

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
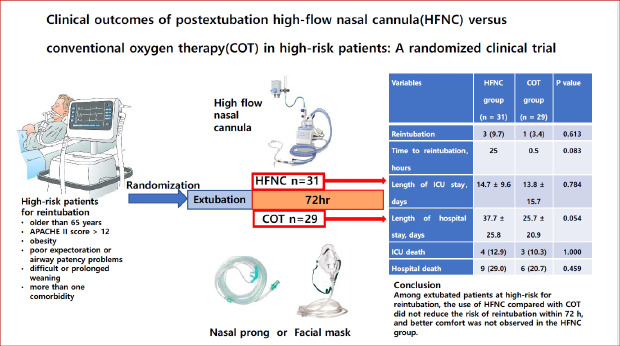
High-flow nasal cannula (HFNC) oxygen therapy supplies heated and humidified oxygen via a nasal cannula device; high flow rates generate low-level positive pressure when the mouth is closed, resulting in a decrease in carbon dioxide level within the anatomic dead space. As a result, HFNC is believed to improve patient comfort, enhance the expectoration of secretions, and decrease the work of breathing. Moreover, HFNC can supply highly concentrated oxygen (up to 100%), which is not possible for conventional oxygen delivery systems. Previous studies have reported physiological and clinical benefits associated with HFNC in respiratory care.12345
Liberation and extubation are important elements in care of patients supported by mechanical ventilation. The success rate of extubation is related to the duration of stay within an intensive care unit (ICU) and mortality rates associated with the underlying condition.67 Following planned extubation, selection of oxygen delivery modality is at the discretion of the attending physician. While previous studies have shown a positive effect of HFNC in postextubation patients,8910 a recent meta-analysis that included a heterogeneous patient group,11 and a previous meta-analysis of studies on patients requiring cardiac surgery demonstrate that HFNC did not reduce reintubation rates or ICU stay duration.12
In Korea, more than half of adult patients treated within an ICU are older adults (aged > 65 years). Concurrently, respiratory insufficiency is one of the most common reasons for ICU admission.13 The present study compared clinical outcomes associated with HFNC and COT among patients at high risk for reintubation.
METHODS
Study design and patients
A single-center randomized clinical trial was conducted at the ICU of the Chungbuk National University Hospital between March 2018 and June 2019. All adult patients requiring mechanical ventilation via an endotracheal tube at a medical ICU for more than 12 hours were eligible for inclusion. Patients suitable for extubation, as confirmed by two intensivists based on the spontaneous breathing test (SBT) result were screened for eligibility. Factors indicative of high risk of reintubation were:
- Acute Physiology and Chronic Health Evaluation II (APACHE II) score > 12 points on extubation day14
- Obesity (defined as body mass index > 3016)
- Poor expectoration or airway patency problem (patients with poor expectoration had a weak cough reflex or previous history of poor expectoration or altered consciousness without sedation before extubation, confirmed by observed frequency [> 3 times during 24 hours] of tracheal suctioning after extubation)17
- Difficult or prolonged weaning17
- Multiple comorbidities (for example, heart failure or moderate to severe chronic obstructive pulmonary disease1415).
Patients had to have at least one of these risk factors to be included in the present study. Patients (or family members, as required) who declined participation in this study were excluded.
Liberation protocol
Clinical liberation from the ventilator followed the ICU protocol of the Chungbuk National University Hospital, which required that patients meet the following criteria: recovery from a primary illness; inspiratory pressure ≤ 12 cmH2O; SpO2 ≥ 92% at a fraction of inspired oxygen (FiO2) < 50% or a positive end-expiratory pressure of 4–6 cmH2O; pH > 7.3 in arterial blood gas analysis (ABGA); respiratory rate (RR) < 30/min; presence of triggering activity > 5 times/min; no use of a neuromuscular blocking agent; systolic blood pressure ≥ 90 mmHg, allowing low-dose inotropes administration (norepinephrine ≤ 0.08 mcg/kg/min, dopamine ≤ 5 mcg/kg/min, and dobutamine ≤ 10 mcg/kg/min).
Patients who met these criteria were subsequently tested for a shallow breath index < 105 breath/min/L. Patients who passed this test took the SBT. Patients underwent SBT with a t-piece for 30 to 120 minutes, and when the patient showed respiratory distress, we returned the patient to ventilator support during the next 24 hours. If the extubation criteria were fulfilled (alert mental status, capable of coughing or rotating the neck, SpO2 ≥ 92%, RR < 30/min, and no respiratory distress), we attempted extubation.
Randomization and data collection
Before planned extubation, we performed stratified randomization according to age and gender, assigning patients to HFNC oxygen therapy and COT. Baseline characteristics of the enrolled patients were recorded, including age, gender, height, body weight, primary disease that required ICU admission, underlying diseases, the date of ICU admission, intubation, extubation, and reintubation, APACHE II score on the day of extubation, vital signs (blood pressure and RR), FiO2, and the results of ABGA 30 minutes before and after extubation, and 24 hours after extubation. Data on the duration of ICU and hospital stay, and mortality rate were collected.
Intervention
HFNC oxygen therapy (AIRVO; Fisher & Paykel Healthcare, Auckland, New Zealand) was applied immediately after extubation in the HFNC group. The supplied FiO2 was maintained alongside the previous setting of the mechanical ventilator and adjusted to the patient's peripheral capillary oxygen saturation (SpO2) that was greater than 90%. The set range of flow was 30–60 L/min, adjusted based on the patient's RR. The HFNC was maintained for over 72 hours; a switch to COT was allowed after 72 hours.
COT included use of the nasal prong, and a non-rebreather facemask was applied in this group. Oxygen flow was adjusted to the target SpO2 greater than 90%. The crossover to HFNC was not allowed. Both the HFNC and COT groups were treated by the same nursing and medical staff and had similar medical management in the ICU.
Outcomes
The primary outcome of interest in this study was reintubation within 72 hours. Secondary outcomes included duration of ICU and hospital stay, mortality rate, and time to reintubation. Reintubation was performed in the following clinical situations: 1) refractory hypoxemia or hypercapnia, 2) excessive respiratory secretions, 3) signs of respiratory muscle fatigue, 4) altered mental status, and 5) other situations, where reintubation was deemed necessary by the attending physician.
Statistical analysis
All statistical analyses were performed using SPSS for Windows (version 25.0; SPSS Inc., Chicago, IL, USA). Continuous variables were presented as the mean and standard deviation or median and interquartile range, whereas discrete variables were presented as frequency or percentage. The Mann–Whitney U test was used for between-group comparison of continuous variables, and Fisher's exact test was used for between-group comparison of categorical variables. The impact of interventions on outcomes of interest was compared between groups using a paired t-test. All significance testing was two-tailed, and P values < 0.05 were considered statistically significant.
Ethics statement
The present study protocol was reviewed and approved by the Institutional Review Board of Chungbuk National University Hospital (approval No. 2017-08-003). The trial was undertaken in accordance with the Declaration of Helsinki. Written informed consent was submitted by all participants at the time of enrollment.
RESULTS
From March 2018 to May 2019, we screened 67 patients with at least one risk factor for reintubation; a total of 60 patients were included in the final sample (31 and 29 patients in the HFNC and COT group, respectively) (Fig. 1). Differences in baseline characteristics of the groups are detailed in Table 1. The APACHE II scores (at the time of extubation) of the HFNC group were higher than the scores of the COT group (13.3 ± 4.2 vs. 10.7 ± 3.1; P = 0.010). Frequency of high-risk factors for reintubation did not differ between two groups. Pulmonary infection was the most common reason for ICU admission and was significantly more prevalent in the HFNC than in the COT group (80.6% vs. 51.7%; P = 0.018).
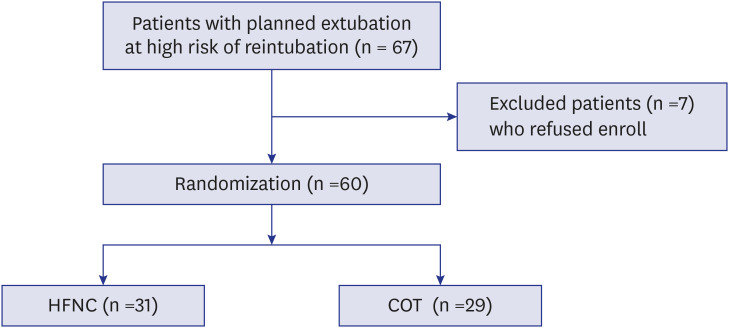
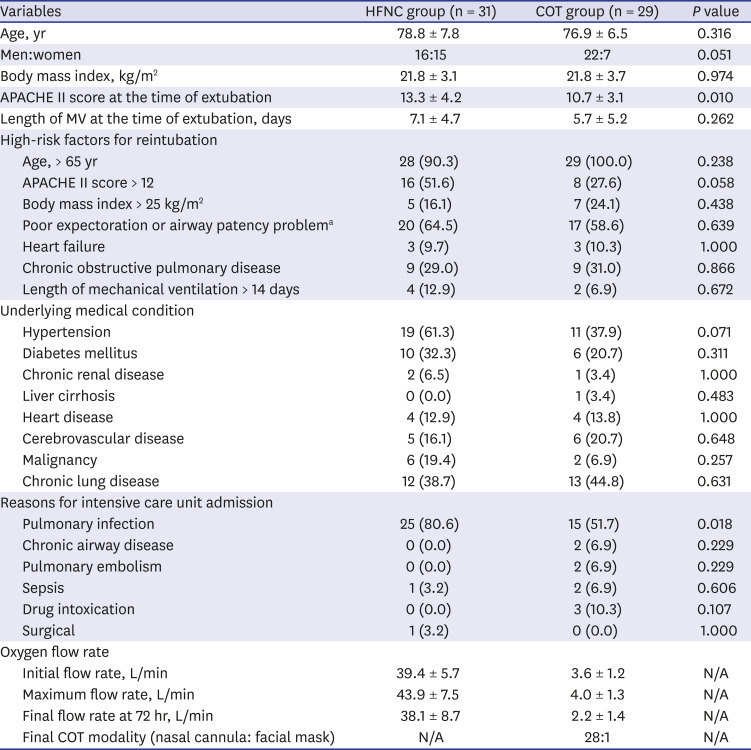
Fig. 1
Flow diagram presenting the number of patients included and excluded from the study, with reasons.
HFNC = high-flow nasal cannula, COT = conventional oxygen therapy.
![]()
Table 1
Baseline clinical and demographic characteristics of enrolled patients
Data are presented as number (%) or mean ± standard deviation.
HFNC = high-flow nasal cannula, COT = conventional oxygen therapy, APACHE II = Acute Physiology and Chronic Health Evaluation II, MV = mechanical ventilation, N/A = not applicable.
aAt least three instances of sputum suction were required within 24 hours after extubation.
![]()
Reintubation was performed in 3 patients (9.7%) in the HFNC group, and 1 patient (3.4%) in the COT group (P = 0.613) (Table 2). The median time from extubation to reintubation was 25 hours (HFNC) and 0.5 hour (COT). The length of ICU or hospital stay, and mortality rate (ICU and hospital) did not differ between the groups. We compared vital signs and ABGA data measured at the time of extubation, 30 minutes and 24 hours after extubation (Supplementary Table 1, Figs. 2 and 3). Heart rate measured after 24 hours of extubation in the HFNC group was significantly higher than that in the COT group (99.8 ± 26.3 vs. 85.0 ± 17.1, P = 0.012).
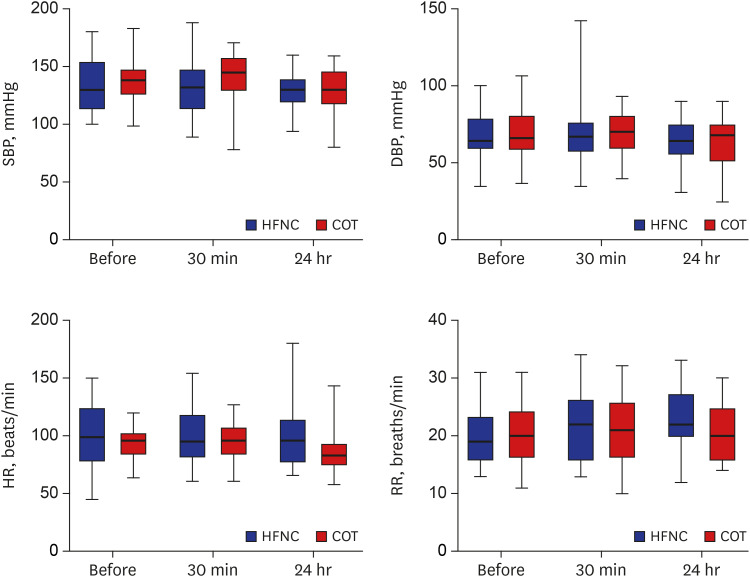

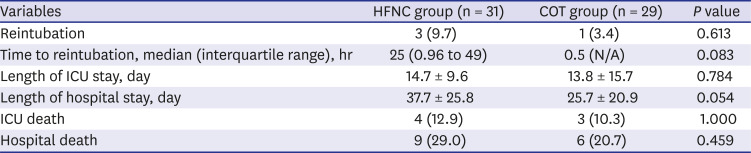
Fig. 2
Changes to vital signs at the time of extubation, 30 minutes and 24 hours after extubation.
HFNC = high-flow nasal cannula, COT = conventional oxygen therapy, sBP = systolic blood pressure, dBP = diastolic blood pressure, HR = heart rate, RR = respiratory rate.
![]()
Fig. 3
Changes in arterial blood gas analysis at the time of extubation, 30 minutes and 24 hours after extubation.
HFNC = high-flow nasal cannula, COT = conventional oxygen therapy, PF ratio = PaO2/FiO2 ratio, pH = arterial blood pH, pCO2, = arterial blood pCO2.
![]()
Table 2
Primary and secondary outcomes
Data are presented as number (%) or mean ± standard deviation.
HFNC = high-flow nasal cannula, COT = conventional oxygen therapy, ICU = intensive care unit.
![]()
The characteristics and outcomes of four reintubated patients are detailed in Table 3. Three of four patients were initially admitted to the ICU due to pneumonia. The most common reason for reintubation was tachypnea. Only one patient survived until discharge. Differences in characteristics between patients experiencing reintubation (n = 4) and weaning success (n = 56) are detailed in Supplementary Table 2. In the HFNC group, the APACHE II score at the time of extubation was significantly higher than that in the COT group (18.3 ± 6.7 vs. 11.6 ± 3.3, P = 0.001). Arterial blood pH measured at the time of extubation was significantly different between the groups (7.49 ± 0.03 vs. 7.43 ± 0.07, P = 0.032).
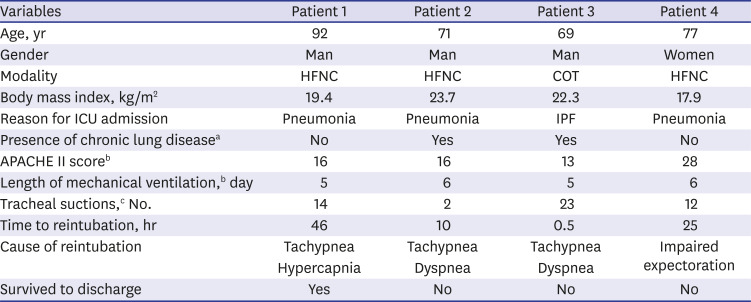
Table 3
Clinical and demographic characteristics, and outcomes of four patients, following reintubation
HFNC = high-flow nasal cannula, COT = conventional oxygen therapy, APACHE II = Acute Physiology and Chronic Health Evaluation II, ICU = intensive care unit, IPF = idiopathic pulmonary fibrosis.
aPatient 2 (pneumoconiosis), patient 3 (asthma and destroyed lung secondary to tuberculosis); bMeasured at the time of extubation; cRequired number of tracheal suctions within 24 hours after extubation.
![]()
DISCUSSION
To the best of our knowledge, this is the first randomized study to compare clinical outcomes associated with HFNC and COT in patients at high risk of reintubation in Korean population. The majority of included patients constituted older adults with chronic lung diseases. Although this was a single center study with a small sample size, it is likely to accurately reflect the characteristics of ICU patients in Korea.13 In contrast to previous studies, the present study involved a minimum 72-hour HFNC, which was longer than in a previous study.18
Compared to previous studies, the present study involved a relatively low rate of reintubation (6.7%). It is possible that patients with less severe illness or symptoms were included in the present study. In the study by Fernandez et al.,18 which compared HFNC with COT, the total rate of reintubation was 13.5% (11% and 16% in HFNC and COT, respectively). This difference might be accounted for by the discrepancy in the definition of a “high-risk” patient (presence of 2 or more risk factors) and slightly greater proportion of patients with heart failure. In other studies that compared HFNC with non-invasive ventilation (NIV), reintubation rates were higher than in the present study. In the study by Hernandez et al.,19 which included more patients with obesity and patients who required prolonged ventilation, 22.8% of patients who received HFNC required reintubation. In a study by Yoo et al.,20 which included more patients with malignancy, and chronic lung and heart disease than did the present study, 20.6% of patients who received HFNC required reintubation.
In the present study, HFNC did not reduce the risk of reintubation, length of hospital stay, or mortality rate. HFNC oxygen therapy is associated with benefits in respiratory care, and previous studies have aimed to demonstrate its clinical superiority. Despite many advantages associated with HFNC, its superiority over COT in clinical practice remains controversial, in particular, in circumstances involving post-extubation respiratory care. Song et al.21 have reported that HFNC showed a higher success rate in oxygen therapy, less discomfort, and a lower RR than an air entrainment mask; however, the authors reported no significant difference between study groups in reintubation rate during the 24-hour post-extubation period. A recent meta-analysis has reported that compared to COT, HFNC might reduce postextubation respiratory failure and RR.11 However, the authors included a heterogeneous patient group and could not demonstrate significant differences in reintubation rates, duration of ICU stay, or mortality rates. Meanwhile, Hernandez et al. have reported that HFNC oxygen therapy for a duration of 24 hours can reduce the risk of reintubation within 72 hours in a low-risk group,9 but the same study did not show significant differences in reintubation rates, duration of ICU stay, or mortality rate in the high-risk group.18
As HFNC is considered to have similar efficacy but better tolerability than NIV,20 it is widely used as postextubation modality and in postoperative care or respiratory procedures (e.g., bronchoscopy).2223 However, the cost of HFNC in Korea is three times (17,080 won/day) the cost of COT (6,240 won/day), while the circuitry for HFNC requires additional costs (19,000 won) with the support of medical insurance (20% of 95,000 won). Therefore, comparisons of effectiveness are required to ensure resources are suitably allocated. Future studies should consider this aspect of care.
Patients' comfort was not directly evaluated in the present study. We used physiologic variables to assess comfort instead of using a specific assessment tool (e.g., visual numerical scale). Except for heart rate at 24 hours after extubation, physiologic variables such as RR and P/F ratio were not different between the groups (Supplementary Table 1). Considering physiologic outcomes, flow rate changes, and COT modalities (i.e., most patients had a nasal cannula), comfort levels appear similar between two groups (Table 1).
The present study limitation was between-group heterogeneity. Recruited patients were randomized under the supervision of a statistician, using stratification based on age and gender, but not APACHE II scores. Moreover, small sample size might have contributed to between-group heterogeneity. Although our data showed higher APACHE II score in the HFNC group than in the COT group (13.3 ± 4.2 vs. 10.7 ± 3.1, P = 0.01), it might not be a clinically significant difference, as the APACHE II score-predicted mortality rates were in the same range (APACHE II score 10 to 14 predicted a 12% mortality rate among non-operative patients).17 Further large and well-designed clinical trials are required.
In conclusion, compared with COT, HFNC did not reduce the risk of reintubation within 72 hours of planned extubation, length of hospital stay, or mortality rate among patients at high risk of reintubation. Post-extubation use of HFNC in patients at high risk of reintubation, such as older adults, has no benefit that justifies the cost.
 XML Download
XML Download