVID-19 could be explained by unmeasured confounders related to good adherence to hypertension treatment. Previously, clustering of unhealthy lifestyle behaviors was more commonly observed in patients with low adherence to recommended preventive activities.20 Therefore, poor adherence to antihypertensive medication might be related to unhealthy behaviors such as smoking, physical inactivity, and poor hand hygiene.
The RAS plays a multifaceted role, but the association between SARS-CoV-2 infection and RAS blockers is unclear. Patients with cardiovascular disease and those with diabetes, complications are also treated with ACEIs and ARBs. This implies that our scope of understanding should be expanded to include biological mechanisms to investigate whether the increase in ACE2 expression due to the use of ACEIs and the up-regulation of ACE2 due to the use of ARBs increases the viral load entering the cell and whether this affects disease progression and severity. More research is needed to address these questions.
This study had several limitations. First, we measured medication adherence indirectly based on the KNHIS claims data. Therefore, the data may not reflect real compliance with antihypertensive medication in the population. However, KNHIS claims are based on the full coverage of prescriptions and pharmacy purchases, this is a practical indirect method to assess medication adherence in a large population. Furthermore, our definition of hypertension was based on prescriptions, which may have excluded hypertensive patients who do not take antihypertensive medications or did not visit a clinic during the study period. Second, our risk estimation based on MPRs may not reflect actual compliance at the time of the outbreak. Therefore, our interpretation of therapeutic effects of antihypertensive medications in the management of patients with COVID-19 should not be overrated. Irrespective of the disease severity, all confirmed cases were managed by admission to health care facilities or repurposed institutions. We did not have information on either the patients' clinical course during the hospital day or their outcomes. Therefore, the risk of developing severe and fatal COVID-19 is not reflected in our analysis.22 Third, risk of medication was estimated on the basis of pharmacologic mechanisms and not on the basis of individual antihypertensive medication. Likewise, we did not estimate the risk of other medications related to RAS blocking, including thiazolidinediones13 and ibuprofen. Lastly, cases were mostly symptomatic patients, diagnosed using RT-PCR testing. Despite the comprehensive coverage of symptomatic cases in the general population during the outbreak period, most asymptomatic patients may not have been detected.23 The prevalence of asymptomatic infection of COVID-19 varies depending on the characteristics of contact and population. A recent estimate was reported to be 40% to 45%.24 In Daegu, criteria of COVID-19 testing were extended, including all identified cult members, which may have included a higher proportion of asymptomatic cases than the outbreak in the other areas. A report from one series of screening center, 75 (34.6%) out of 217 with a positive test for COVID-19 was asymptomatic, which was slightly lower, but reasonable, than the previous report, considering the criteria of RT-PCR testing in Daegu, i.e., testing for all identified cult group regardless of symptom, but only those with any symptoms among general citizen.2425 This may reflect the over-representation of the cult group.
This study presents an observational report on the risk of COVID-19 according to components of antihypertensive medication. Based on a population survey with a comprehensive coverage of the general population and confirmed cases via extensive RT-PCR testing, this study is less prone to selection bias of the population and detection bias of the cases. Information on potential confounders was also comprehensive based on the objective assessments of employment status and income level, residency, and biologic features of the study population. Cases were defined based on a national survey, therefore, cases detected outside the Daegu area were not excluded, even if the city was not closed during the outbreak. This outbreak was one of the biggest outside China at the earlier phase of global pandemic, development of herd immunity may not have affected the outbreak process. As medication history data was based on comprehensive recordings of prescriptions with national coverage, exposure assessment were relatively unbiased. Therefore, our analysis was conducted with a minimum adjustment for essential confounders.
In conclusion, antihypertensive medication use by hypertensive patients did not increase the risk of SARS-CoV-2 infection during the recent community outbreak in Korea. Some protective effects of ARBs and CCBs were observed, but these may not necessarily represent pharmacologic protection. The study findings suggest that maintenance of a high compliance to antihypertensive medication may be beneficial in hypertensive patients.
 XML Download
XML Download