

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Osteoporosis is one of the most important healthcare concerns and results in osteoporotic fractures in elderly population.12 Osteoporotic fractures lead to the decreased mobility, activity and quality of life in these population.34
Bisphosphonates, one of potent anti-resorptive agents, have been recommended to treat osteoporosis and to prevent osteoporotic fractures.25
Recent studies have reported that long-term use of bisphosphonates was associated with the increased risk of atypical femoral fractures (AFFs).67 These fractures occur spontaneously or after minimal trauma at the subtrochanteric region or femoral shaft (ST/FS).89 They are often proceeded by a prodromal pain, and have radiographic features of an insufficiency fracture; lateral cortical thickening and transverse fracture pattern,10 and are associated with high rates of non-union and reoperation.111213141516
Based on several epidemiologic studies with large scale cohorts, the incidence rate of ST/FS fractures among bisphosphonate users varies from 76 to 310 per 100,000 person-years.171819202122 Most studies were conducted in western countries involving Caucasians.1718192021
In East Asia as elsewhere, osteoporosis and osteoporotic fractures are prevalent due to aging of population,2324 and the use of bisphosphonate to prevent and treat osteoporosis becomes increasing.2225262728 Accordingly, bisphosphonate associated AFF is a growing concern in that area. 92729
Previous studies, which were conducted in health care registry of western countries, evaluated ethnic differences of AFFs and reported that the AFF incidence was higher in Asian population than in Caucasian population.293031323334 However, a recent hospital-based study showed that the AFF incidence in Korean population was not higher than those in western population.35 Therefore, the exact incidence of AFF in East Asian countries remains to be revealed. Considering the rarity of AFFs, a large epidemiologic study based on nationwide database is necessary to reveal the AFF incidence with sufficient statistical power. However, there has been no such a study conducted in East Asia.
Several studies examined the risk of AFF in long-term users of bisphosphonates. In these studies, the use of bisphosphonates was not associated with a greater risk of ST/FS fractures.17182022 Even a decreasing risk was observed with increasing average daily dose of alendronate in a nationwide cohort study from Denmark.19
Therefore, the purpose of this study was to determine the risk of ST/FS fractures and the benefit of typical hip fractures prevention among bisphosphonate users from a database on National Health Insurance Service-National Sample Cohort (NHIS-NSC).
Go to : 
METHODS
Data source
We conducted a retrospective cohort study, using the Korean NHIS-NSC database from 2002 to 2013.363738 The NHIS-NSC database comprises a semi-dynamic cohort; data regarding newborns are added to the database every year to supplement the loss of numbers due to deaths. That database was validated by its representativeness of the overall Korean population.39 It includes data on subject demographics; clinical information, such as disease diagnosis, drug prescription, and healthcare costs; beneficiary's social economic level; and death records. Disease diagnoses held in the database are coded based on the International Codes of Disease 10th Edition Clinical Modification (ICD-10-CM).
A total of 1,107,015 subjects were randomly selected from the 756 strata using three kinds of variables (age [18 groups], gender [2 groups], and income level according to type of insurance [10 groups for both NHI district subscriber and NHI employee subscriber, and one group as medical aid: total of 21 groups]) in the Korean NHIS-NSC database.3637
Data availability statement
The Korean NHIS-NSC database is not open to public. Its access is restricted to researchers, who gain an approval by NHIS. We got the NHIS approval and our study protocol was approved by Institutional Review Board of principal investigator's affiliation and NHIS.
Study population and design
The study cohort was defined as women patients, who were older than 50 years and had a prescription of bisphosphonates for the first time between January 1, 2003 and December 31, 2011. We excluded patients who had received that prescription during the preceding years to eliminate the influence of previous bisphosphonate treatment on the development of AFF.
We excluded patients, who had been previously treated for hip fractures (ICD-10: S720, S721, S722, S723), those, who had a diagnosis of malignancies (ICD-10: C*, D45*, D46*, D47, D470*, D471*, D472*) or metabolic bone disorders (ICD-10: M83*, Q780, Q782, E21*, E835*, G40*, M88*, N250) before the index date; the date of the first prescription of bisphosphonate (Fig. 1).

We identified prescriptions of intravenous or oral forms of bisphosphonates; alendronate, risedronate, etidronate, clodronate, ibandronic acid, pamidronate and zoledronate in the NHIS-NSC database, which used the Anatomical Therapeutic Chemical classification system of the World Health Organization for the record of prescriptions.40
The duration of bisphosphonate medication was calculated as daily, weekly, monthly, quarterly and annually, considering the sustained release of prescribed bisphosphonates. To determine the continuous exposure interval, “refill gap” of up to 60 days was allowed between the end of effective period of the previous prescription and the date of next prescription.31
The long-term users were defined as subjects who had taken bisphosphonate ≥ 1 year after the index date, and subjects who had taken bisphosphonate < 1 year after the index date were grouped into the short-term users, according to the criteria of Hsiao et al.22
New bisphosphonate users were followed from the index date until the date of the first hospital admission due to ST/FS fractures or typical hip fractures, end of the study period, or subject's death, whichever came first. In our study, we treated the death as a censoring event not a competing one.
Identification of AFFs
We identified patients, who had an inpatient diagnosis of ST/FS fractures (ICD-10 codes: S722 or S723) as the primary or secondary diagnosis after the index date.
From the cohort of new bisphosphonate users, we captured their first instances of inpatient claims for ST/FS fractures after index date with the ICD 10 (S722 and S723) and codes of surgical procedures; open reduction of fractured extremity-femur, closed pinning-femur, external fixation-pelvis/femur, closed reduction of fractured extremity-pelvis/femur, and bone traction.
Identification of typical hip fractures
Typical hip fracture included femoral neck (FN) and intertrochanteric (IT) fracture as the primary or secondary diagnosis. To identify typical hip fracture, from the cohort of new bisphosphonate users, we captured their first instances of inpatient claims for FN/IT fractures after index date with the ICD 10 (S720 and S721) and codes of surgical procedures; open reduction of fractured extremity-femur, closed pinning-femur, external fixation-pelvis/femur, closed reduction of fractured extremity-pelvis/femur, bone traction, hemiarthroplasty, and total hip arthroplasty.
Potential confounders
In the analysis, we included age at the index date and Charlson's index of comorbidities, which were diagnosed within 1 year before the index date, as confounding factors.
Statistical analysis
The demographic and clinical information between long-term users and short-term users was compared by descriptive statistics. Categorical variables were described by frequency and continuous variables by mean and standard deviation.
We calculated the incidence rates per 100,000 person-years by dividing the number of events by the total number of person years at risk for the ST/FS and for FN/IT fractures. We also calculated the 95% confidence interval (CI) assuming a Poisson distribution.
Cox regression models were used to estimate hazard ratios (HRs) and their 95% CIs for ST/FS and FN/IN fractures with time adjusting covariates. Adjustments were made for age and Charlson's comorbidity index score. By using this model, we could obtain an estimate of the HR of bisphosphonate use for ST/FS fractures and the protective benefit of bisphosphonate use for FN/IN fracture.
We also plotted the cumulative incidence of ST/FS and FN/IT in each group.
To determine the risk and benefit of bisphosphonate, absolute risk increase and number needed to harm (NNH) for ST/FS, and absolute risk reduction and number needed to treat (NNT) for typical hip fracture were calculated.
We used the SAS statistical application program (release 9.4; SAS Institute, Cary, NC, USA) for all statistical analyses. A two-tailed value of P < 0.05 was considered to be statistically significant.
Ethics statement
This study was approved by the Institutional Review Board of Seoul National University Bundang Hospital (B-1103/124-102). Informed consent was waived, because the data was anonymized, so study was considered exempt from review.
Go to :
RESULTS
From the 551,556 eligible women, who were included in the Korean NHIS-NSC database from 2002 to 2013, we identified 46,420 bisphosphonate users who received prescriptions for at least one bisphosphonate. Among them, 36,529 people met the inclusion criteria (Fig. 1).
After calculating duration of bisphosphonate use, 14,689 users were selected as long-term users (≥ 1 year) and 21,840 people were defined as short-term users (< 1 year) (Fig. 1). Table 1 shows the baseline characteristics of long-term and short-term users.
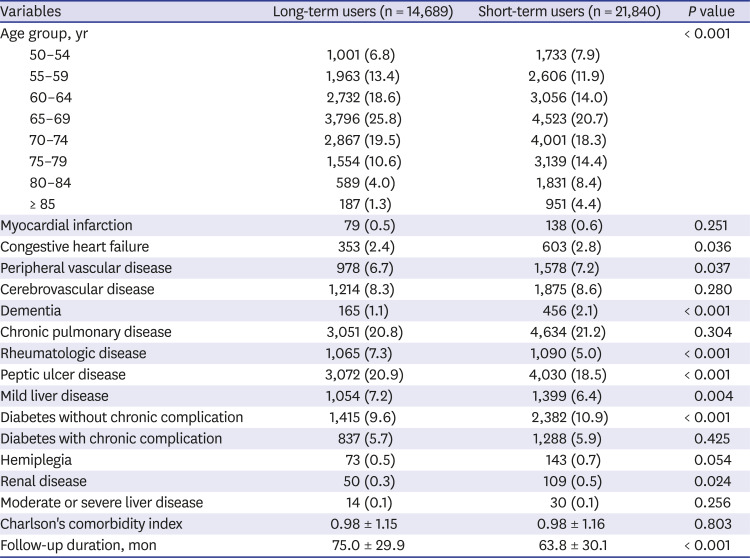
Table 1
Demographics of bisphosphonate long-term users and short-term users
![]()
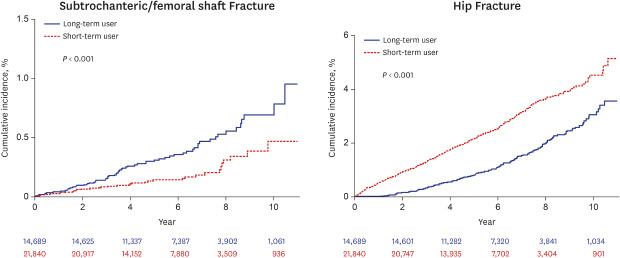
During the study period, 61 of the long-term users had ST/FS fractures, while 36 of the short-term users had such fractures. The incidence rate of ST/FS fractures was 67.1/100,000 person-years (95% CI, 50.3–83.9) in the long-term users and 31.2/100,000 person-years (95% CI, 21.0–41.4) in the short-term users. The cumulative incidence of ST/FS fracture was higher in the long-term users than in the short-term users (P < 0.001) (Fig. 2).
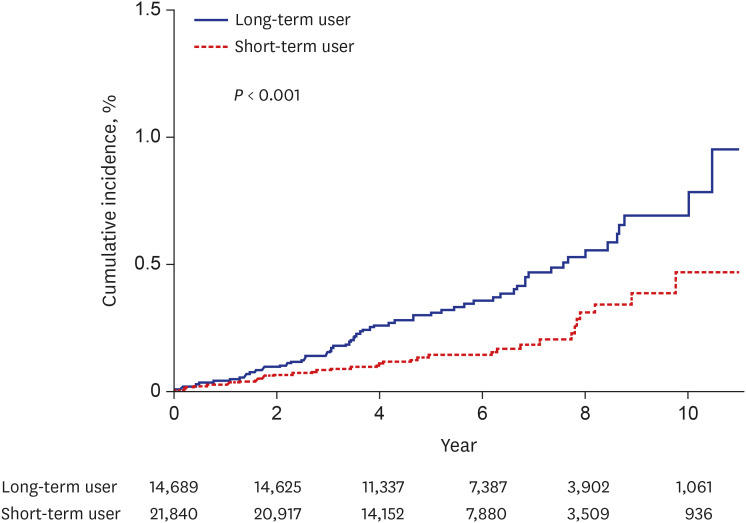
The risk of ST/FS fractures was higher in long-term users than in short-term users (adjusted HR, 2.345; 95% CI, 1.541–3.569) (Table 2).
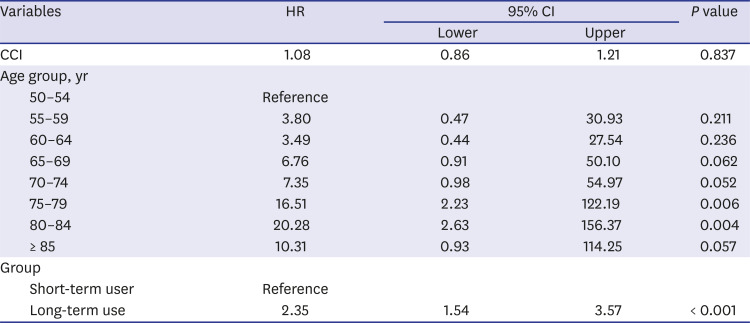
Table 2
HRs for subtrochanteric and femoral shaft fracture
![]()
During the study period, 204 of the long-term users had FN/IT fractures, while 511 of the short-term users had such fractures. The incidence rate of FN/IT fractures was 225.5/100,000 person-years (95% CI, 194.6–256.5) in the long-term users and 448.6/100,000 person-years (95% CI, 409.7–487.5) in the short-term users. The cumulative incidence of FN/IT fractures was higher in the short-term users than in the long-term users (P < 0.001) (Fig. 3).
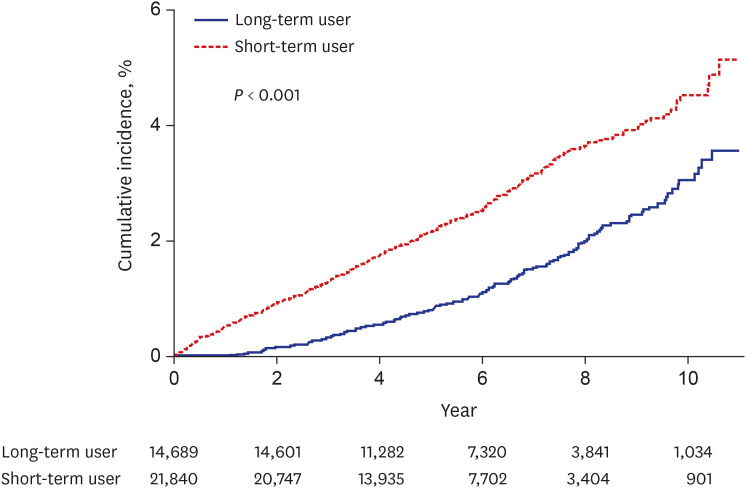
Using the short-term users as a reference, long-term use significantly reduced the risk of typical hip fracture (adjusted HR, 0.578; 95% CI, 0.490–0.682) (Table 3).
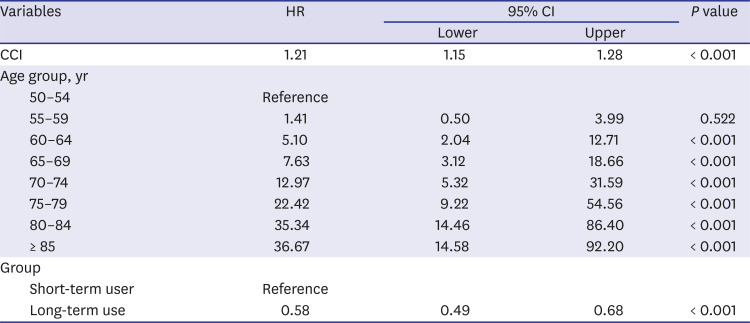
Table 3
HRs for femoral neck and intertrochanteric fracture
![]()
Absolute risk increase for ST/FS was 0.0025 (61/14,689–36/21,840) and the NNH for ST/FS was 400, which mean that one ST/FS will occur if 400 patients were treated with long-term use of bisphosphonate. Absolute risk reduction for typical hip fracture was 0.0095 (511-21,840 - 204/14,689) and the NNT for typical hip fracture was 105, which mean that 105 patients would have to be treated with long-term bisphosphonate to avoid one typical hip fracture.
Go to :
DISCUSSION
In this population-based cohort study using diagnostic and procedure codes, we found out the association between the long-term use of bisphosphonate and the risk of ST/FS fractures. However, our results showed that the long-term use of bisphosphonate (≥ 1 year) was associated with the reduced risk of FN/IT fractures.
The incidence rate of ST/FS fractures was 67.1/100,000 person-years, which was comparable with or lower than reportedly known rates in western countries (Table 4).172022

Table 4
Incidence rate of subtrochanteric and femoral shaft fracture identified using code system after bisphosphonate use
| Authors | Country | Study period | Age, yr | No. of bisphosphonate users | Incidence rate (/100,000 patients-yr) |
|---|---|---|---|---|---|
| Abrahamsen et al.17 | Denmark | 1997–2005 | > 60 | 5,187a | 280 |
| Abrahamsen et al.18 | Denmark | 1996–2005 | NA | 39,567a | 310 |
| Hsiao et al.22 | Taiwan | 2001–2007 | NA | 2,425a | 155 |
| Kim et al.20 | USA | 1996–2006 | NA | 17,028 | 146 |
| Wang et al.21 | USA | 2006–2010 | > 65 | 522,287 | 76 |
| Current study | Korea | 2003–2011 | > 50 | 14,689 | 67.1 |
![]()
The estimated incidence rate might be overestimated in our study because we could not exclude high energy fractures by using ICD-10 codes. Nevertheless, we observed a much lower incidence rate of ST/FS fractures in Korea than those of western countries (Table 4).172022
Our results were not consistent with those of previous studies, which reported that the occurrence of ST/FS fractures was higher in Asian than Caucasian.293031323334
Several studies reported that the use of bisphosphonate was not associated with an increased risk of AFFs,1718192022 while other studies have demonstrated that the occurrence of those fractures was significantly associated with the long-term use of bisphosphonate.717202122294142 Our study showed that the long-term use of bisphosphonate (≥ 1 year) was a potential risk factor of ST/FS fractures.
On the other hand, many clinical trials and registry-based cohort studies have reported that bisphosphonate use provides benefits of hip fracture prevention.2643 Several guidelines on osteoporosis treatment have recommended use of bisphosphonate to prevent osteoporotic fractures.44454647 Our results supported these guidelines and those studies on benefits of bisphosphonate on fracture prevention.
Our results, the difference between NNH (400) for ST/FS and NNT (105) for typical hip fracture, mean that just one ST/FS could occur, while 4 typical hip fractures would be prevented, if 400 patient was treated with long-term bisphosphonate. Our findings showed that the benefit of long-term use of bisphosphonate for prevention of typical hip fracture was larger than the risk for ST/FS.
Our study has several strengths. First, our cohort was one of the largest from Asian, allowing us to investigate even rare events such as AFFs. Second, we conducted population-based study design using a nationwide claims database containing drug prescriptions.
There were several limitations in this study. First, although we used a very large cohort, our cohort was a sampled one and might not have represented the entire female population in Korea. However, the Korean government provided a standardized cohort by using stratification according to the age, gender, and level of socioeconomic status. Second, we could not evaluate radiographs to confirm the atypical features of ST/FS fractures. This study might have a potential bias due to inaccurate coding and incomplete medical records.48 However, previous several studies on the epidemiology of AFFs have used the same coding system.171819202122 A evaluation for the validity of discharged diagnosis showed that the overall positive predictive value of the diagnoses was 83.4% in patients, who were admitted to hospital.49 Third, we could not analyze possible confounding factors such as menopausal status, bone turnover status, and bone mineral density, because the claim database did not include these. Fourth, fracture due to high-energy injury might be included in this study, because the ICD-10 coding system did not distinguish between high and low-energy fractures. However, we did not need an additional operational definition to exclude high energy trauma, because the NHIS database does not include high-energy injuries such as those from traffic accidents and industrial injury.50
Despite these limitations, our results showed that bisphosphonates may be playing a differential role between FN/IT fracture and ST/FS fracture. The longer use of bisphosphonate was associated with the lower risk of typical hip fracture, while it was associated with the higher risk of occurrence of ST/FS fractures in Korean women. Our study suggested that the raised concerns about bisphosphonate-associated ST/FS fractures in East Asia may be overestimated than the reality, considering the longer use of bisphosphonate was associated with the lower risk of FN/IT fractures.
Go to :
 XML Download
XML Download