

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
In healthcare policy and research, summary measures regarding the burden of disease and injuries are needed for priority setting and rational allocation of limited resources (including budget).12 In this context, during the 1990s, Alan D Lopez and Christopher J.L. Murray developed disability adjusted life year (DALY), an indicator that can comprehensively measure the health status of a population. DALY is the sum of years of life lost due to premature death (YLL) and years lost due to disability (YLD).2 DALY is meaningful in that it expresses the health status of a population as a comprehensive quantitative indicator, rather than segmenting it by morbidity and mortality. It is being used as the representative indicator for measuring the global burden of disease in the Global Burden of Disease (GBD) study. In particular, the World Health Organization used YLD, a component of DALY, to estimate health-adjusted life expectancy (HALE), which is used as key evidence when prioritizing policies or allocating budget.
To combine YLL and YLD into the indicator of DALY, YLD must be estimated by the disability weight (DW). DW represents a measured value of specific health status and severity of the disease, with values ranging between 0 (perfect health) and 1 (equivalent to death). Therefore, DW acts as a bridge between disease morbidity and mortality.3 In this context, DW of a specific disease must be set to accurately reflect the average characteristics of that disease. In other words, the relative severity of diseases must be well reflected in DW.
Research on DW has evolved along with the GBD study. In the 1990 GBD study, investigation using visual analogue scale (VAS) and person trade off (PTO) with 10 public health specialists produced DWs for 483 health conditions corresponding to 131 diseases and injuries.4 Since 1996, several studies have been conducted to estimate DW in a variety of countries.35678 However, the methodology, validity, and universality of DW estimation are not adequately clear.910 DWs used in the 2010 GBD study were estimated based on a household questionnaire and online surveys administered to 30,230 people in 5 countries (the United States, Peru, Tanzania, Bangladesh, and Indonesia). Paired comparison and population health equivalence (modified from a PTO) were used as valuation methodologies.11 As an upgrade, the 2013 GBD study used DWs that reflected those from studies conducted in 4 European countries (the Netherlands, Sweden, Hungary, and Italy).12 However, despite such attempts at a methodological upgrade, many scholars still question the validity of methodology for estimating DWs.131415 Nord13 criticized that the agreement between countries for DWs used in the 2010 GBD study was exaggerated. The DW associated with each health condition is currently fixed across all social, cultural, and environmental contexts.16
In this context, there is an ongoing effort since 2000 to estimate DW that reflects the unique social and cultural context of Korea.3171819 Most DW studies conducted in Korea have targeted people who received medical education to allow more objective and broader assessment of disease characteristics.31718 Although reflecting preferences of the general population is required for priority setting and rational allocation of limited resources, the general population may have biases about disease status and may not be able to determine the severity of the diseases that are not very well-known. Therefore, careful consideration of the target population for estimating DWs is important.
Moreover, the issue of the size of DW needs to be studied as well. Although a direct comparison may be difficult, the DWs used in the 2015 Korean National Burden of Disease (KNBD) study showed regular distribution around the value of 0.5 (normal distribution), whereas the DWs used in the GBD study were lower than those of the 2015 KNBD study. For example, Alzheimer disease and other dementias had DW of 0.069, 0.377, and 0.449 for mild, moderate, and severe cases in the GBD study,12 respectively, whereas the DW used in the 2015 KNBD study had the value of 0.736.18 Such a difference can significantly affect the size of YLD and even influence HALE.
The present study aimed to estimate cause-specific DWs based on the opinion of medical professional experts and discuss the differences found. Furthermore, the study also aimed to compare and assess the size of DW according to two analytical methods and estimate the most reasonable DW from the YLD and HALE estimation perspective. Accordingly, the study aimed to derive the Korean version DW update by estimating DWs according to the severity of major diseases.
METHODS
Study design and participants
A self-administered web-based survey was conducted based on the methodology of previous studies for estimating DWs.318 The survey was performed from November 2018 to December 2018. In order to explore the possibility of expanding the participants in the survey, we included nurses and oriental medical doctors as well as physicians and medical students (third or fourth grade of a regular course). Participants were recruited through the promotion of the survey in the online community site for medical professionals and by word-of-mouth from other participants.
Valuation method and causes of disease
First, participants responded to their age group, sex, occupation, and specialty. Next, the participants assessed the severity of the causes of disease by using a ranking method. We used the complete ranking method listing five alternatives in view of the effectiveness and feasibility demonstrated in previous studies.31820 The participants ranked the five listed causes of disease in order of good health, considering the seriousness of the physical and mental problems caused by the diseases. The descriptions of the causes of disease were not presented to the participants and they judged the severity by looking at the names of the presented causes of disease.
A total of 313 causes of disease were used in this survey. The list of causes of disease utilized in this study is based on the GBD 2016 study.21 In the GBD 2016 study, DALY and YLD were calculated for 333 and 328 causes of disease, respectively. After reviewing the list of the causes of disease from GBD 2016 study, 277 causes of disease were selected after considering duplication of causes of disease and the possibility of emerging causes of disease in Korea. Among the 277 causes of disease, 14 causes of diseases were subdivided by the degree of severity. For example, major depressive disorder was subdivided into ‘major depressive disorder (mild),’ ‘major depressive disorder (moderate),’ and ‘major depressive disorder (severe).’ In the case of diabetes mellitus, the severity was classified as the presence (‘diabetes mellitus with complications’) or absence of complications (‘diabetes mellitus without complications’). Furthermore, ‘allergic rhinitis,’ ‘atopic dermatitis,’ and ‘metabolic syndrome,’ which were not included in the GBD 2016 study, were included in the list to calculate the magnitude of the problem in Korean National Burden of Disease study. ‘Full health’ and ‘being dead’ were also included in the list to identify participants who made illogical responses and to use them as anchor points in the analyses.
Participants conducted a total of 20 ranking methods to evaluate five alternatives. Among the 311 causes of disease (excluding ‘full health’ and ‘being dead’), 5 randomly selected causes of disease were given to participants in each ranking method question. However, ‘full health’ was fixed as the first cause of disease in question 1 and the fifth cause of disease in question 11. Similarly, ‘being dead’ was fixed as the first cause of disease in question 5, fifth cause of disease in question 10, the first cause of disease in question 15, and the fifth cause of disease in question 20.
Analysis
Descriptive analyses were performed to determine the socio-demographic characteristics of the participants. Before proceeding with the analyses of DWs, only the responses of participants who answered ‘full health’ in questions 1 and 11 with the best health state were included in the analyses. Then, the ranked data were converted into paired comparison data in accordance with previous studies.31820 For example, if the response of a participant was in the order of C1-C2-C3-C4-C5, it was converted to C1-C2, C1-C3, C1-C4, C1-C5, C2-C3, C2-C4, C2-C5, C3-C4, C3-C5, and C4-C5. Thus, paired comparison data were obtained by ranking method listing five alternatives. Probit regression analysis was conducted with these paired comparison data. The stated preference of the first cause of disease in the paired comparison was regarded as the dependent variable. The two causes of disease that were compared were considered as independent variables and ‘being dead’ was treated as a reference of the dummy variable. Using the coefficient estimates of the probit regression, the predicted probabilities of causes of disease were calculated.
In the process of rescaling predicted probability to DW on a scale from 0 to 1, two models were used. Model 1 was to rescale considering the normal distribution of DWs as in previous studies.318 In Model 2, predicted probabilities taking the natural logarithm were rescaled considering the asymmetric distribution of DWs. ‘Being dead (1)’ and ‘full health (0)’ were used as anchor points in both Models. Subgroup analyses were also performed according to the occupation of participants. Group 1 comprised physicians and medical students as in the previous studies,318 whereas Group 2 comprised nurses and oriental medical doctors. We determined the frequency distributions of the DWs from the models and calculated the Pearson correlation coefficients to compare the DWs from the models to those obtained in the most recent Korean DWs study.18
We used Stata 13.1 software (StataCorp, College Station, TX, USA) for all statistical analyses. In this study, P value less than 0.05 was regarded as statistically significant.
Ethics statement
This study was approved by the Institutional Review Board (IRB) of the Ulsan University Hospital (IRB No. 2018-11-034). All participants were informed about the purpose and process of the study and only those who agreed to participate joined this survey. Each participant received a 9,000 won coffee coupon.
RESULTS
A total of 901 participants started the survey and 872 participants completed the survey. Among 872 participants, 66 participants were excluded from the analyses due to illogical responses such as ‘full health’ was not listed as the best health state. Table 1 summarized the details of the socio-demographic characteristics of 806 participants used in the analyses. Most participants were in the 30s and about 70% were male. About two-thirds of the participants were specialists and there were more medical specialists than surgical specialists. Group 1 comprised only physicians and medical students and group 2 comprised only nurses and oriental medical doctors and included were 682 and 124 participants, respectively.
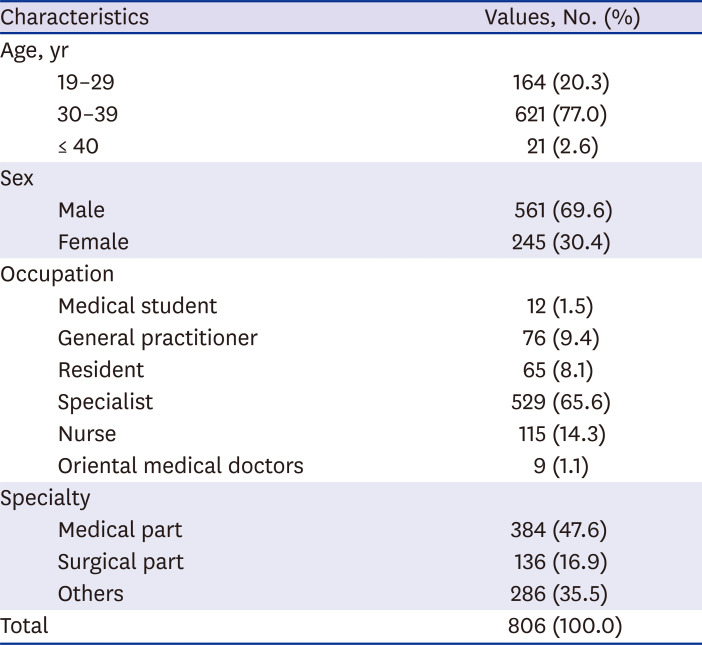
Table 1
Characteristics of the study participants
![]()
Table 2 shows the DWs by the model of analysis for each group. The mean of the DWs according to the models in each group was 0.490 (Model 1 in Group 1), 0.378 (Model 2 in Group 1), 0.506 (Model 1 in Group 2), and 0.459 (Model 2 in Group 2), respectively. In all analyses, ‘Pancreatic cancer’ had the highest DW as follows: 0.929 (Model 1 in Group 1), 0.724 (Model 2 in Group 1), 0.996 (Model 1 in Group 2), and 0.986 (Model 2 in Group 2). On the other hand, the cause of the disease with the lowest DW was acne vulgaris in Model 1 in Group 1 (0.059) and Model 2 in Group 1 (0.229). Cause of disease with the lowest DW differed according to the analysis method. Acne vulgaris, caries of deciduous teeth, and allergic rhinitis had low DWs overall.

Table 2
Disability weights from each model for the subgroups
![]()
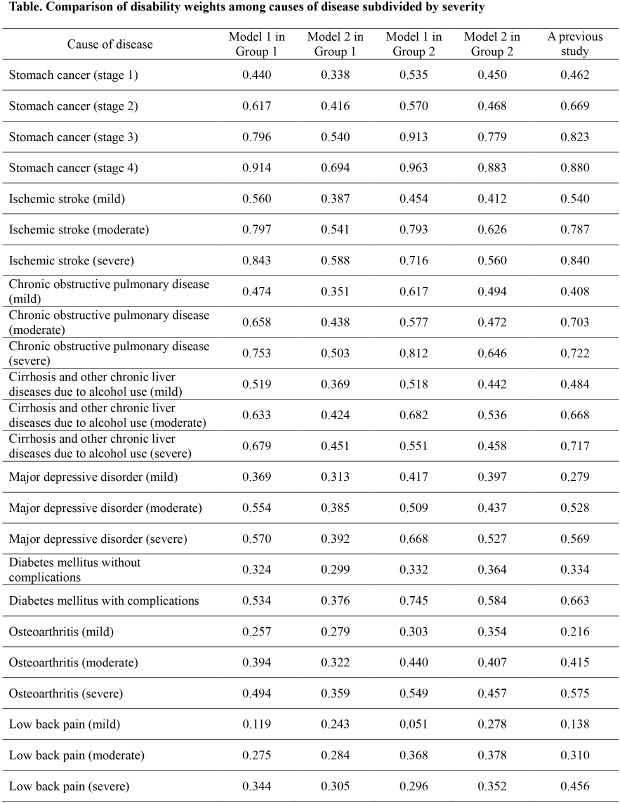
The DWs of causes of disease that were classified by severity are shown in Table 3. Furthermore, Table 3 also shows the DWs calculated from a previous study for comparison.3 In the results of Group 1, there was no case where the DWs were reversed according to severity. However, in Group 2, there were some cases in which DWs were reversed according to severity. For example, among the results of ‘Model 2 in Group 2,’ the DW of ‘Ischemic stroke (moderate)’ was 0.626, but that of ‘Ischemic stroke (severe)’ was 0.560. In addition, the results of Model 2 showed that the DWs were generally low in causes of disease with high severity, compared with those from a previous study. For example, in the case of ‘trachea, bronchus, and lung cancers (stage 4),’ the DW of the previous study was 0.906, but that of ‘Model 2 in Group 1’ was estimated to be 0.692.
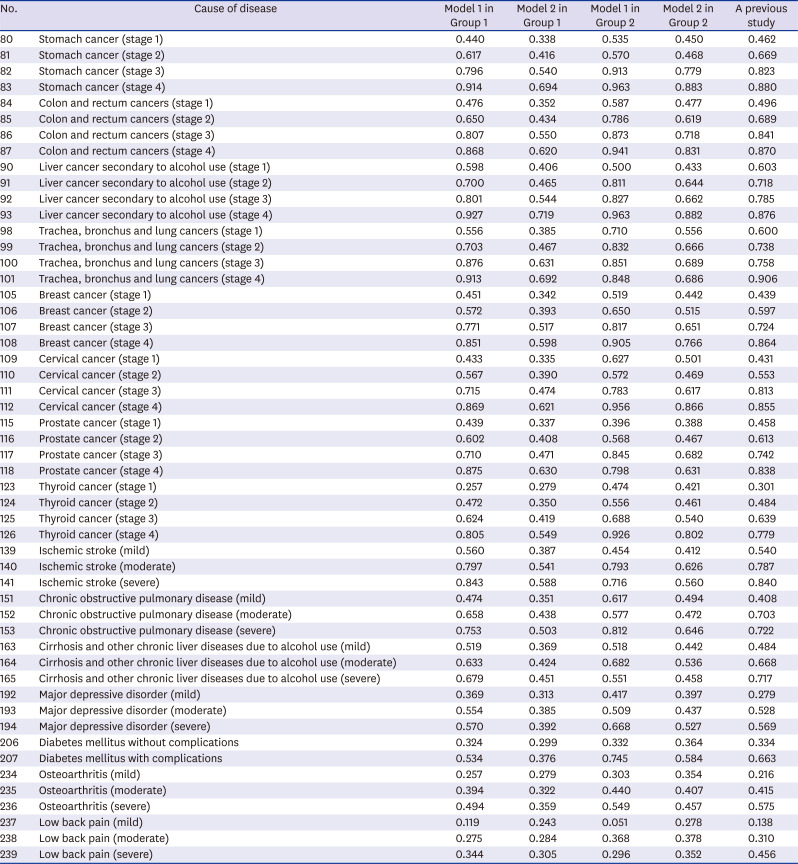
Table 3
Comparison of disability weights among causes of disease subdivided by severity
![]()
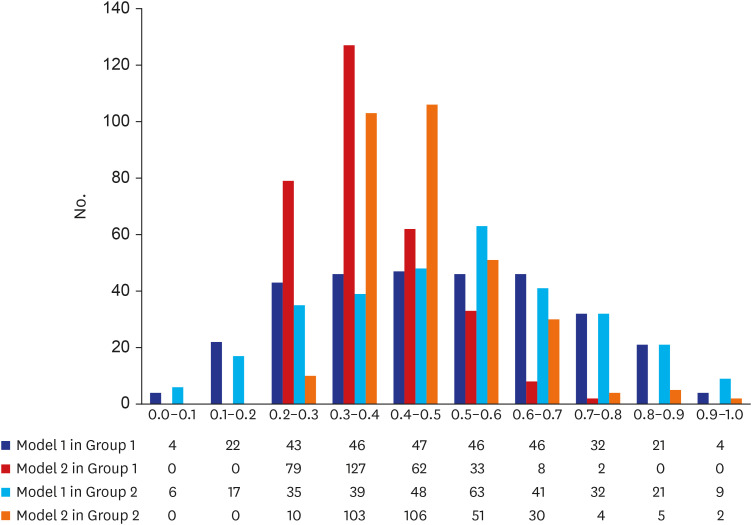
Fig. 1 shows the distributions of DWs in all analyzes. The distributions of DWs for ‘Model 1 in Group 1’ and ‘Model 1 in Group 2’ were close to normal distribution. However, the distributions of DWs for ‘Model 2 in Group 1’ and ‘Model 2 in Group 2’ were right skewed. About two-thirds of the causes of disease had DWs of 0.2 to 0.4 in ‘Model 2 in Group 1.’ Furthermore, in ‘Model 2 in Group 1,’ there was no cause of disease with a DW of more than 0.8 or less than 0.2.
The correlations between the DWs for 200 overlapping causes of disease from a previous study18 and this study are shown in Fig. 2. The Pearson correlation coefficient was highest in ‘Model 1 in Group 1 (0.975)’ and lowest in ‘Model 2 in Group 2 (0.867).’ When the DWs of Model 1 in Group 1 were compared with those of the previous study, a total of 96 causes of disease had decreased DW, but 104 causes had increased DW (Supplementary Table 1). However, when the DWs of ‘Model 2 in Group 1’ were compared to the previous study, a total of 155 causes had decreased the DW, but 45 causes had increased DW. In particular, the DW of the ‘Cervical cancer (stage 3)’ in ‘Model 2 in Group 1 (0.474)’ decreased by 0.338 compared to the previous study (0.813). However, the DW of ‘Falls’ in ‘Model 2 in Group 1 (0.370)’ increased by 0.205 compared to the previous study (0.165).
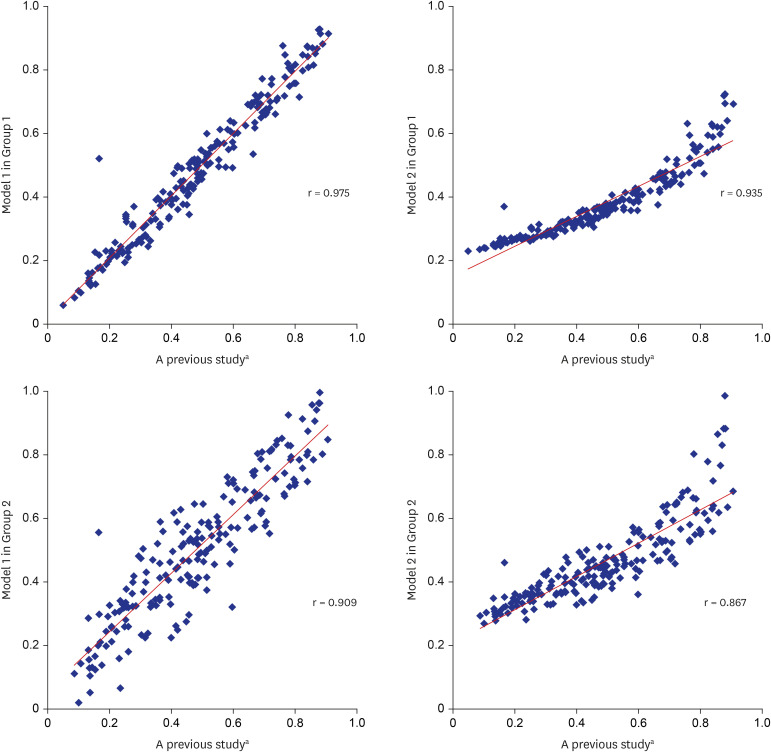
Fig. 2
Correlation of disability weights between a previous study and this study.
aData from the most recent Korean disability weights study.18
![]()
DISCUSSION
In this study, we updated the methodology to obtain reasonable DWs for the calculation of DALY and HALE. Specifically, we attempted to determine whether DWs could be calculated for physicians and medical students as well as nurses and oriental medical doctors. In addition, we attempted to identify an optimal model for calculating valid DWs through evaluating the size and distribution of DWs as well as correlation with previous research results and reversal of DW according to the severity of diseases. The survey method and the analytical model for the calculation of DWs, which have been proved through this study, can be used in the calculation of the DW in other countries.
Above all, it is significant because a large number of medical professionals participated in this DW study. Most of the studies on DW conducted for medical professionals were performed by dozens of participants.22 A total of 901 medical professionals participated in the survey and responses of 806 medical professionals were utilized in the analyses. The number of participants was higher than that in the most recent DW study in Korea involving 605 physicians and medical students. Although healthcare professionals have a wealth of knowledge about a variety of health conditions and diseases and can objectively compare and evaluate diseases, questions can arise as to whether they can objectively compare and evaluate diseases as the area of expertise of healthcare professionals becomes increasingly fragmented.23 This limitation may be overcome by more healthcare professionals with diverse specializations participating in DW survey.
In this study, we included nurses and oriental medical doctors as participants of this study. A total of 115 nurses and 9 oriental medical doctors participated in the survey and the results of these responses were analyzed in Group 2. In Group 2, there were some cases in which DWs were reversed according to severity, while there was no case where the DWs were reversed according to the severity in Group 1. Nurses and oriental medical doctors who participated in this study were still unfamiliar with the DW study and seem to have an inconsistent response. In previous studies, healthcare professionals or medical experts have been used extensively in DW studies, but few have specifically identified who will be healthcare professionals or medical experts.2223 Based on the results of this study, it is difficult to make a quick judgment on whether nurses or oriental medicine doctors are not worthy of participating in DW study. However, careful attention should be paid to including medical professionals unconditionally in DW survey, simply because they have medical qualifications. In the DW study, it will be important to educate participants to understand the significance of DW and to make a consistent assessment of the disease during the survey.24
In this study, we attempted to revise the analysis method to obtain valid DWs. The DWs estimated in the previous KNBD studies showed normal distribution,318 whereas the DWs calculated in the GBD studies showed right-skewed distribution. Accordingly, the estimated DWs in KNBD studies were somewhat higher than those in the GBD study. For example, the DWs for ‘anorexia nervosa’ and ‘bulimia nervosa’ were 0.224 and 0.223 in the GBD 2013 study,12 respectively, but 0.420 and 0.392 in the most recent KNBD study,18 respectively. In fact, it is not easy to assess which DWs are valid, but such difference can significantly affect the size of YLD and even influence HALE in KNBD studies. Therefore, this study attempted to revise the method of calculating the DWs considering the distribution assumption of the DWs in the GBD study. In other words, we compared the results of the analytical model assuming a normal distribution of DWs (Model 1) and the results of an analytical model assuming a right-skewed distribution of DWs (Model 2).
As a result, it was confirmed that the DWs in Model 2 was estimated to be smaller than those in Model 1. For example, the DW of ‘Pancreatic cancer’ was 0.929 in Model 1 (Group 1), but 0.724 in Model 2 (Group 1). In Model 2 (Group 1), however, most of the DWs were distributed between 0.2 and 0.4, and there was no cause of disease with DWs of more than 0.8 or less than 0.2. For example, the DW of ‘Otitis media’ was 0.169 in Model 1 (Group 1) but 0.256 in Model 2 (Group 1). It was confirmed that the variance of the DWs between causes of disease estimated in Model 2 was smaller than that of Model 1. Therefore, efforts should continue to be made to produce valid disability weights that can increase the discrimination between causes of disease while meeting distribution assumptions. It is necessary to try to have multiple anchor points and to give constant values using data from health-related quality of life.
Assessing the validity of DWs is not an easy task.2224 This is because there is no gold standard for DWs, and we estimate DWs for hundreds of causes of disease at once. Therefore, in this study, various methods were used to evaluate the validity of DWs. We examined whether there was a reversal in DWs of causes of disease with other severity levels and we also checked the distribution of DWs and compared them with previous results. Although not used in this study, it is also possible to compare EQ-5D's DWs with utility weights.1925 Considering these points together, we conclude that ‘Model 2 in Group 1’ has several advantages over others. However, due to the emergence of new diseases, changes in characteristics of the disease, development of new drugs and treatment techniques, and changes in social perspectives on disability, the DWs calculated in the past may not be valid presently, so that it is necessary to evaluate and revise DWs continuously.
One limitation of this study is that the number of participating nurses or oriental medical doctors was relatively small compared to physicians. Although the number of participants does not seem to be small compared to other studies, the participation of more people in the DW survey can help to reasonably estimate the DWs of a variety of causes of disease. Future studies should include a higher number of nurses and oriental medical doctors for examining the possibility of calculating the DW.
In conclusion, we attempted to calculate DWs by surveying various types of medical professionals using the previous analysis methods as well as the revised analysis method. Finally, we estimated DWs for a total of 313 causes of disease for the KNBD study. The DWs from this study can be used to estimate accurate DALY and health life expectancy, such as HALE, in Korea.
 XML Download
XML Download