

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Coronavirus disease 2019 (COVID-19) caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) was first reported in December 2019 in Wuhan, Hubei Province, China.1 This disease has spread rapidly to other regions around the world, including the Western Pacific, Europe, Eastern Mediterranean, Americas, and Southeast Asia. The World Health Organization declared COVID-19 a pandemic on March 12, 2020. By April 19, 2020, approximately 2.28 million cases had been diagnosed with 155,124 deaths worldwide.
Although 81% of COVID-19 cases are mild, 14% are severe, and 5% are critical. The fatality rate is about 50.0% in critical cases.2 A number of factors associated with severe COVID-19 have been identified from China. Older age, male sex, presence of comorbidities, low oxygen saturation, and abnormal lab findings (high lactate dehydrogenase [LDH], high procalcitonin, low CD4 cell count, low albumin level) were shown to be risk factors for severe COVID-19.345678
However, patient- and disease-related factors vary from region to region, and these factors may be associated with the clinical severity of COVID-19. There have been no studies regarding prognostic factors for severe disease in COVID-19 patients in Korea. This study was performed to identify prognostic factors for severe disease in patients with COVID-19 in Daegu, Korea.
Go to : 
METHODS
Study design and participants
This was a retrospective observational study of 110 patients with confirmed COVID-19 at Yeungnam University Medical Center, Daegu, Korea, from February 19, 2020 to April 15, 2020. During the study period, all adult patients (age ≥ 18 years) with COVID-19 who were hospitalized via the emergency room or outpatient department were eligible for inclusion.
Data collection and definitions
Demographic, clinical, laboratory, treatment, and outcome data were collected from the electronic medical records of the participants. Demographic and clinical data included age, sex, comorbidities, symptoms and vital signs on admission, and treatment in the hospital. Laboratory data consisted of complete blood count, blood biochemistry, and infection-related biomarkers. Peripheral oxygen saturation was measured by pulse oximetry immediately on hospitalization of the patient. In-hospital case fatality rate was monitored until the final date of follow-up. The data were collected and analyzed by all authors.
Severe disease was defined as a composite outcome of acute respiratory distress syndrome (ARDS), intensive care unit care, or death. ARDS was diagnosed according to the Berlin definition.9 SARS-CoV-2 infection was confirmed by real-time reverse transcription polymerase chain reaction assay of nose and/or throat swap samples.
Statistical analysis
Continuous variables are expressed as means ± standard deviation and were compared by Student's t-test or the Mann-Whitney U test. Categorical variables are described as number (%) and were compared by the χ2 test or Fisher's exact test. Univariable logistic regression analysis was performed to identify prognostic factors of severe COVID-19. Multivariable logistic regression analysis was conducted with variables that showed P < 0.05 in univariable analysis. We excluded variables from the univariable analysis if the number of events was too small for calculation and if there was no marked difference between two groups. In all analyses, two-tailed P < 0.05 was taken to indicate statistical significance. All statistical analyses were performed using SPSS software (ver. 24.0; SPSS Inc., Chicago, IL, USA).
Ethics statement
This study was conducted in accordance with the tenets of the Declaration of Helsinki and was reviewed and approved by the Institutional Review Board (IRB) of Yeungnam University Hospital (YUH IRB 2020-03-057). The requirement for informed consent was waived because of the retrospective study design. The final follow-up date was April 15, 2020.
Go to :
RESULTS
Demographic and clinical characteristics
After excluding seven patients who were transferred to other hospitals, 110 hospitalized patients with confirmed COVID-19 were included in this study (Fig. 1). Baseline characteristics of all patients are summarized in Table 1. The mean age was 56.9 ± 17.0 and 62 patients (56.4%) were women. Forty-nine patients (44.5%) had comorbidities, of which hypertension was the most common (33.6%) followed by diabetes mellitus (26.4%). The most frequently presenting symptoms were fever (56.4%) and cough (52.7%).
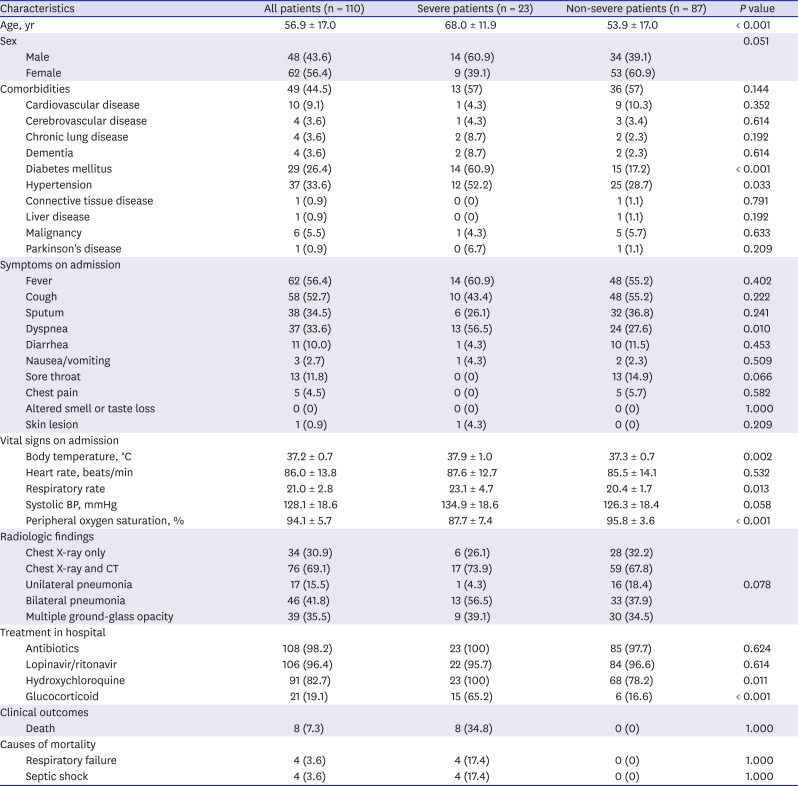
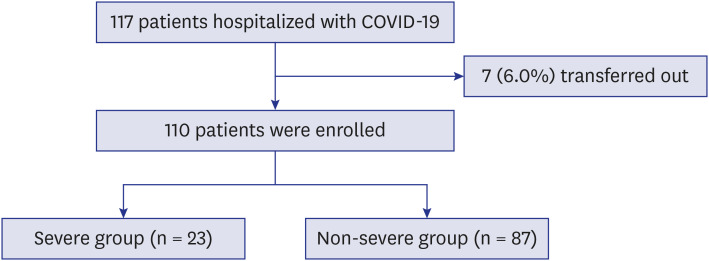
Table 1
Baseline characteristics of the study participants with COVID-19
Data are presented as the mean ± standard deviation or number (%).
COVID-19 = coronavirus disease 2019, BP = blood pressure, CT = computed tomography.
![]()
The patients in the severe group were significantly older than the patients in the non-severe group (68.0 ± 11.9 vs. 53.9 ± 17.0, respectively, P < 0.001). The severe group was significantly more likely to have diabetes mellitus (60.9% vs. 17.2%, respectively, P = 0.001) and hypertension (52.2% vs. 28.7%, respectively, P = 0.033). On admission, body temperature (37.9°C ± 1.0°C vs. 37.3°C ± 0.7°C, respectively, P = 0.002) and respiration rate (23.1 ± 4.7 vs. 20.4 ± 1.7 breaths per minute, respectively, P = 0.013) were significantly higher in the severe group than the non-severe group. Peripheral oxygen saturation was significantly lower in the severe group than the non-severe group (87.7 ± 7.4 vs. 95.8 ± 3.6, respectively, P < 0.001). It was difficult to detect meaningful differences in radiologic findings between patients in the severe group and those who were not.
Laboratory findings
Laboratory findings on hospital admission are summarized in Table 2. In complete blood counts, white blood cell count (8.2 ± 3.4 vs. 6.3 ± 3.2, respectively, P = 0.017) and neutrophil count (7.1 ± 3.4 vs. 4.1 ± 3.0, respectively, P < 0.001) were higher in the severe group than the non-severe group. Lymphocyte count (0.7 ± 0.3 vs. 1.6 ± 0.7, respectively, P < 0.001) and platelet count (184.7 ± 75.3 vs. 259.8 ± 104.6, respectively, P = 0.002) were significantly lower in the severe group than the non-severe group. With regard to blood chemistry, albumin level was significantly lower in the severe group than the non-severe group (3.1 ± 0.4 vs. 3.9 ± 0.5 g/dL, respectively, P < 0.001). Concentrations of aspartate aminotransferase, total bilirubin, blood urea nitrogen, LDH, and creatine kinase-MB (CK-MB) were significantly higher in the severe group than the non-severe group. With regard to infection-related markers, C-reactive protein level was significantly higher in the severe group than the non-severe group (15.5 ± 8.8 vs. 3.3 ± 6.2 mg/L, respectively, P < 0.001), although procalcitonin level was not significantly different between the two groups (2.2 ± 5.6 vs. 0.1 ± 0.1 ng/mL, respectively, P = 0.094). Three cases of bacterial co-infection (2 cases of Klebsiella pneumonia, 1 case of Clostridium difficile) were identified in the non-severe group. Duration of viral shedding was not different between the two groups.
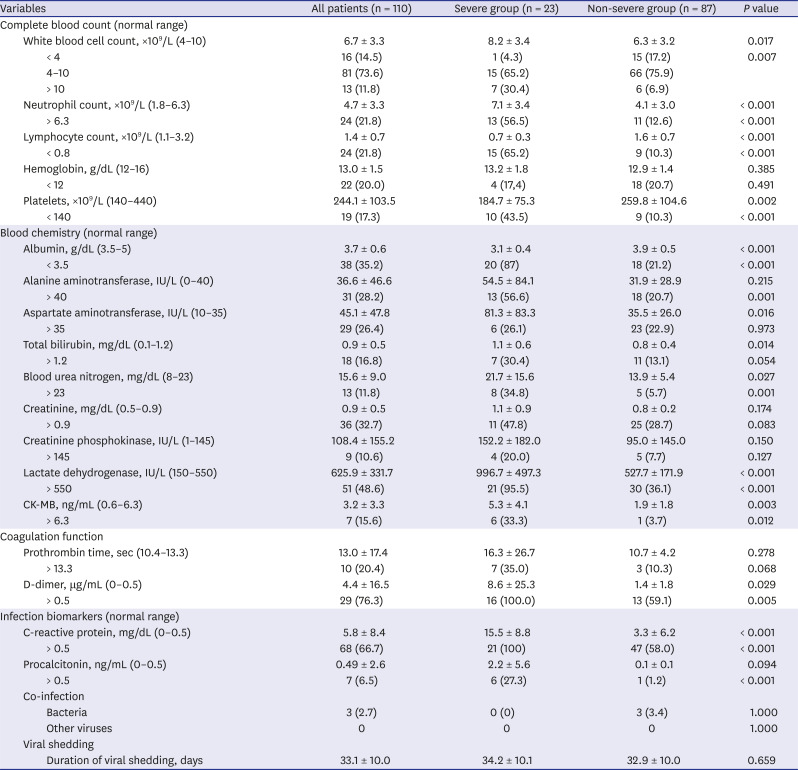
Table 2
Laboratory findings on admission in patients with COVID-19
Data are presented as the mean ± standard deviation or number (%).
COVID-19 = coronavirus disease 2019, CK-MB = creatine-kinase MB.
![]()
Prognostic factors for severe COVID-19
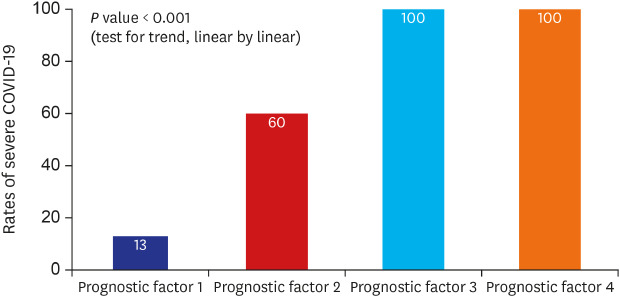
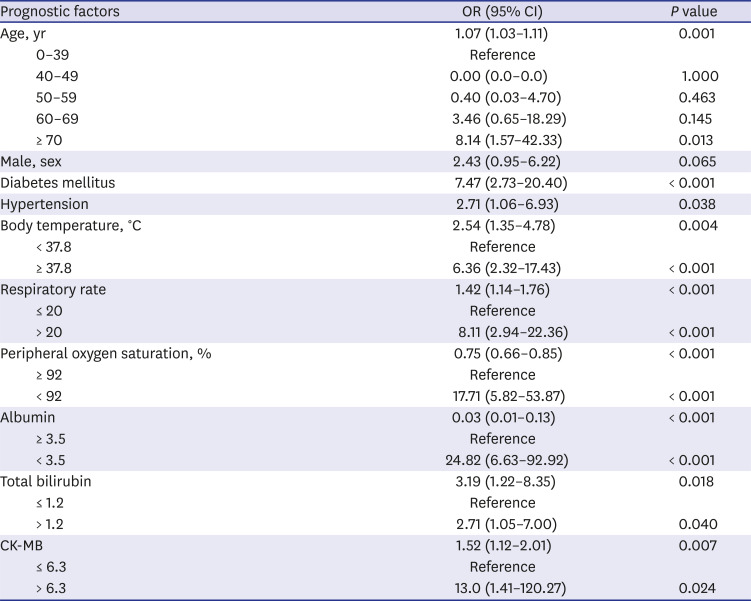
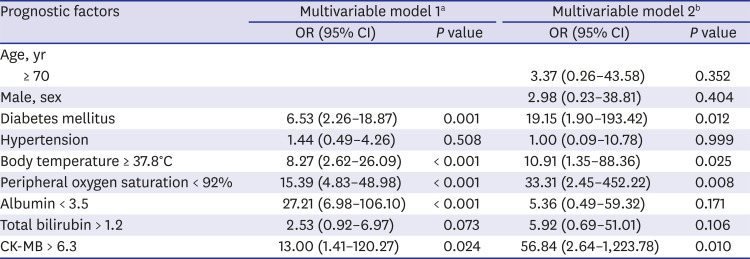
Multivariable analysis using variables with P < 0.05 in univariable analysis (Table 3) and the final logistic regression model demonstrated that diabetes mellitus (odds ratio [OR], 19.15; 95% confidence interval [CI], 1.90–193.42; P = 0.012), body temperature ≥ 37.8°C (OR, 10.91; 95% CI, 1.35–88.36; P = 0.025), peripheral oxygen saturation < 92% (OR, 33.31; 95% CI, 2.45–452.22; P = 0.008), and CK-MB > 6.3 (OR, 56.84; 95% CI, 2.64–1,223.78; P = 0.010) on admission were associated with greater risk of severe COVID-19 (Table 4). The rates of severe disease increased for patients with diabetes mellitus, body temperature ≥ 37.8°C, peripheral oxygen saturation ≤ 92%, and CK-MB > 6.3 (Fig. 2). The likelihood of development of severe COVID-19 increased with increasing number of prognostic factors (P < 0.001, test for trend) (Fig. 3).
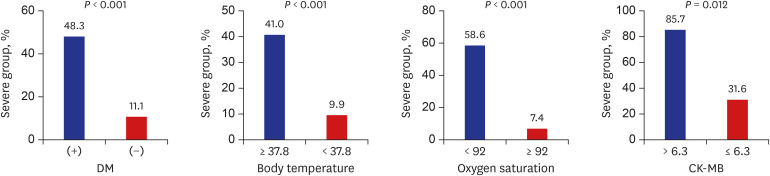 | Fig. 2Comparison of rates of severe COVID-19 using categorical variables.DM = diabetes mellitus, COVID-19 = coronavirus disease 2019, CK-MB = creatine-kinase MB.
|
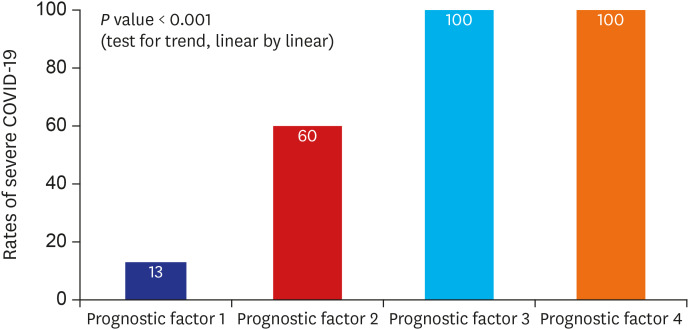 | Fig. 3Rate of patients with severe COVID-19 according to the presence of prognostic factors.COVID-19 = coronavirus disease 2019.
|
Table 3
Univariable analysis of prognostic factors for severe COVID-19
COVID-19 = coronavirus disease 2019, OR = odds ratio, CI = confidence interval, CK-MB = creatine-kinase MB.
![]()
Table 4
Multivariable logistic regression analysis of prognostic factors for severe COVID-19
COVID-19 = coronavirus disease 2019, OR = odds ratio, CI = confidence interval, CK-MB = creatine-kinase MB.
aAdjusted for age, sex; bAdjusted for age, sex, diabetes mellitus, hypertension, body temperature, peripheral oxygen saturation, albumin, total bilirubin, and CK-MB.
![]()
Go to :
DISCUSSION
Among the 110 patients with COVID-19, 23 (20.9%) had severe disease and the in-hospital case fatality rate was 7.3% in this study. We showed that the presence of diabetes mellitus, body temperature ≥ 37.8°C, peripheral oxygen saturation < 92%, and CK-MB > 6.3 were independent predictors of severe disease in hospitalized COVID-19 patients. To our knowledge, this is the first study to evaluate the prognostic factors of severe COVID-19 in Korea.
Diabetes mellitus is a major public health issue, with an estimated global prevalence of 9.3% in 2019.10 A population-based cohort study showed that type 2 diabetes increased the risk of death associated with pneumonia, and hyperglycemia on admission was associated with increased mortality for both diabetic and nondiabetic patients with community-acquired pneumonia.11 Yang et al.12 reported that diabetes and ambient hyperglycemia are independent risk factors for death and morbidity in SARS patients. Diabetes also results in immune dysregulation and more severe and prolonged lung pathology in Middle East respiratory syndrome.13 The main mechanisms underlying the poorer clinical outcomes in cases of infections associated with diabetes mellitus are as follows: 1) decreased T lymphocyte response; 2) decreased neutrophil function; 3) disorders of humoral immunity; and 4) depression of the antioxidant system.14 In a recent study, COVID-19 patients without other comorbidities but with diabetes were shown to be at greater risk of severe disease as assessed by organ damage, inflammatory factors, and hypercoagulability. In addition, COVID-19 patients with diabetes are at high risk for disease progression.15 The results of the present study suggested that the progression of COVID-19 is influenced by diabetes mellitus. Physicians should pay close attention to whether diabetic patients with COVID-19 show rapid clinical deterioration.
Body temperature is one of the variables included in the pneumonia severity index16 and systemic inflammatory response syndrome (SIRS),17 which can predict clinical outcomes in pneumonia. The febrile response is thought to be mediated by endogenous factors, called endogenous pyrogens. Pyrogenic cytokines, such as tumor necrosis factor (TNF), interleukin (IL)-1, IL-6, and interferons (IFNs), are released in response to exogenous stimuli, such as bacterial or viral products and toxins.18 In COVID-19, the levels of the proinflammatory cytokines IL-1β, IL-4, IL-6, IL-10, IFN-γ, and TNF-α are significantly higher in severe cases than in mild cases.19 The results of the present study suggested that critical COVID-19 patients have elevated levels of inflammatory cytokines, which increase body temperature.
Low peripheral oxygen saturation was shown to be an independent prognostic factor for severe COVID-19.8 Many COVID-19 patients experience rapid respiratory failure and hypoxemia without any signs of dyspnea, which is referred to as silent hypoxemia.20 This unique characteristic of COVID-19 makes it difficult to predict clinical deterioration accurately using traditional scores, such as quick sequential organ failure assessment and SIRS. As COVID-19 is a highly contagious infectious disease, medical staff tend to have less contact with patients. Therefore, the discovery of a worsening condition in patients may be delayed. From this viewpoint, peripheral oxygen saturation measured immediately upon hospitalization through pulse oximetry can be used as a convenient and accurate marker for the prediction of clinical deterioration in COVID-19.
Cardiac injury is associated with death, and severity of COVID-19 is associated with acute cardiac injury. In the systemic review of the 28 studies with 4,189 confirmed COVID-19 patients, severe COVID-19 infection was associated with high cardiac injury related markers, such as troponin, CK-MB, and myoglobin. And also cardiac injury in COVID-19 were related with higher mortality (OR, 3.85; 95% CI, 2.13–6.96; P < 0.001).21 It has been known that, the SARS-CoV-2 invades human cells via the receptor angiotensin converting enzyme II (ACE2). ACE2 is expressed in the lung, heart, esophagus, kidney, bladder, and ileum. Thus, organs that express ACE2 are vulnerable to SARS-CoV-2 infection.22 Therefore, the measurement of cardiac damage markers on admission is needed in patients with COVID-19, which predict the prognosis of COVID-19.
There are several Chinese studies demonstrating the risk factors for severity of COVID-19. Li et al.5 reported that elder age, hypertension, high cytokine levels, and high LDH levels were associated with severe COVID-19 inpatients in Wuhan. A study in Anhui, China revealed that low fingertip oxygen saturation, and decreased CD4 cell count were independent risk factors for severe COVID-19 patients.8 Diabetes, and maximum body temperature admission were risk factors for progression of COVID-19.1523 The predictors of severe disease progression on Korean patients and those in Chinese patients were not much different.
This study had several limitations. First, this was a retrospective study conducted in a single center in Korea, which subjected only hospitalized patients. Therefore, these results cannot be generalized to all COVID-19 patients. Second, antiviral agents and corticosteroid usage were not included as variables in this study. Our research focused on the baseline clinical characteristics and laboratory findings related to worsening of the patients' condition due to severe disease and not on treatment. Third, selection bias could not be avoided because population-based data were not used. The disease severity of patients may vary between hospitals in the same region. Fourth, proinflammatory cytokines and early CD8+ T-cell response that can be associated with disease severity, were not measured in this study.
In conclusion, we found that the presence of diabetes mellitus, body temperature ≥ 37.8°C, peripheral oxygen saturation < 92%, and CK-MB > 6.3 are independent predictors of severe disease in hospitalized COVID-19 patients. The likelihood of progression to severe COVID-19 increased with an increasing number of prognostic factors. Appropriate assessment of prognostic factors and close monitoring to provide the necessary interventions at the appropriate time in high-risk patients may reduce the case fatality rate of COVID-19.
Go to :
 XML Download
XML Download