

 PDF
PDF Citation
Citation Print
Print




INTRODUCTION
Distinguishing major depressive disorder (MDD) from bipolar disorder (BD) remains a difficult task in the clinical setting, due to their similarities during depressive episodes.1 BD misdiagnosis and subsequent treatment with antidepressants can result in severe mania, hypomania, or rapid cycling.2 In particular, diagnosis is challenging in pre-pubertal and adolescent patients, as their symptoms may not meet the DSM-IV criteria.3 Also, studies suggest that even during the euthymic state of BD, cognitive and functional abnormalities can persist.4 Thus, biomarkers for BD would be very useful in early diagnosis, disease control, measuring treatment response, and developing new therapeutic methods. While many serum markers, brain scans, and genetic variability have been tested for use in BD diagnosis, no reliable biomarker has yet been determined.5
One biological axis of importance in mood disorders is the purinergic system. Uric acid (UA) is a product of adenosine catabolism.6 UA and adenosine help regulate neurons in the CNS; in particular, activated adenosine receptors reduce neuronal excitability and decrease serum UA.7 Higher purine turnover in the brain was shown to result in peripheral clearance of UA, which also correlated with hallucinations, suicidality, and mania.8 Based on the putative relationship between BD and the purinergic system, many studies have explored possible treatments. Allopurinol, a drug that treats gout by reducing UA levels, was shown to reduce manic symptoms and increase remission rates when used as an add-on treatment for BD.91011
Thus, an association between BD and UA seems likely, but whether UA can serve as a biomarker continues to be a topic of debate. A meta-analysis conducted by Bartoli et al.12 suggested that 1) BD patients have higher serum UA than healthy controls to a moderate-large degree, 2) BD patients have higher serum UA than MDD patients to a moderate degree, and 3) BD manic phase shows higher serum UA than depressive phase to a small degree; however, the second and third conclusions were limited by a lack of sex and age comparability. Recent studies also delve into the question of whether UA may be used as a trait or a state marker of BD. Some studies suggest that UA may be used as a trait marker. Dos Santos Oliveira et al.13 retrospectively observed that MDD patients with higher UA levels were more likely to convert to a diagnosis of BD in the following 10 years. On the other hand, some results suggest that UA may be used as a state marker. Tatay-Manteiga et al.14 saw no differences in UA levels among euthymic BD patients, their siblings, and genetically different healthy controls, suggesting that UA may account for only the acute stages of BD.
Studies in the Korean population showed that higher UA levels significantly correlated with metabolic syndrome factors such as obesity and high blood pressure.1516 To the best of our knowledge, however, none of the studies comparing UA in BD and MDD had controlled body mass index (BMI) as a variable, and available studies considering sex, age, and psychiatric medication were inconsistent. In this cross-sectional, retrospective study, we hypothesized that UA levels of BD patients would be higher than those of MDD patients. With the consideration of factors such as BMI, sex, age, and psychiatric medication use, we aimed to provide a clearer comparison of UA levels between BD and MDD patients.
Go to : 
METHODS
Subjects
Our retrospective chart review study included patients admitted to Seoul National University Hospital Psychiatry Inpatient Unit and diagnosed with MDD or BD.
The admission data were collected using a program called SUPREME (www.supreme.snuh.org), the hospital's automated electronic medical record screening program. The program isolated the data of patients admitted to the psychiatric inpatient unit between January 1, 2015 and December 31, 2018, aged 19–60 years, and whose main discharge diagnosis was either MDD (F32.0-33.9) or BD (F31.0-31.9) according to the ICD-10 (International Statistical Classification of Diseases and Related Health Problems—10th Revision). Data such as sex, age, date of birth, BMI, admission date, discharge date, diagnosis, serum UA examination date, and serum UA level were exported. For patients with multiple admissions, clinical data from only the most recent admission were used.
As the comorbidities of the patients were unclear from the available records, their medication usages the day before UA examination were used to infer the presence of medical conditions that may impact UA levels. Therefore, patients on medication for an autoimmune disorder, liver disorder, gout, hypertension, hypercholesterolemia, diabetes, and thyroid disorder were excluded. Patients with cancer and patients on corticosteroids, anti-inflammatory drugs, and narcotics were also excluded.
Each patient's psychiatric medication usage the day before the UA examination was assessed and categorized into mood stabilizer, antipsychotic, or antidepressant use. The mood stabilizer agents were lithium, valproate, oxcarbazepine, topiramate, lamotrigine, pregabalin, and lacosamide. The antipsychotic agents were risperidone, aripiprazole, haloperidol, clozapine, olanzapine, quetiapine, sulpiride, chlorpromazine, paliperidone, ziprasidone, blonanserin, and amisulpride. The antidepressant agents were escitalopram, vortioxetine, bupropion, sertraline, paroxetine, fluoxetine, desvenlafaxine, venlafaxine, duloxetine, tianeptine, amitriptyline, nortriptyline, trazodone, mirtazapine, imipramine, milnacipran, clomipramine, and fluvoxamine.
Assessing serum UA
The serum UA measurements were made during the routine, standard bloodwork of inpatients. Our hospital uses the TBA-FX8 automated clinical chemistry analyzer (Toshiba, Tokyo, Japan) for blood analyses.
Statistical analysis
Statistical analyses were performed using SPSS (version 25.0; IBM Corp., Armonk, NY, USA). For comparisons of variables between the MDD and BD groups, the independent t-test was used for continuous variables, and Pearson's χ2 test was used for categorical variables. The comparison of UA levels in medication user and non-user groups was performed with independent t-tests in order to choose the confounding variables to include in the subsequent logistic regression analysis. Logistic regression analysis was carried out, with BD diagnosis as a dependent variable, and UA levels, age, sex, and BMI as covariates. Additionally, the types of medication that were associated with UA levels in the previous independent t-tests were respectively controlled for, to see if the usage of these medications influenced our results.
Ethics statement
This study was approved by the Institutional Review Board (IRB) of Seoul National University Hospital (approval No. 1910-187-107). Due to our retrospective and non-invasive study design, informed consent requirement was waived by the IRB.
Go to :
RESULTS
The SUPREME program yielded a total of 914 inpatient data entries. After the inclusion of data from only the most recent admission for patients with multiple admissions, the number of potentially eligible patients was 542, including 242 MDD and 300 BD. Among them, 166 patients with medical conditions and on medications that affect UA levels were excluded, leaving the final number of eligible patients at 376, with 142 MDD and 234 BD. The flow diagram for the sample selection process is shown in Fig. 1.
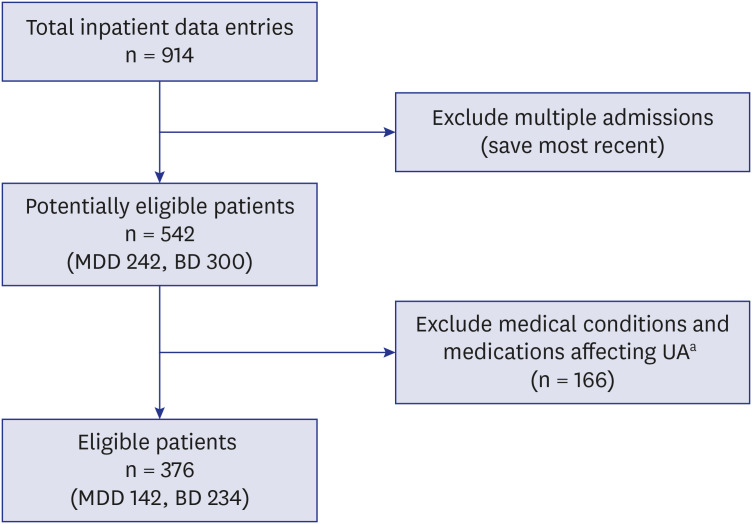 | Fig. 1Flowchart of sample selection. From 914 total available inpatient data entries, multiple admissions were excluded in order to include only the most recent admission entry of each patient. From the 542 patients, those with medical conditions and those on medications affecting uric acid levels were excluded. The final eligible patient number was 376, including 142 patients with major depressive disorder and 234 patients with bipolar disorder.MDD = major depressive disorder, BD = bipolar disorder, UA = uric acid.
aMedical conditions: cancer, autoimmune disorder, liver disorder, gout, hypertension, hypercholesterolemia, diabetes, and thyroid disorder. Medications: corticosteroids, anti-inflammatory drugs, and narcotics.
|
The comparison of variables showed that in our selected sample, MDD patients are significantly older, have lower BMI, use fewer mood stabilizers and antipsychotics, use more antidepressants, and have lower serum UA levels compared to BD patients. The specific values are presented in Table 1.
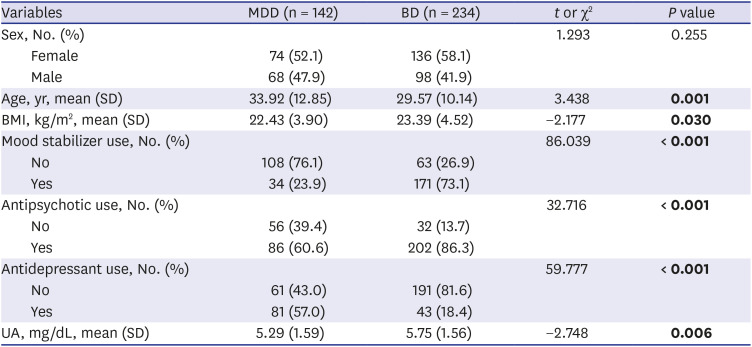
Table 1
Demographic and clinical characteristics of the sample
P < 0.05 are marked in bold.
MDD = major depressive disorder, BD = bipolar disorder, SD = standard deviation, BMI = body mass index, UA = uric acid.
![]()
To assess whether mood stabilizer, antipsychotic, or antidepressant use may be confounding factors for comparing UA levels, independent t-tests were performed on UA levels of medication user and non-user groups. In the mood stabilizer group, UA levels of the non-user group were lower than those of the user group (5.31 ± 1.56 mg/dL vs. 5.80 ± 1.58 mg/dL, P = 0.003). In the antipsychotics group, UA levels of the non-user group were also lower than those of the user group (5.25 ± 1.49 mg/dL vs. 5.68 ± 1.60 mg/dL, P = 0.024). In the antidepressants group, UA levels of the non-user group were not different from those of the user group (5.63 ± 1.56 mg/dL vs. 5.47 ± 1.64 mg/dL, P = 0.348) (Table 2). Therefore, we confirmed that mood stabilizer and antipsychotic use may be relevant confounding variables in our sample analysis.
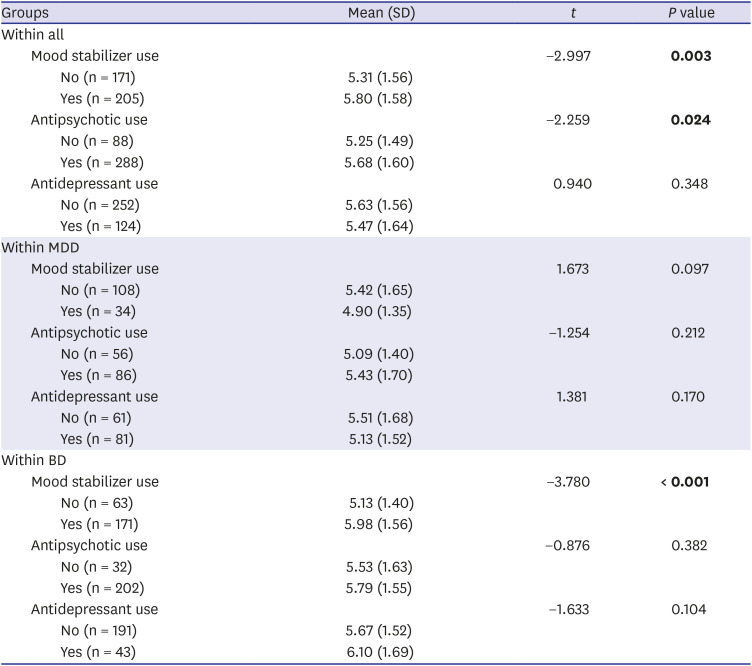
Table 2
Independent t-test results comparing the serum uric acid (mg/dL) of different groups
P < 0.05 are marked in bold.
SD = standard deviation, MDD = major depressive disorder, BD = bipolar disorder.
![]()
Logistic regression analysis results showed that UA levels were still significantly associated with the likelihood of a BD diagnosis after controlling for sex, age, and BMI (odds ratio [OR], 1.410; 95% confidence interval [CI], 1.150–1.728; P = 0.001) (Table 3). Additionally, UA levels were still significantly associated with the likelihood of a BD diagnosis after further control for mood stabilizer use (OR, 1.263; 95% CI, 1.014–1.573; P = 0.037) or antipsychotic use (OR, 1.351; 95% CI, 1.092–1.670; P = 0.005).

Go to :
DISCUSSION
We found that higher UA levels significantly indicate the likelihood of a BD diagnosis rather than an MDD diagnosis. This result follows that of other similar studies. Albert et al.17 saw that BD patients have higher serum UA levels in comparison to age- and sex-matched patients with MDD, obsessive-compulsive disorder, or schizophrenia. Wen et al.18 and Bartoli et al.19 also saw that depressed patients had lower serum UA levels than patients with BD. On the other hand, Wiener et al.20 found no association between UA levels and diagnosis of BD or MDD. The apparent discrepancies may be due to differences in the sample characteristics or the choice of control variables, such as sex, age, metabolic parameters, psychiatric drugs, and pharmacological drugs. Because of the relevant ease with which UA can be measured in each patient, it may have a promising utility as a biomarker in the clinical setting. Bartoli et al.19 did not see a correlation between the behavioral features of BD or MDD and serum UA levels. However, Dos Santos Oliveira et al.13 showed that MDD patients with higher serum UA levels were significantly more likely to convert to BD in 10 years. Thus, while UA levels may not predict symptom severity, it may be used as a trait marker to predict BD conversion in MDD patients. Whether UA levels can function as a state or a trait marker is an ongoing question. Albert et al.17 saw no differences in UA levels among manic, depressive, and euthymic BD states, while Muti et al.21 saw that the patients with manic/mixed BD states had significantly higher UA levels compared to those with euthymic or depressive states. In our study, the data screening program could not export the episodic state of a patient; thus, we were not able to divide the BD patients into mood state groups. We suggest that an important follow-up study would involve a comparison of the UA levels in different BD states to those of MDD. To our knowledge, we are the first to include BMI and psychiatric drug usage in the analysis and also to thoroughly vet medical conditions that may influence UA levels. Although we were not able to test UA as a state marker, our results thus far show a strong promise for the use of UA levels in distinguishing between BD and MDD.
Our finding that UA levels are higher in patients with BD compared to MDD adds to the hypothesis that purinergic dysfunction underlies the biology of mood disorders. The most prevalent adenosine receptor, A1, resides in high concentrations in the hippocampus, cortex, cerebellum, and thalamus, and its activation causes membrane hyperpolarization, a decrease in UA levels, and a reduction in neuronal postsynaptic calcium influx. Thus, decreased adenosine activity and high UA levels have been related to mania.222324 Ortiz et al.8 compiled an extensive review summarizing the physiology of the purinergic system and its relation to mood disorders: UA levels correlated with an increased incidence of hallucination, suicidality, and mania; adenosine receptor downstream signaling markers cAMP, protein kinase C, and intracellular calcium levels in manic patients were altered; and BD patients were at higher risk of developing gout in a nationwide study.222526 Burnstock27 also wrote a general review on purine receptors and their potential therapeutic targets: the P2X7 receptor gene showed involvement in both MDD and BD, and A1, A2a agonists (subsets of P1) and P2Y1 antagonists were suggested as possible treatment targets for depression and anxiety.2829
Because we did not have a sufficient number of drug-free patients, to control for psychiatric medication usage, we decided to look at the three categories—mood stabilizers, antipsychotics, and antidepressants—in our analysis. These three categories comprise the psychiatric drugs most commonly used by patients with BD and MDD. A limitation of our study is that each drug within the three categories has its unique action and, therefore, possibly a different effect on the serum UA levels. Duration or dosage of the medications could not be considered either. Thus, our results cannot suggest whether mood stabilizers, antipsychotics, or antidepressants as a categorical drug class raise or lower serum UA levels. What our data do suggest is that, in our sample, BD significantly correlates with higher serum UA levels, after accounting for the three categories of medication use. In future studies, perhaps an ideal analysis would categorize the psychiatric medications into the following two groups: those expected to raise serum UA levels and those expected to lower serum UA levels. For such groupings to be possible, a comprehensive review of each psychiatric medication's effect on UA levels and/or other metabolic parameters would be necessary; as yet, there is none. Following is a summary of the currently available studies on monotherapy treatment and UA levels: lithium, carbamazepine, and phenytoin lower UA levels, while valproate, phenobarbital, haloperidol, and risperidone increase UA levels.30313233 It would be of interest to explore the commonly used psychiatric medications' effects on serum UA levels. Also, drug use tends to correlate with disorder severity; the higher UA levels could be an indication of the acuteness of a bipolar episode rather than the drug effect itself. To assess this relationship, a future study on a drug-naïve group or one incorporating measurement of both drug usage and symptom severity would be necessary.
A further limitation of our study is that our sample consisted only of inpatients at a single hospital, leaving room for selection bias and restricting the generalizability of the results to patients with mild to moderate symptoms. However, Kesebir et al.34 saw similarly higher UA levels in patients with BD than those with MDD when looking at outpatients in remission for at least 8 weeks. Therefore, the UA levels may be consistently high in patients with BD regardless of varying symptom severities.
Another limitation of our study is its cross-sectional design, due to which the full progress of the disease could not be analyzed. Some patients with BD may have been wrongly diagnosed with MDD at their discharge in the study's selected time period. Further, due to a lack of consistent records, alcohol use, smoking, caffeine intake, and dietary patterns could not be considered, all of which may impact UA levels.
In short, our study indicates that patients with BD are significantly likely to have higher serum UA compared to patients with MDD. The strength of our study lies in the exploration of important confounding factors, including BMI and psychiatric drug usage. Further studies of interest may include a comparison with healthy controls and an investigation of parameters associated with UA levels, such as inflammatory markers and kidney function.
Go to :
 XML Download
XML Download