

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
N,N-dimethylformamide (DMF) is a colorless organic solvent with the formula (CH3)2NC(O)H and chemical abstracts service number 68-12-2. It is extensively used in the manufacturing of synthetic leathers, films, fibers, surface coatings, and polyurethane materials. Its global consumption is significantly increasing according to the rapid growth of the chemical, pharmaceutical and electronic industries.123
Its toxic effects include hepatotoxicity, carcinogenesis, embryotoxicity, heart and renal toxicity, which were shown in animal studies and human cases.4567 Despite governmental regulation on the occupational exposure limit for DMF and industrial hygiene surveillance, new cases of DMF poisoning are frequently reported, especially in China.1 Human exposure to DMF is mainly through skin contact and inhalation in occupational settings. While many cases of DMF-induced toxic hepatitis were reported, there have been no known cases of DMF-induced autoimmune hepatitis (AIH).
AIH is a rare, immune-mediated hepatitis characterized by the presence of autoantibodies, an elevated blood immunoglobulin G (IgG) level and typical pathological features including interface hepatitis with portal lymphoplasmacytic infiltrates.8 AIH can present as a wide spectrum of liver diseases including acute hepatitis or acute liver failure, chronic hepatitis, liver cirrhosis and hepatocellular carcinoma (HCC).9 Here, we report the first case of AIH after occupational exposure to DMF so that clinicians are aware of DMF-related AIH for a timely therapeutic decision.
Go to : 
CASE DESCRIPTION
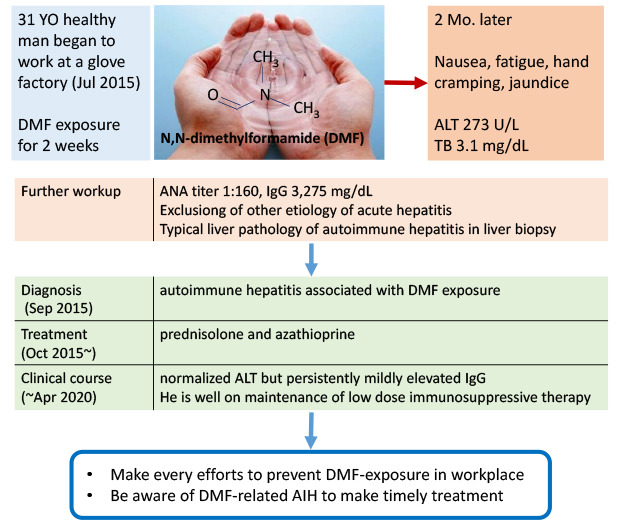
A 31-year-old man, who was previously healthy and a regular blood donor until Mar 2015, started working at a glove factory in July 2015. At his workplace, he had intermittently put his bare hands in a diluted solution of DMF without wearing gloves for the first 15 days at work despite receiving occupational safety education. He did not consume any drugs or excessive alcohol.
In late Aug 2015, he felt nausea, fatigue, and intermittent hand cramping, which led to another hospital admission with suspicion of non-viral acute hepatitis. His laboratory findings were suggestive of the diagnostic criteria of AIH: serum total bilirubin, 3.1 mg/dL; aspartate aminotransferase (AST), 292 IU/L; alanine aminotransferase (ALT), 273 IU/L; alkaline phosphatase, 72 IU/L; gamma glutamyl transferase, 89 IU/L; positive antinuclear antibodies (ANA) with a titer of 1:160, and a high level of IgG at 3,275 mg/dL. He underwent a liver biopsy on September 9, and the pathology report showed chronic hepatitis, probably toxic, and the liver copper content was sufficiently normal (28 ug/g) to exclude Wilson's disease. His physician diagnosed him as type 1 AIH and treated him with daily prednisolone 30 mg plus azathioprine 50 mg from October 30; however, his jaundice was aggravated; thus, he visited our hospital on November 4, 2015 (Fig. 1).
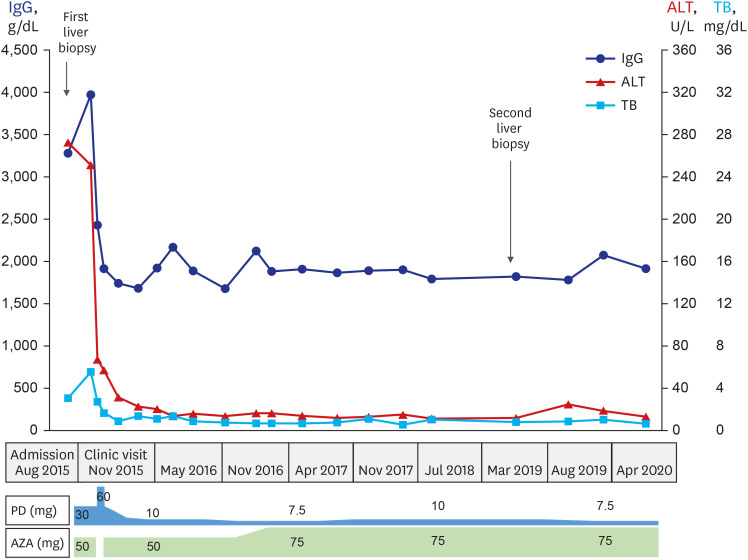 | Fig. 1Clinical course of the case. Initial laboratory results showed elevated ALT and IgG levels with typical pathology of AIH by liver biopsy. He responded well to prednisolone and azathioprine.ALT = alanine aminotransferase, IgG = immunoglobulin G, AIH = autoimmune hepatitis, PD = prednisolone, AZA = azathioprine, TB = total bilirubin.
|
At our hospital, his laboratory results were as follows: bilirubin, 5.6 mg/dL; ALT, 252 IU/L; IgG, 3,970 mg/dL; ANA, 1:320 (+); anti-smooth muscle Ab (+), anti-LKM1 (−), and anti-mitochondrial Ab (−). Review of his previous liver pathology showed portoperiportal lymphoplasmacytic infiltration and interface activity with confluent centrilobular necrosis, which was compatible with severe AIH with acute presentation (Fig. 2A-C). To avoid azathioprine hepatotoxicity, prednisolone single therapy (60 mg/day) was tried, and his liver chemistry improved rapidly. From November 25, the combination therapy of prednisolone 30 mg and azathioprine 50 mg was tried which led to normalization of the ALT and IgG in March 2016.
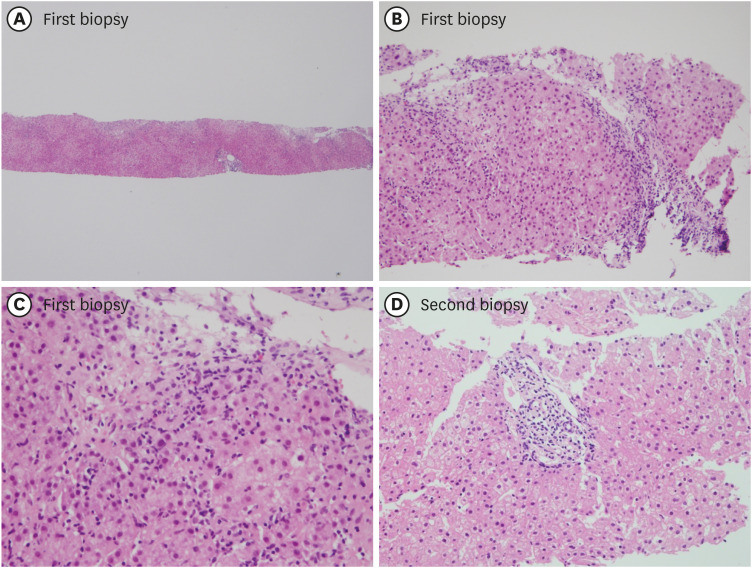 | Fig. 2Microscopic findings of the first and second liver biopsy specimens (hematoxylin and eosin staining). First biopsy-(A) inflammation concentrated at portal tract (×40); (B) lymphoplasmacytic infiltration in hepatic lobule (×200); (C) interface activity (×400). Second biopsy-(D) mild nonspecific portal inflammation (×200).
|
However, tapering off of the daily prednisolone to 7.5 mg resulted in an elevated IgG level; thus, a combination therapy of prednisolone 10 mg and azathioprine 75 mg was maintained until March 2019. To make a decision on whether to taper the immunosuppressive therapy further, he underwent a 2nd liver biopsy on April 2019, which showed mild nonspecific portal inflammation, minimal interface activity and no lobular activity (Fig. 2D). After the liver biopsy, a gradual tapering of the immunosuppressive therapy was planned. He was in good condition without symptoms and maintained normal liver tests with prednisolone 5 mg combined with azathioprine 75 mg until April 2020.
Ethics statement
We obtained an informed consent from the patient for this case report after approval of Institutional Review Board (IRB) of Seoul National University Bundang Hospital (IRB No. B1912-583-701).
Go to :
DISCUSSION
Here, we report a case of acutely presenting severe type 1 AIH probably induced by occupational exposure to DMF and successfully treated it with immunosuppressive therapy in a previously healthy 31-year-old Korean man. This is the first reported AIH case related to DMF to our knowledge.
The precise pathogenesis of AIH is not known; however, recent studies have revealed that environmental factors may trigger AIH in genetically susceptible individuals such as having human leukocyte antigens (HLA) DR3 and DR4. The exposure of self-mimicking exogenous factors trigger an immune response to structurally similar self-proteins (molecular mimicry), and T cells targeting the self-epitope become primed and expand, which leads to initiation and perpetuation of autoimmune- mediated liver injury.10
Molecular mimicry is well demonstrated in type 2 AIH, in which the key target antigen of autoimmune responses is the liver enzyme cytochrome P450 (CYP) 2D6 (CYP2D6), and an amino acid sequence of CYP2D6 has a high level of homology with proteins encoded by hepatitis C virus and members of the herpes virus family (for example, cytomegalovirus, Epstein–Barr virus and herpes simplex virus). There are many cases of AIH after viral infection of the above noted viruses as well as hepatitis A, B and E virus, and an experimental mouse model also supported molecular mimicry as a pathogenic mechanism of AIH. Not only viral infection, but also environmental toxins could change the hepatic epitope, which could trigger an autoimmune response by molecular mimicry, including nitrofurantoin, minocycline, statins, diclofenac and several herbal medicines.1011
DMF is metabolized by CYP2E1 in the liver, and its metabolites are excreted through the urine.1213 In the hepatic metabolism process, DMF is hydroxylated to N-hydroxymethyl-N-methylformamide by CYP2E1, then decomposes to N-methylformamide (NMF). The NMF may further decompose to formamide or form a reactive metabolic intermediate by CYP2E1, which could spontaneously react with glutathione or adduct with hemoglobin. DMF could induce a dose-dependent increase in reactive oxygen species production, and treatment with antioxidants such as N-acetyl cysteine led to a reduction of the serum marker for DMF-induced hepatotoxicity in rats.
Therefore, it is highly likely that the hepatic metabolism of DMF and consequent changes in redox homeostasis account for the DMF-induced hepatic toxicity. Moreover, DMF led to hepatocyte necrosis or apoptosis, and alteration of the gut microbiota in experimental animals and in vitro studies.1 Moreover, the reactive metabolites may be recognized by the immune system as neoantigens by binding to cellular proteins such as CYP or others, which further leads to the development of AIH. It is difficult to prove this case was DMF-induced AIH, because there are no previously reported cases, and no available experimental data on the pathogenic mechanism of DMF in the development AIH. However, our case was previously healthy man supported by repeated blood donation with documented normal liver test results. He evidently exposed to DMF through hands' skin, and time sequence of development of AIH after DMF exposure with exclusion of other cause of hepatitis strongly suggest that this case was related to DMF.
Though AIH is categorized as a rare liver disease, complete remission with immunosuppressive therapy is achieved in more than 80% of patients. Therefore, a high index of suspicion for an early diagnosis of AIH and timely treatment are important to intervene in the disease progression to acute liver failure or liver cirrhosis with complications such as end stage liver disease or HCC.141516 There are many human mortality cases of DMF induced hepatotoxicity ranging from acute liver failure to decompensated liver cirrhosis, though most of the DMF-induced liver damage is recovered.17181920
The limitation of this study includes no measurement of DMF exposure at his workplace, and no detection of the urine metabolite for DMF at the early phase of diagnosis, and his HLA typing was not performed due to cost issues.
In conclusion, we report this case because there are no reported cases of AIH associated with DMF to our knowledge, and it is important that clinicians are aware of DMF-associated AIH to make timely therapeutic decisions. Moreover, workers who handle DMF should receive strict workplace safety education and undergo periodic medical examinations to prevent the occurrence of DMF poisoning.
Go to :
 XML Download
XML Download