

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Beginning December 2019 the world has been experiencing an outbreak of novel coronavirus (CoV) infection, called coronavirus disease 2019 (COVID-19). This is the third member of a family of CoVs that is associated with the development of severe acute respiratory syndrome (SARS) due to atypical pneumonia. The disease has evolved from Wuhan, China and was first reported among the visitors of local seafood market. It is likely to have a zoonotic origin as horseshoe bats are a well-known natural reservoir for a variety of CoVs that spread to humans via incidental hosts, which has not yet been identified in relation to COVID-19.1
The novel CoV was determined already on 9 January 2020 and received a name of SARS-CoV-2.2 The virus quickly spread over the globe, on 30 January 2020 the World Health Organization (WHO) declared COVID-19 a public health emergency of international concern, and already on 11 March 2020 a pandemic was announced.3 Currently, more than 5.8 million cases of COVID-19 were reported with more than 350 thousand associated deaths.4 The confirmed case is defined as a positive test for COVID-19 regardless the presence of symptoms and signs of the disease.5 Thus, identification of cases depends on testing coverage, while many countries do not test individuals with only mild symptoms.6
According to the recent meta-analysis, the most common symptoms of COVID-19 are fever (82%), cough (61%), fatigue with or without muscle aches (36%), dyspnea (26%), headache (12%), sore throat (10%), and gastrointestinal symptoms (9%).7 In China, the vast majority of COVID-19 cases are mild (81.4%), whereas 13.9% are severe and 4.7% are critical.8 In countries of European Union the proportion of severely ill patients is approximately the same and constitutes 15% of hospitalized cases.9 The increased case fatality rate (CFR) was established in older patients (≥ 60 years), males, and those who presented with severe pneumonia and comorbidities.10
As an outbreak expands in the country, more and more individuals become affected and a number of critically ill patients may increase drastically, surpassing the abilities of health care system to resist the coercive pressure. Therefore, several approaches were proposed to decrease the rate of disease spreading and to secure the capacity of health care in meeting the population demands.11 Such approaches could be divided into two broad categories–individual protection and community protection. Voluntary self-isolation, frequent hand washing, following the principles of respiratory etiquette, wearing of face masks in public places and avoidance of touching face work well on a personal level, while mass quarantine of healthy individuals, closures of schools and child care facilities, social distancing, and regular cleaning of frequently touched surfaces in public places enable community protection.12
Most countries across the globe implemented a set of protective measures with mass quarantine, social distancing, and travel restrictions being the most frequently practiced. Although it definitely had positive response, the COVID-19 pandemic is still far from its final phase and some international researchers anticipate another wave later this year.13 In this study, we aim to report on the rates of COVID-19 in the Republic of Kazakhstan, to make prognoses on cases, deaths, and recoveries through predictive modeling, and to forecast the need in professional workforce.
METHODS
Data sources
Positive polymerase chain reaction (PCR) test for SARS-CoV-2 is currently used in the Republic of Kazakhstan to confirm the COVID-19 case. Ministry of Health reports on the number of COVID-19 cases via a special platform run by the National Center of Public Health.14 The data on total population at risk (average in year) were obtained from official statistics presented at the website of Republican Center for Health Development.15 From these data, we constructed a real-time database that included all COVID-19 cases in the country beginning March 13, 2020 and ending May 28, 2020.
Study setting
Kazakhstan has a population of 18,654,000 people16 and is administratively divided into 14 regions (East Kazakhstan, Pavlodar, Akmola, Karaganda, Kostanay, North Kazakhstan, Aktobe, Atyrau, Mangystau, West Kazakhstan, Almaty, Zhambyl, Kyzylorda, and Turkistan regions). Also, three cities–Nur-Sultan, Shymkent and Almaty–do not belong to the regions they are surrounded by and are considered as the separate administrative units.17
Formulas used
The CFR was calculated as the proportion of individuals who die from COVID-19 out of all individuals who were diagnosed with the disease over the period from March 13, 2020 till May 28, 2020:
The mortality rate (MR) for COVID-19 was calculated on the basis of theoretical assumptions as the current situation is changing and we will have more precise data on COVID-19 cases and mid-year population by the end of 2020. The following formula was applied:
MR = (total number of COVID-19 deaths at current point of time / estimated mid-year population in 2020) × 1,000.
The incidence rate (IR) was calculated as:
The CFR (age-adjusted) was calculated on the basis of overall number of fatal cases of COVID-19 in specific age group and overall number of COVID-19 cases in the same group:
The CFR (age-and-sex-adjusted) was calculated based on total number of fatal outcomes in specific age and sex group and total number of COVID-19 cases in the same group via the following formula:
CFR (age-and-sex-adjusted) = fatal outcomes in specific age and sex group / total cases in specific age and sex group.
The growth forecasts for COVID-19 were calculated with possibility of exponential growth, i.e., on the basis of assumption that current growth trends are true and that future growth of COVID-19 cases will be proportional to numerical values of COVID-19 with 95% confidence interval (CI).
Forecast modeling
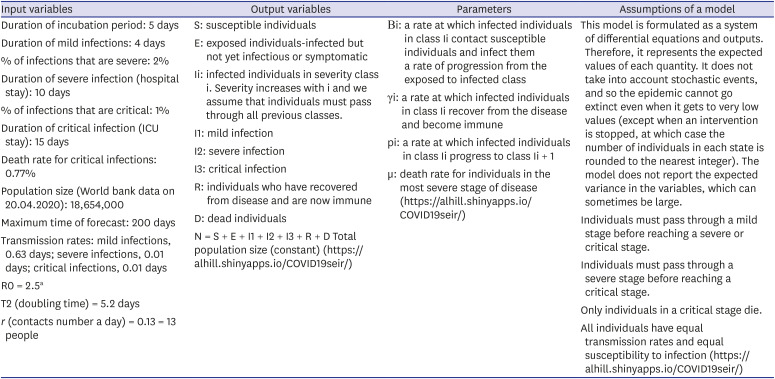
To describe the spread and progression of COVID-19 in the Republic of Kazakhstan, we applied an on-line tool18 of compartmental epidemiological model, which is based on the classic susceptible-exposed-infected-removed (SEIR) model. SEIR model is a widely used method for modeling of epidemic situation in the specific place. The model is based on the SIR model with addition of “exposed” compartment. According to this model, all people are categorized as susceptible (individuals who can develop the disease), exposed (individuals who are already infected but have no symptoms), infected (infected individuals who show symptoms and signs), and removed (recovered individuals).19 The time of modeling used was equal to 200 days. The list of basic variables that were used in the model without intervention is presented in Table 1.
Table 1
Basic variables and characteristics of SEIR model for COVID-19 in Kazakhstan
| Input variables | Output variables | Parameters | Assumptions of a model |
|---|---|---|---|
| Duration of incubation period: 5 days | S: susceptible individuals | Βi: a rate at which infected individuals in class Ii contact susceptible individuals and infect them | This model is formulated as a system of differential equations and outputs. Therefore, it represents the expected values of each quantity. It does not take into account stochastic events, and so the epidemic cannot go extinct even when it gets to very low values (except when an intervention is stopped, at which case the number of individuals in each state is rounded to the nearest integer). The model does not report the expected variance in the variables, which can sometimes be large. |
| Duration of mild infections: 4 days | E: exposed individuals-infected but not yet infectious or symptomatic | a rate of progression from the exposed to infected class | Individuals must pass through a mild stage before reaching a severe or critical stage. |
| % of infections that are severe: 2% | Ii: infected individuals in severity class i. Severity increases with i and we assume that individuals must pass through all previous classes. | γi: a rate at which infected individuals in class Ii recover from the disease and become immune | Individuals must pass through a severe stage before reaching a critical stage. |
| Duration of severe infection (hospital stay): 10 days | I1: mild infection | pi: a rate at which infected individuals in class Ii progress to class Ii + 1 | Only individuals in a critical stage die. |
| % of infections that are critical: 1% | I2: severe infection | μ: death rate for individuals in the most severe stage of disease (https://alhill.shinyapps.io/COVID19seir/) | All individuals have equal transmission rates and equal susceptibility to infection (https://alhill.shinyapps.io/COVID19seir/) |
| Duration of critical infection (ICU stay): 15 days | I3: critical infection | ||
| Death rate for critical infections: 0.77% | R: individuals who have recovered from disease and are now immune | ||
| Population size (World bank data on 20.04.2020): 18,654,000 | D: dead individuals | ||
| Maximum time of forecast: 200 days | N = S + E + I1 + I2 + I3 + R + D Total population size (constant) (https://alhill.shinyapps.io/COVID19seir/) | ||
| Transmission rates: mild infections, 0.63 days; severe infections, 0.01 days; critical infections, 0.01 days | |||
| R0 = 2.5a | |||
| T2 (doubling time) = 5.2 days | |||
| r (contacts number a day) = 0.13 = 13 people |
SEIR = susceptible-exposed-infected-removed, COVID-19 = coronavirus disease 2019, ICU = intensive care unit.
aR0 is a reproduction number and the value of 2.5 was selected because it was the most common in other models https://www.isglobal.org/en/coronavirus-lecciones-y-recomendaciones.
After modeling the situation without intervention measures, we assumed that measures implemented by the country government will be effective at least in 50% cases. So, possible reduction of R0 on 50% was taken as an influence factor of quarantine introduction. The quarantine measures were induced in Kazakhstan on the 6th day (19 March 2020) after the first COVID-19 case appeared (13 March 2020). Thus, start time for the intervention was inputted as the tenth day because it is the earliest possible day in SEIR modeling. Basic parameters of model after intervention and reduction of R0 were: R0 = 1.25; r = 0.025 per day, and T2 = 27 days. We created the forecast graphs that reflected reduction of all symptomatic patients, all infected and exposed individuals, all deaths and all hospitalized cases.
The Health Workforce Estimator tool (version 2.2; WHO, Copenhagen, Denmark) was utilized for forecast modeling of health care workers capacity.20 This tool provides a daily estimate of each type of health care personnel needed to treat all country cases of COVID-19 depending on their severity (mild, moderate, severe, and critical). Being developed by the WHO, the tool estimates ideal workforce numbers. To make calculations, we grounded our judgments on the basis of SEIR modeling outcomes. Thus, for the scenario when no intervention measures are applied, we made the following inputs: out of total number of symptomatic individuals (2.038 million) there will be 80% mild cases (1.63 million), 18% moderate cases (367.2 thousand), about 2% severe cases (40.8 thousand), and 0.77% critical cases. The same assumptions were applied for forecasting the need in health care professionals in case of implementation of quarantine measures with an account of reduction in symptomatic individuals to 84.92 thousand cases at the peak.
Definitions of clinical stages used in SEIR modeling
Mild infection is defined as symptomatic individuals who have mild disease manifestations, i.e., fever and cough and mild pneumonia. Commonly, hospitalization is not required (though in many countries such individuals are also hospitalized). Severe infection is defined as symptomatic individuals presenting with severe disease manifestations, i.e., more severe pneumonia that leads to dyspnea, respiratory rate < 30/min, blood oxygen saturation < 93%, ratio of partial pressure arterial oxygen to fraction of inspired oxygen (PaO2/FiO2 < 300), and/or lung infiltrates > 50% volume within 24 to 48 hours. Hospitalization and supplemental oxygen therapy are generally required. Critical infection is defined as symptomatic individuals who experience respiratory failure, septic shock, and/or multiple organ dysfunction or failure. The treatment is provided in an intensive care unit (ICU) and often requires mechanical ventilation.18
We assume that all infected individuals will show the signs of mild disease in 80% cases, moderate disease in 18% and will have severe disease in about 2% cases (that may potentially become critical in the future). This assumption is based on the current distribution of COVID-19 clinical forms in Kazakhstan.
RESULTS
Overall, the crude incidence rate of COVID-19 in the country is 0.5240 with much heterogeneity between administrative units. Such, the highest incidence rate was observed in two largest cities – Nur-sultan and Almaty. It has to be noted that first patients in the country were identified in these cities and there is a high concentration of specialized medical facilities, which serve as referral centers for severely ill patients from neighboring regions. The lowest incidence rate was seen in East Kazakhstan and North Kazakhstan regions, where it constituted 0.0536 and 0.0916, respectively. The highest crude CFR was spotted in Akmola region (2.68) followed by Kostanay region (1.47) and East Kazakhstan region (1.35) (Table 2). As for the age-adjusted CFR, it was the highest in age stratum 90-99 (0.083). Eighty-eighty nine-year old males had excessive age-and-sex-adjusted CFR (0.167) and so did 90–99 year old females (0.111) (Table 3). From the beginning of COVID-19 outbreak in Kazakhstan, the vast majority of patients (87.4%) had mild disease, 11.3% had moderate disease, while severe manifestations were seen in 1.3% cases (Fig. 1).
Table 2
Crude epidemiology indicators of COVID-19 (28.05.2020)
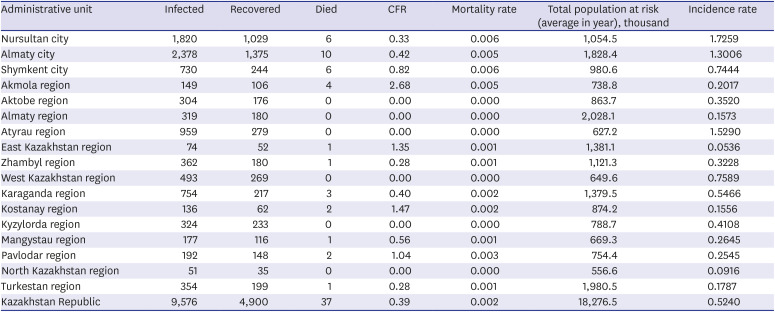
Table 3
Case fatality rate (sex and age adjusted) (May 28, 2020)
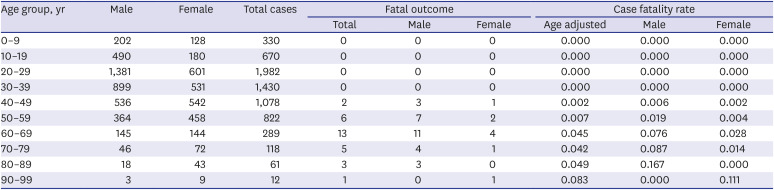
Fig. 1
General epidemiology of COVID-19 in the Republic of Kazakhstan: 13 March 2020–28 May 2020.
COVID-19 = coronavirus disease 2019.

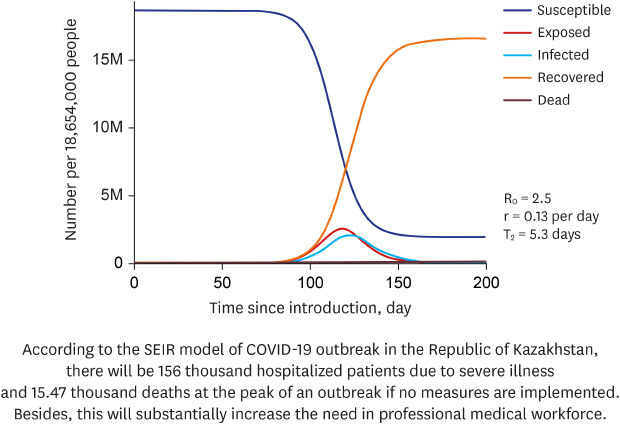
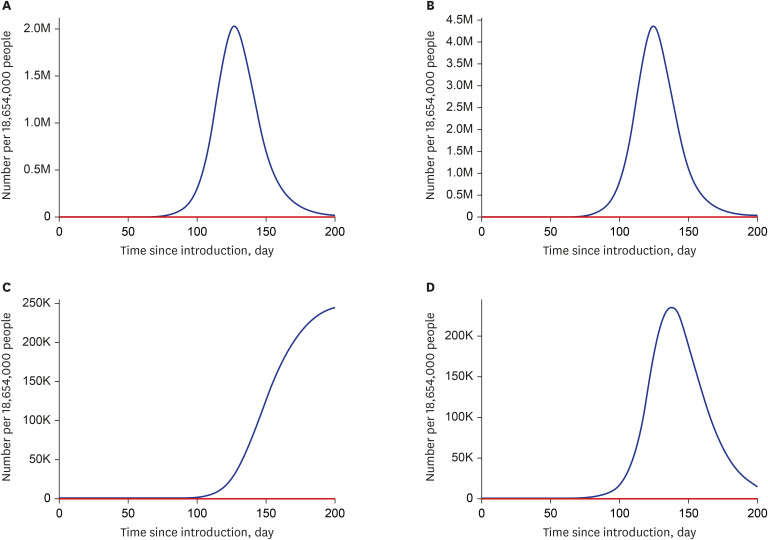
Fig. 2 presents the results of SEIR modeling in situation when no intervention measures are applied. Such, a possible peak is 120 day after appearance of the first COVID-19 case in the country and the number of susceptible population is 7.12 million people. At the peak of COVID-19 outbreak there will be 2.038 million infected individuals, 2.5 million exposed individuals, 15.47 thousand people will die, and 156 thousand patients will require hospitalization. Fig. 3 demonstrates the changes in COVID-19 dynamics introduced by the quarantine measures. Reduction of all symptomatic patients (with mild [I1], severe [I2] and critical [I3] disease manifestation) will result in total 84.92 thousand cases at the peak (Fig. 3A). Reduction of all exposed and infected individuals will give in total 188.983 thousand cases at the peak (Fig. 3B). Reduction of all deaths will result in total 3.75 thousand cases at the peak (Fig. 3C) and reduction of all hospitalized patients (with severe and critical disease manifestation) will give in total 9.31 thousand cases at the peak (Fig. 3D).
Fig. 2
SEIR modeling of COVID-19 outbreak in Kazakhstan without intervention measures (https://alhill.shinyapps.io/COVID19seir/).
SEIR = susceptible-exposed-infected-removed, COVID-19 = coronavirus disease 2019.
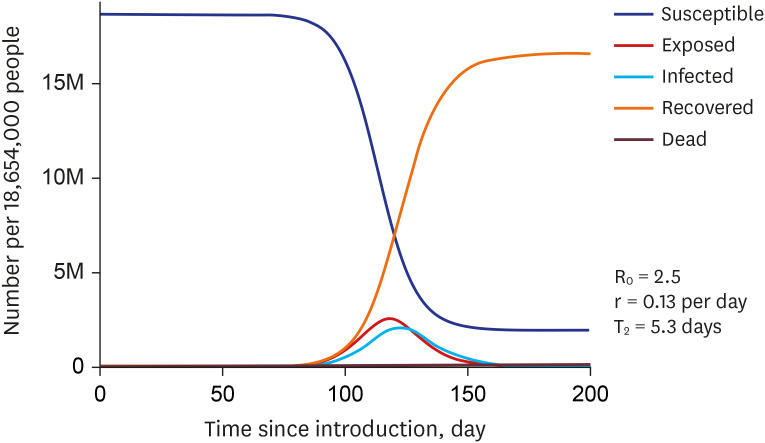
Fig. 3
Reduction of all symptomatic individuals (A), Reduction of all infected and exposed individuals (B), Reduction of all deaths (C), and Reduction of all hospitalized patients (D), after introduction of quarantine measures.
On the next stage of our analyses we aimed to decipher the need in health care professionals at a country level depending on the fact of implementation of quarantine measures. At the peak of COVID-19 outbreak if no quarantine is applied, there will be a daily need in 12,026 ICU doctors and 58,144 ICU nurses, while introduction of quarantine may potentially reduce these numbers to 500 and 2,420, respectively. Likewise, lack of quarantine measures will necessitate the availability of 707 dialysis practitioners and 589 extracorporeal membrane oxygenation (ECMO) practitioners, while implementation of quarantine will can help to reduce these numbers to 29 and 24 practitioners, respectively. Besides, 168,576 ward nurses will be needed in the country if no intervention is applied as compared to just 7,982 nurses in case of quarantine implementation (Tables 4 and 5).
Table 4
Forecast of health care workers capacity during COVID-19 outbreak in Kazakhstan without intervention measures

Table 5
Forecast of health care workers capacity during COVID-19 outbreak in Kazakhstan with introduction of quarantine measures

DISCUSSION
This study aimed at epidemiological elucidation of COVID-19 outbreak in the Republic of Kazakhstan and at predictive modeling of cases, deaths, and recoveries, as well as needs in professional workforce depending on implementation of quarantine measures. To the best of our knowledge, this is the first study devoted to epidemiology of COVID-19 outbreak in the Republic of Kazakhstan. The vast majority of symptomatic patients in this study have mild disease manifestations and the proportion of moderate disease is around 10%. Refusal to implement quarantine measures will result in 156 thousand hospitalized patients due to severe illness and in 15.47 thousand deaths at the peak of an outbreak. Besides, this will substantially increase the need in professional medical workforce. Still, 50% compliance with quarantine measures could potentially reduce the number of deaths up to 3.75 thousand cases and the number of hospitalized patients up to 9.31 thousand cases at the peak. Also, this may decrease the demand for medical professionals alleviating the burden placed on Kazakhstani health care system.
Having the SEIR model and parameters in hand, simulations could be carried-out for a longer time period and thus, predict the potential trends of COVID-19 outbreak both at the national and local levels. Simulation models could also evaluate the impact of different intervention scenarios.21 Other studies across the globe show good agreement between SEIR modeling and official data that fall within 95% CI. In China, the forecasted values were higher than the actual ones, which was attributed to the effectiveness of anti-epidemic measures undertaken by the country government.22 In Italy, the forecast modeling of COVID-19 outbreak showed high accordance with the real data.23
Communitywide protective measures, such as quarantine, social distancing and closure of schools and childcare facilities are broadly implemented throughout COVID-19 pandemic and Kazakhstan is not the exception. Although being effective, these measures present rather challenging issue as they might be very disruptive, and require adequate planning and community engagement.24 A recently published rapid systematic review concludes that home quarantine is not very cost-effective and should be started when pandemic just began. The authors emphasize that testing and contact tracing with rapid isolation of infected individuals–a strategy that is also undertaken in Kazakhstan–appears to be more cost-effective than quarantine.25 Apart from social and economic costs, home quarantine is associated with mental distress, as it leads to confusion, anger, and posttraumatic stress syndrome, which may have long-lasting negative effects.26
Still, quarantine measures undertaken by other countries have proven to be effective in controlling the spread of COVID-19.2122 Despite early introduction of quarantine in Kazakhstan, the outbreak continues to escalate, probably because many infected individuals have not been identified yet. This phenomenon could be explained in two different ways. First, many infected individuals remain asymptomatic and this proportion could be as high as 40%–50%.27 These individuals are not identifiable at the community level and along with those who are presymptomatic or have only mild symptoms are not likely to seek medical care. Second, individuals with known exposure, like asymptomatic/presymptomatic foreign travelers, do not readily follow the recommendations on self-isolation. Taking into consideration that inadequate compliance with quarantine leads to community transmission of SARS-CoV-2 to the susceptible individuals, this explains the continuing community spread.
As COVID-19 outbreak evolves, the scarcity of health care resources becomes a major challenge. No country in the world is prepared for rapidly increasing needs in ICU resources, including beds, equipment and professionals. In India allocation of one third of ICU beds for COVID-19 alone would result in troubling effects among other patients presenting with serious conditions requiring ICU care.28 The actual number of ICU beds available in Kazakhstan is not officially reported although the Ministry of Health made efforts to equip existing ICUs with additional mechanical ventilators and ECMO machines. However, if COVID-19 outbreak takes the negative scenario, the newly emerged patients in critical condition will completely overwhelm the health care system of Kazakhstan.
Severe cytokine activation or cytokine release syndrome (CRS) is an acute systemic inflammatory response and might be the cause of lethal outcome in otherwise healthy individuals affected by COVID-19.29 The cause of CRS is the activation of bystander immune cells and endothelial cells due to the binding of CAR T-cell receptor to its antigen. In turn, activation of bystander immune cells results in mass production of cytokines and pathophysiological cascade of subsequent events.30 Because COVID-19 patients with CRS carry worse prognosis, it is important to recognize it early in order to provide an adequate therapeutic response.31
In general, effective tackling of COVID-19 outbreak has several side aspects and improved patients satisfaction is one of them. As this outbreak caused multiple problems for the population of Kazakhstan, it is worth to maintain trust in such international organizations as the WHO32 and also in local health care providers, which became undermined over recent years.33 For this, it might prove to be useful to provide adequate information on outbreak status in a timely manner and to initiate an open dialog with general public, which could be done via social media.
The outcomes of our study could be of interest for policymakers as they help to forecast the trends of COVID-19 outbreak, the demands for professional workforce, and to estimate the consequences of quarantine measures. Our study results based on combination of official data on COVID-19 outbreak in Kazakhstan and SEIR modeling, suggest that 50% compliance with quarantine measures could potentially reduce the number of cases. According to available international reports, introduction of quarantine may provide beneficial effects. In reality, Kazakhstan initiated quarantine very early and combined it with other community protection measures, including closure of all educational establishments, restriction of travels and cleaning with disinfection in public places. Thus, this model is likely to show exaggerated results and the real situation can be more optimistic if the country government will not cease the interventions preliminary. We hope that this simulation can be useful for managing COVID-19 outbreak in Kazakhstan, as well as in other countries that are still at an early stage of COVID-19 epidemic.
 XML Download
XML Download