

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Acute kidney injury (AKI) is a common clinical syndrome with significant morbidity and mortality in hospitalized patients.12 It also has been increasingly recognized as the major risk factor for the development and progression of chronic kidney disease (CKD) and a recent United States Renal Data System report showed that acute tubular necrosis (ATN) with no recovery is responsible for 2%–3% of the annual incidence of end stage renal disease (ESRD) cases.3 However, despite this huge clinical impact, long-term outcome of AKI still remains unclear.
In the spectrum of AKI, ATN, caused by ischemia, toxins, or sepsis, is the most common cause of intrinsic AKI and characterized by patchy or diffuse denudation of renal tubular cells with loss of the brush border and intratubular obstruction with sparing of glomeruli.4 However, despite these well characterized pathological features of ATN, it is usually diagnosed clinically without histological confirmation. In contrast, disease affecting the interstitium with infiltration of lymphocytes and eosinophils, termed acute interstitial nephritis (AIN) is usually diagnosed by kidney biopsy and is increasingly recognized as an important cause of AKI.567
While kidney biopsy is a gold standard not only in diagnosis but also in prediction of outcome in various glomerular diseases, it is not usually performed in AKI. Kidney biopsy in AKI is usually indicated in the presence of active urinary sediment with possible diagnosis of diseases affecting glomeruli or vasculature or in cases of uncertain etiologies. The majority of AKI cases are diagnosed in the clinical context. The lack of specific therapeutic option coupled with risk of complications have also been a barrier for kidney biopsy in patients with AKI and thus, the value of histological features in predicting outcome has not been studied thoroughly.
Here in this study, we compared long-term renal outcome of 116 biopsy proven ATN and 137 AIN cases. Rate of progression to ESRD during the mean follow up of 76.5 ± 91.9 months were compared and pathological features that are associated with progression to ESRD were also determined.
Go to : 
METHODS
Participants
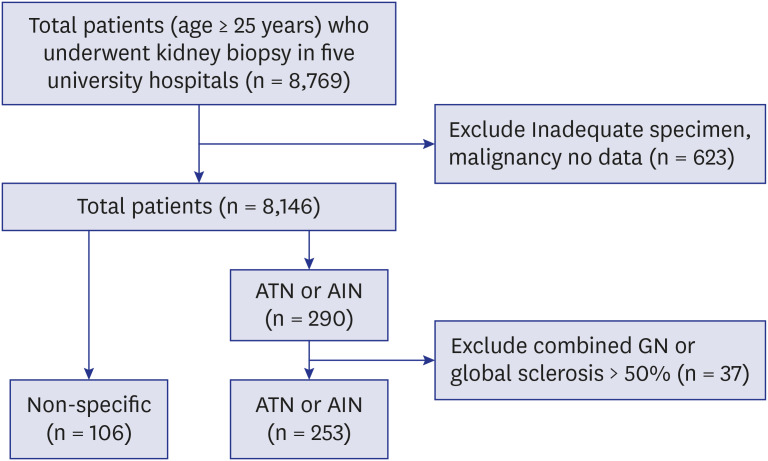
Out of 8,769 native kidney biopsy series that have been obtained from five university hospitals in Korea: Korea University Anam Hospital, Korea University Guro Hospital, Seoul National University Hospital, Seoul National University Bundang Hospital, and Hallym University Kangdong Sacred Heart Hospital from January 1982 and January 2018, we first identified 290 patients who were histologically diagnosed with ATN or AIN in kidney biopsy. Thirty-seven patients with combined glomerulonephritis or global sclerosis of > 50% were excluded and 116 patients with ATN and 137 patients with AIN were finally enrolled (Fig. 1). We also identified 106 patients with no specific abnormality in pathology and used as control. Renal tissue was obtained with ultrasonography-guided percutaneous gun biopsy, and the results were interpreted by a renal pathologist in each hospital. Clinical, biochemical, and medication data were obtained from the electronic medical records using the patient identification number and date of renal biopsy. These data were confirmed by a trained research nurse.
Definitions
The estimated glomerular filtration rate (eGFR) was estimated by using Modification of Diet in Renal Disease Study equation.8 Body mass index was calculated on the basis of weight and height (kg/m2). Proteinuria was defined as protein ≥ 1+ on urine dipstick. Hypertension (HTN) was defined as systolic blood pressure ≥ 140 mmHg, diastolic blood pressure ≥ 90 mmHg, or use of antihypertensive medication. Diabetes mellitus (DM) was defined as fasting blood glucose ≥ 126 mg/dL, use of an oral hypoglycemic agent or insulin, or history of diabetes according to the electronic medical records. Steroid treatment was defined as use of steroids within 30 days before or after kidney biopsy. Cardiovascular disease was defined as angina, myocardial infarction, or stroke. Non-renal recovery was defined as eGFR < 60 mL/min/1.73 m2 at 6 months after biopsy. Data on ESRD and death were collected from the registry of the Korean Society of Nephrology on April 2018 and electronic medical records.9 A progressor was defined as a patient who developed ESRD within the follow-up period.
Renal pathology
Methods of renal pathology evaluation were described previously.10 All biopsies were evaluated using hematoxylin and eosin, periodic acid-Schiff, Masson trichrome, or periodic acid methenamine silver stains for light microscopy; immunofluorescence staining using antibodies against IgA, IgG, IgM, C3, C1q, and kappa and lambda light chains; and electron microscopy. We assessed the presence of tubular necrosis, tubular edema, interstitial inflammation, tubulitis as well as tubular atrophy, interstitial fibrosis and vascular lesion. Vascular lesions represent either arteriolar fibro-intimal thickening or hyalinosis.
Statistical analysis
All analyses were performed using SPSS software (SPSS version 25.0, Chicago, IL, USA). Data were presented as mean ± standard deviations for continuous variables and as percentages for categorical variables. Differences were analyzed using a χ2 test for categorical variables and analysis of variance for continuous variables. The Kaplan-Meier method was used for the survival curve, and statistical significance was calculated using the log-rank test. For multivariate logistic regression analysis and Cox proportional hazards analysis, variables were chosen using P < 0.05 in univariate analysis, along with age and sex. A P value of < 0.05 was considered significant.
Ethics statement
This study was approved by the Institutional Review Board (IRB) of Korea University Anam Hospital (IRB approval No. 2018AN0063), Korea University Guro Hospital (IRB approval No. 2017GR0082), Seoul National University Hospital (IRB approval No. 1802-102-924), Seoul National University Bundang Hospital (IRB approval No. B-1707/408-106), and Kangdong Sacred Heart Hospital (IRB approval No. KANGDONG 2016-06-008). IRB approved that informed consent was not necessary because this was a retrospective study.
Go to :
RESULTS
Baseline patient characteristics
Among 8,769 kidney biopsy series, ATN and AIN were found to be 1.6% and 1.9% respectively. The baseline characteristics of the study patients were collected at the time of kidney biopsy (Table 1). Patients with AIN were significantly older than those with control and ATN (P < 0.001). Compared to control group, prevalence of DM, HTN was higher in both ATN/AIN group. ATN/AIN group showed significantly lower eGFR, suggesting the state of AKI and also lower serum albumin, cholesterol and hemoglobin level. The prevalence of 1+ or more dipstick proteinuria was highest in the AIN group (P = 0.003) and the use of steroid was significantly higher in patients with AIN (P < 0.001).
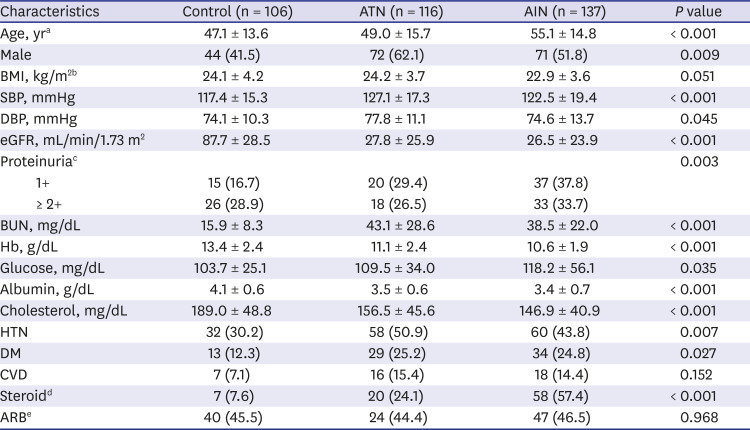
Table 1
Baseline characteristics of patients
Data are presented as mean ± standard deviation or number (%).
ATN = acute tubular necrosis, AIN = acute interstitial nephritis, BMI = body mass index, SBP = systolic blood pressure, DBP = diastolic blood pressure, eGFR = estimated glomerular filtration rate, BUN = blood urea nitrogen, Hb = hemoglobin, HTN = hypertension, DM = diabetes mellitus, CVD = cardiovascular disease, ARB = angiotensin II receptor blocker.
a
P < 0.05, ATN vs. AIN; bBMI was measured in 260 patients; cUrine analysis was measured in 256 patients; dThe use of steroid was analyzed in 276 patients; eThe use of ARB was analyzed in 243 patients.
![]()
Pathologic findings in ATN and AIN
Although ATN and AIN are distinct pathological entities with characteristic tubular necrosis and interstitial inflammation, there were significant overlap in several components of pathological characteristics. Tubular necrosis (88.0% vs. 65.2%) and interstitial edema (57.4 vs. 37.1%) were more common in the ATN (P < 0.01), while interstitial inflammation (79.6 vs. 99.2), tubulitis (6.5 vs. 51.5), interstitial fibrosis (38.9 vs. 64.9) and vascular lesion (31.8 vs. 49.2) were more common in AIN (P < 0.01). The percentages of global glomerulosclerosis or tubular atrophy were not significantly different between the groups (Table 2).
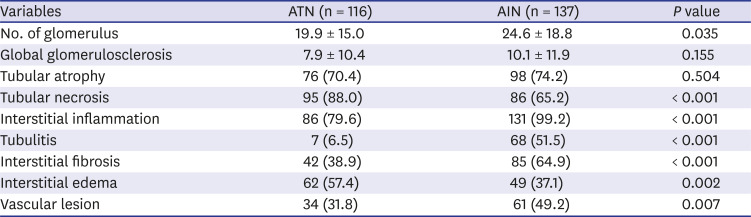
Table 2
Pathologic findings in patients with acute tubular necrosis or interstitial nephritis
Data are presented as mean ± standard deviation or number (%).
ATN = acute tubular necrosis, AIN = acute interstitial nephritis.
![]()
Renal recovery in patients with ATN and AIN
Although eGFR at the time of biopsy was not different, rate of non-recovery of renal function defined as eGFR > 60 mL/min/1.73 m2 at 6 months after biopsy was significantly higher in AIN (69.4 vs. 49.3%, P = 0.007) (Fig. 2). Compared with the ATN, the AIN group showed a 2.21-fold higher risk of non-recovery of renal function (95% confidence interval [CI], 1.17–4.18) after adjusting for age and sex and this association persisted even after adjusting multiple factors including baseline comorbidities (relative risk [RR], 2.80; 95% CI, 1.20–6.47 compared to ATN group) (Table 3).

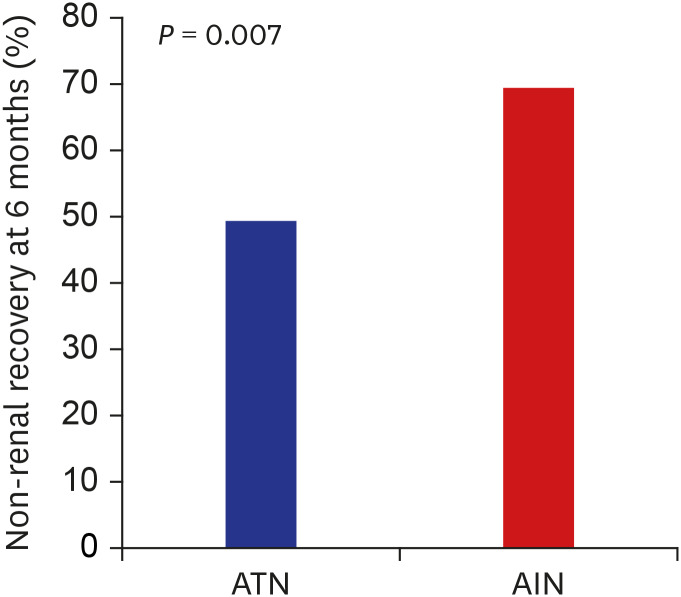 | Fig. 2Incidence of non-renal recovery at 6 months.The incidence of non-renal recovery was lower in the ATN group than in the AIN group, at 49.3% and 69.4%, respectively, (P = 0.007). Non-renal recovery was defined as estimated glomerular filtration rate < 60 mL/min/1.73 m2 at 6 months.
ATN = acute tubular necrosis, AIN = acute interstitial nephritis.
|
Table 3
Risks for the non- recovery of renal function at 6 months in AIN compared with ATN
| Variables | Model 1 | Model 2 | Model 3 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| RR | 95% CI | P value | RR | 95% CI | P value | RR | 95% CI | P value | |
| ATN | Reference | Reference | Reference | ||||||
| AIN | 2.34 | 1.26–4.34 | 0.007 | 2.21 | 1.17–4.18 | 0.014 | 2.79 | 1.20–6.47 | 0.017 |
Data are presented as mean ± standard deviation or number (%).
ATN = acute tubular necrosis, AIN = acute interstitial nephritis, RR = relative risk, CI = confidence interval.
Model 1, unadjusted; Model 2, adjusted by age, sex; Model 3, adjusted by age, sex, body weight, systolic blood pressure, estimated glomerular filtration rate, hemoglobin, glucose, cholesterol, history of diabetes, hypertension, and cardiovascular disease.
![]()
Progression to ESRD in patients with ATN and AIN
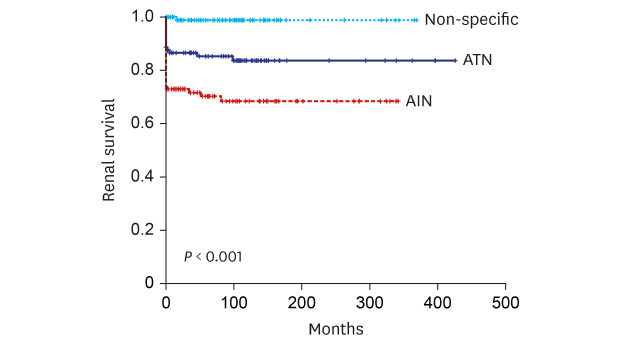
During a mean follow up of 76.5 ± 91.9 months, 82 (22.9%) patients progressed to ESRD. ESRD developed in 2.8%, 21.5%, and 39.4% of patients with control, ATN, and AIN respectively (P < 0.001). Kaplan-Meier curves showed that the AIN group had the worst renal survival followed by ATN and control (P < 0.001) (Fig. 3).
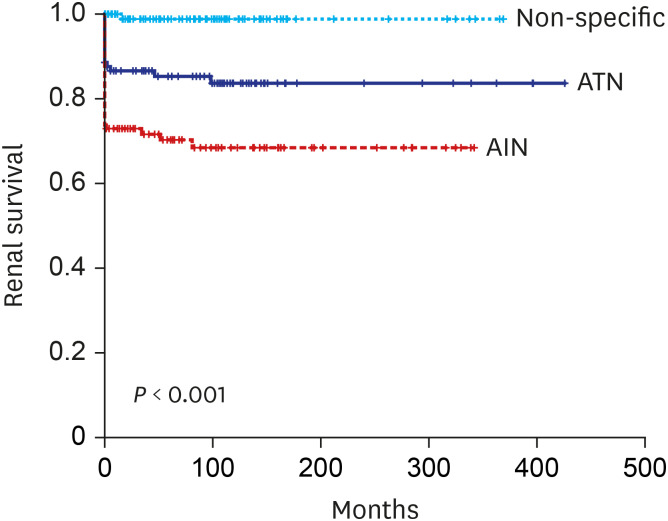
After adjusting patients’ demographic factors and comorbidities, biopsy proven ATN showed a 12.14-fold increased risk of developing ESRD compared with the control group (95% CI, 1.19–24.24). The RR of ESRD in biopsy proven AIN was 23.05 compared with the control group (95% CI, 2.42–219.53) (Table 4).

Table 4
Risks of development of end stage renal disease according to the pathologic diagnosis in all patients
| Variables | Model 1 | Model 2 | ||||
|---|---|---|---|---|---|---|
| RR | 95% CI | P value | RR | 95% CI | P value | |
| Control | Reference | Reference | ||||
| ATN | 16.39 | 2.17–124.04 | 0.007 | 12.14 | 1.19–24.24 | 0.035 |
| AIN | 29.58 | 4.03–217.19 | 0.001 | 23.05 | 2.42–219.53 | 0.006 |
RR = relative risk, CI = confidence interval, ATN = acute tubular necrosis, AIN = acute interstitial nephritis.
Model 1, adjusted by age and sex; Model 2, adjusted by age, sex, estimated glomerular filtration rate, history of diabetes, hypertension, cardiovascular disease, and use of steroid.
![]()
Eighteen (5.0%) died during the median follow up of 67.3 (31.0–140.1) months. Mortality was significantly high in both ATN (8.6%) and AIN (5.1%) compared to control group (0.9%) (P = 0.032) (data not shown).
Factors associated with progression ESRD in ATN and AIN
We compared clinical and pathological features that are associated with progression to ESRD in patients with ATN or AIN. Progressors were significantly older (P = 0.001) and more likely to be women (P = 0.036) and treated by steroid (P < 0.001). The nadir eGFR and also 6 months eGFR were significantly lower (P < 0.001) and percentage of patients with dipstick proteinuria ≥ 2+ were higher in progressors (P = 0.002).
Among the pathological findings, the presence of interstitial inflammation (87.9% vs. 96%, non-progressor vs. progressor, P = 0.048), tubulitis (26.7% vs. 41.3%, progressor vs. progressor, P = 0.023), vascular lesion (36.9% vs. 50.7%, non-progressor vs. progressor, P = 0.049) and interstitial fibrosis (47.0% vs. 66.7%, non-progressor vs. progressor, P = 0.005) were significantly associated with progression, while tubular necrosis or interstitial edema, tubular atrophy were not. The presence of interstitial edema and tubular necrosis was higher in non-progressor (Table 5).
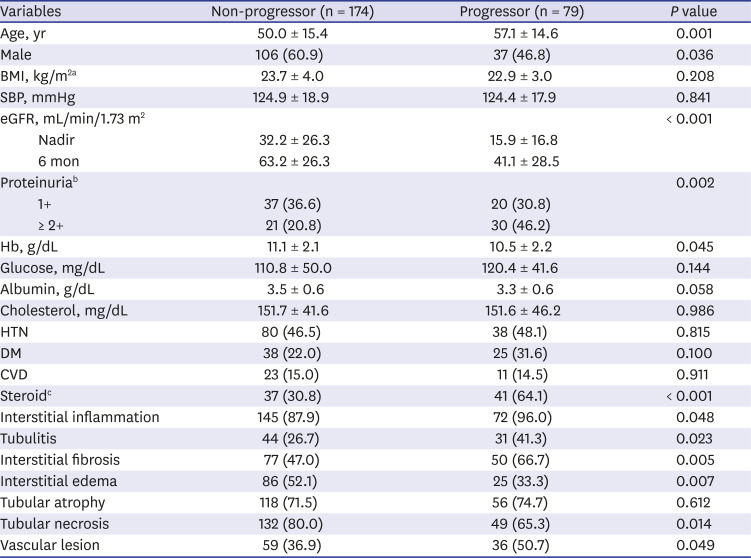
Table 5
Factors associated with progression to end stage renal disease in biopsy proven ATN and AIN
Data are presented as mean ± standard deviation or number (%).
ATN = acute tubular necrosis, AIN = acute interstitial nephritis, BMI = body mass index, SBP = systolic blood pressure, eGFR = estimated glomerular filtration rate, Hb = hemoglobin, HTN = hypertension, DM = diabetes mellitus, CVD = cardiovascular disease.
aBMI was measured in 170 patients; bUrine analysis was measured in 166 patients; cThe use of steroid was analyzed in 183 patients.
![]()
Go to :
DISCUSSION
In this study, we demonstrated the followings; 1) substantial proportion of patients with biopsy proven ATN (21.5%) and AIN (39.4%) progressed to ESRD in long-term follow up, 2) AIN showed worse renal outcome compared to ATN, 3) older age, female sex and low nadir eGFR, 6 months eGFR were associated with ESRD progression, and 4) pathological features including interstitial inflammation, tubulitis, interstititial fibrosis and vascular lesion were also associated with progression to ESRD regardless of causes.
Although epidemiological studies have shown AKI increases the risk of CKD and/or ESRD, long-term renal outcome of AKI still remains unclear and lack of biopsy based studies in AKI might contribute to this uncertainty. ATN from ischemia, toxins or infection is the most common type of AKI and recently, AIN has become increasingly recognized as an important cause of AKI. However, the reported incidence of AIN was only 1%–4.7% in all kidney biopsy series6 and 10%–27% in biopsies performed in patients with AKI.11 Percentage of AIN of total 8,769 biopsies in our study (1.9%) was also comparable with previous report. The renal outcomes of AIN have been reported to be poor. In a single-center study of 133 patients with biopsy-proven AIN, 38% of patients achieved partial recovery while 14% showed no recovery at 6 months.12 Another study of 157 patients with AIN also showed that 52.2% of patients developed CKD by 12 months and ESRD developed in 9.4% of steroid-treated patients and in 34.4% of non-treated patients during a median follow-up of 20 months.713 In line with these studies, our study also demonstrated poor renal outcome; 69.4% of patients did not recover their renal function defined as eGFR > 60 mL/min/1.73 m2 at 6 months and more importantly, we demonstrated that 39.4% of patients ultimately progressed to ESRD in a follow up period of 76.5 ± 91.9 months regardless of steroid treatment. Although specific etiologies of AIN are not separately analyzed in this study, we could clearly demonstrate worse renal outcome in patients with AIN in very long term follow up. RR of developing ESRD in AIN patients were 23-fold higher compared to control group. Significantly older age, more frequently combined interstitial fibrosis or vascular lesion, that are indices of chronicity, in AIN could be one factor facilitating the progressive CKD/ESRD. In contrast to AIN that the kidney biopsy is prerequisite for diagnosis, biopsy studies of ATN have been far more limited.1415 The vast majority of ATN is diagnosed in the clinical context with a help of traditional urinary indices with reasonable degree of accuracy. ATN has been considered to have a relatively good prognosis in terms of functional recovery. However, according to a study by Abdulkader et al.16 renal outcome of biopsy proven ATN also seems to poor. They demonstrated that 11 of 18 biopsy proven ATN patients showed only partial recovery of renal function and higher peak creatinine, longer hospital stay and tubulointerstitial lesion that was a sum of tubular necrosis, tubular atrophy, interstitial fibrosis and interstitial infiltrate were predictors of partial recovery. However the number of patients and follow up period were only 18 patients with 6 months, making a firm conclusion impossible.17 Recently, a 6.64-fold increased risk of developing stage 4 CKD was observed in US veterans of more than 110,000 with ATN.16 The annual incidence of ESRD attributed to ATN was estimated to be 3.5% in 2009–2010.3 However, that study has possibility to have included patients with other causes of AKI, because the definition of ATN used in the study was based on laboratory findings and diagnostic code of acute renal failure or ATN only. In contrast, our study analyzed a relative large number of biopsy proven ATN patients (n = 116) with long term follow up to ESRD. In spite of lower rate of non-recovery or progression to ESRD compared to AIN, patients with biopsy proven ATN still showed poor renal outcome; 49.3% did not achieve renal functional recovery defined as eGFR > 60 mL/min/1.73 m2 at 6 months and more importantly, 21.7% progressed to ESRD during 76.5 ± 91.9 months that is significantly higher compared to control group. To the best of our knowledge, this is the largest study of long-term renal outcome of histologically confirmed native kidney ATN. Although specific indication or timing of biopsy are not clearly recorded, these data could give an important message that ATN from diverse etiologies might be contributing to increasing incidence of ESRD worldwide. Even after adjusting multiple patient factors, RR of progressing to ESRD was 12.136-fold higher in biopsy proven ATN patients compared to control group. However, given that the majority of patients with AKI are diagnosed and treated without biopsy, we still cannot answer to questions that who and what percentage of patients progress to CKD/ESRD.
Kidney biopsy is an important tool in diagnosis and outcome prediction in glomerular diseases. Degree of interstitial fibrosis or number of crescents are well known histologic features in predicting outcome or treatment response. ATN and AIN are distinct pathological entities with predominant tubular necrosis and interstitial inflammation. However, pathological features including tubular necrosis, interstitial inflammation, edema, tubulitis and even chronicity indices such as tubular atrophy, interstitial fibrosis or vascular lesion are substantially overlapped in both entities. We assessed the value of these histological features in predicting renal outcome in both AIN and ATN. The presence of interstitial inflammation, tubulitis, interstitial fibrosis and vascular lesion in both ATN or AIN were significantly associated with progression to ESRD while tubular necrosis, interstitial edema or tubular atrophy were not. Although all these pathological features were not found to be an independent factor that can predict ESRD, the value of these pathological features in ATN or AIN as outcome predictors should be further assessed in larger series of native kidney biopsy studies. Given that insight regarding the role of kidney biopsy in AKI is expanding, it is possible that combining these pathological features with patient clinical and laboratory findings might improve the accuracy of outcome prediction. In addition, kidney biopsy in AKI may offer opportunities of finding newer insight into heterogenous pathogenesis, molecular mechanisms and newer therapeutic targets of human AKI.
Despite several meaningful findings, our study also has limitations First, kidney biopsies were not reviewed by same renal pathologist. Second, the indication and timing of biopsy might have differed among clinicians and third, the etiologies of ATN or AIN were not determined. Finally, we included relatively severe AKI and this result could not be generalized to the patients with mild degree of ATN or AIN.
However, to our knowledge, this is the first study to show very long-term renal outcome of biopsy proven ATN and AIN and also suggest the possible usefulness of pathological findings in predicting outcome.
In conclusion, our study demonstrated patients with biopsy proven AIN or ATN are at high risk of developing ESRD compared to control patients. Pathological features of interstitial inflammation, tubulitis, interstitial fibrosis or vascular lesion might be important in progression.
Go to :
 XML Download
XML Download