

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Hip fracture in the elderly is associated with high mortality rates.1 Hip fracture not only causes dysfunction and poor quality of life, but also places economic burdens on families.23 For this reason, this fracture is a major public health problem in the geriatric population; prevention and early management are very important.4
End-stage renal disease (ESRD) is also a public health problem associated with advanced age.4 The incidence of dialysis is greater in elderly patients with ESRD and they also have higher mortality rates, despite the fact that dialysis is performed to prevent uremia.56 In ESRD patients, hip fracture risk increases from 4.1 times to 17.4 times compared to that of the general population.78 Hyperphosphatemia, decreased vitamin D concentrations with declining glomerular filtration rate (GFR), and increased fibroblast growth factor 23 and parathyroid hormone levels contribute to weakening of the bony structure.59 In addition, comorbidities such as diabetes mellitus and metabolic acidosis exacerbate bone mineral metabolism and reduce physical activity.67 Nevertheless, the effect of dialysis on mortality after hip fracture is rarely reported in Korea.810
If hip fracture occurs in ESRD patients, preoperative delay can occur frequently due to preoperative electrolyte imbalance, low hemoglobin levels, and dialysis schedules. Complications such as wound hematoma, infection, implant failure, and nonunion are more likely to occur after surgery.11 Rehabilitation is also difficult due to ambulation restriction during dialysis. Therefore, the purpose of this study was to analyze all-cause mortality rate over time after hip fracture in elderly ESRD patients undergoing dialysis using a Korean nationwide claim database.
Go to : 
METHODS
Study subjects
This retrospective nationwide study identified subjects from the Korean National Health Insurance Service-Senior cohort (NHIS-Senior) compiled by the Korean NHIS. This database included approximately 5.5 million Korean enrollees > 60 years of age in 2002. The NHIS-Senior was constructed to represent the elderly living in Korea. A total of 588,147 participants were randomly selected for this study using 10% simple random sampling. All individuals included in the NHIS-Senior were followed up until 2015 unless they died or were disqualified for National Health Insurance (e.g., because of emigration). The NHIS is a single-insurer system providing universal health coverage, maintaining all personal information, demographics, and medical treatment data for Korean citizens who are categorized as insured employees, insured self-employed individuals, and medical aid beneficiaries.1213 The information in the data set included all inpatient and outpatient medical claims data, including treatment procedure codes and diagnostic codes.
Elderly hip fracture cohort
Eligibility criteria for elderly hip fracture patients were as follows: 1) first-time admission to an acute care hospital (index admission) with diagnostic codes of femoral neck fractures (International Classification of Diseases, 10th Revision [ICD-10] S720) or intertrochanteric fracture (ICD-10 S721)1415; 2) having at least a three-year hip fracture-free period; 3) undergoing typical surgeries, including internal fixation (open reduction of fractured extremity [femur], closed pinning [femur]), hemiarthroplasty (hip), or total arthroplasty (hip); and 4) age 65–99 years at the time of a hip fracture to assure inclusion of only osteoporotic hip fractures.15 To ensure a minimal 1-year follow-up period, patients with hip fractures occurring less than 1-year before the end of the observation period (December 31, 2015) were excluded. Patients with hip fractures prior to December 31, 2004, were also excluded to guarantee at least a 3-year hip fracture-free period. Incidence date (index date, time zero) of hip fracture was defined as the date of admission to the acute care hospital that fulfilled eligibility criteria. The last date of follow-up was defined as the date of death or December 31, 2015, whichever came first.
Renal dialysis
Diagnostic codes used in this study were N18, N19 based on validation study of ICD-10 for identifying ESRD.16 Codes for treatment were O7011-O7020 for hemodialysis, and O7071-O7075 for peritoneal dialysis.16 Renal dialysis patients were defined as follows: 1) patients with both diagnostic codes and treatment codes; and 2) patients who had peritoneal dialysis records or at least four episodes of hemodialysis records per month within 3 months before the index date.
All-cause mortality
In the NHIS-Senior, each subject's unique de-identified number was linked to mortality information from the Statistics Korea.13
Statistical analysis
Baseline characteristics were identified at time zero. Survival time was defined as days from the index date to dates of death or December 31, 2015, whichever occurred first. Cumulative survival probabilities and survival curves were calculated and plotted using the Kaplan–Meier method and the product-limit formula. A generalized estimating equation model with Poisson distribution and logarithmic link function was used to estimate adjusted risk ratios (aRRs) and 95% confidence intervals (CIs) to assess association between renal dialysis and cumulative mortality at various time frames (30-day, 60-day, 90-day, 180-day, 1-year, 2-year, and 3-year risk).
Included covariates were age group, gender, household income level, residential area, Charlson comorbidity score (CCS), fracture type, surgery type, anesthesia types, length of hospital stay (LOS), number of hospital days, and calendar year of the hip fracture incidence. Each subject's number of comorbidities was assessed by diagnostic codes during three years before the index date using the Quan ICD-10 coding algorithm of the CCS.17 The presence of CCS disease-constituting categories was defined by at least two outpatient visits or one admission upon the primary or first secondary diagnosis. All statistical analyses were conducted using SAS Enterprise Guide version 7.1 (SAS Institute, Cary, NC, USA). P values < 0.05 were considered statistically significant.
Ethics statement
The protocol of this study was approved by Institutional Review Board of Eulji University Hospital (No. EMC 2020-02-002). Informed consent was waived due to the retrospective nature of this study.
Go to :
RESULTS
From January 1, 2002 to December 31, 2015, 19,915 patients were hospitalized for hip fractures. Of these, 3,097 patients were excluded (1,478 patients for non-operative treatment, 1,374 did not meet the hip fracture-free period and 1-year follow-up, and 245 patients were under 65 or over 99 years of age). Finally, the total number of patients was 16,818. These patients were divided into two groups: 116 (0.69%) in the dialysis group and 16,702 (99.31%) in the no-dialysis group (Table 1). In the dialysis group, six (5.17%) patients had peritoneal dialysis prior to hip fracture. There were significant differences between the groups in terms of demographic characteristics (except for fracture type, LOS, surgery type, and calendar year) (all P < 0.05). The dialysis group had a higher rate of males, femoral neck fractures, low-income groups, and higher CCS groups (all P < 0.05). The mean LOS was 43.87 ± 48.45 days in the dialysis group and 36.29 ± 37.49 days in the no-dialysis group (P = 0.095).
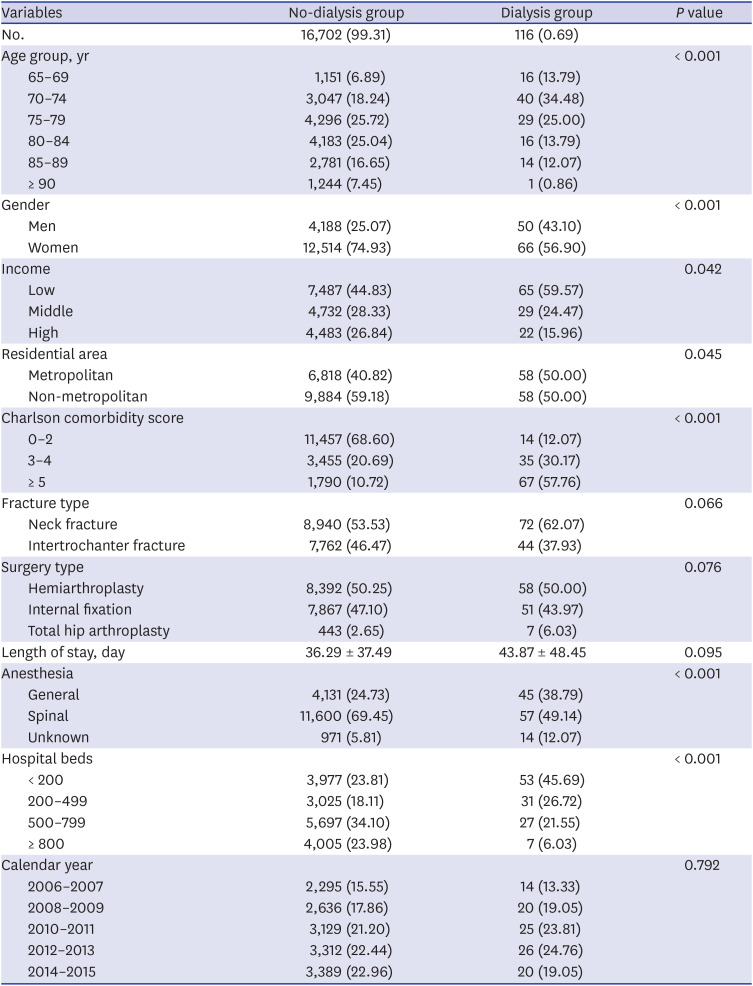
Table 1
Baseline characteristics of study participants
![]()
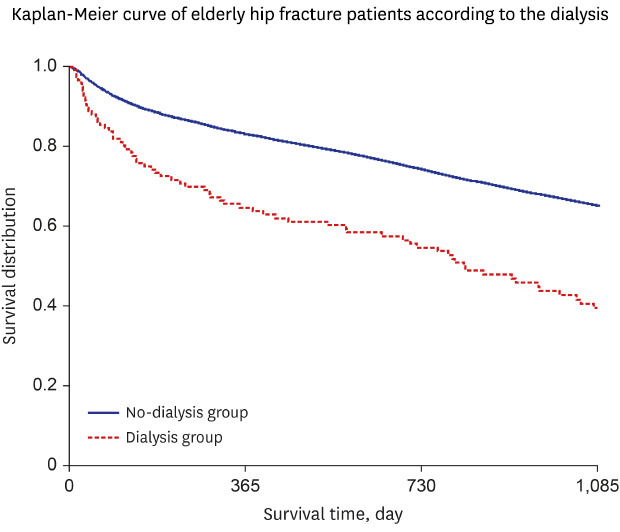
The 30-day, 60-day, 90-day, 180-day, 1-year, 2-year, and 3-year cumulative mortality rates were 2.44%, 5.13%, 7.32%, 11.42%, 16.87%, 25.68%, and 32.88% in the no-dialysis group, and 7.76%, 13.79%, 17.24%, 26.72%, 35.34%, 44.83%, and 57.76% in the dialysis group, respectively (Table 2 and Fig. 1). The in-hospital cumulative mortality rates were 4.02% in the no-dialysis group, and 13.79% in dialysis group.
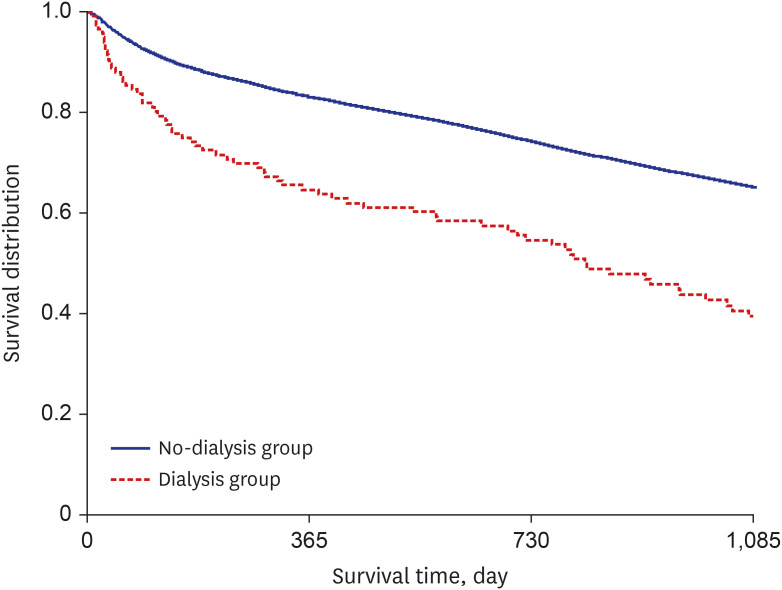 | Fig. 1Kaplan-Meyer curve of older patients with hip fracture according to renal dialysis.
P value of Log-rank test was < 0.001.
|
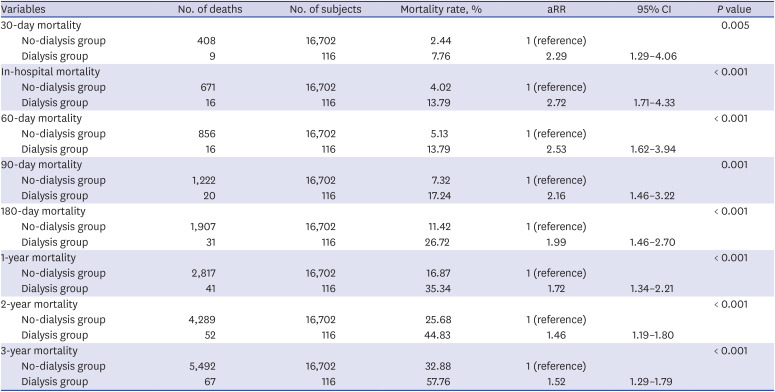
Table 2
Effect of renal dialysis on all-cause mortality of different time frame
![]()
The effect of renal dialysis on all-cause mortality was 2.29-fold (aRR; 95% CI, 1.29-4.06; P = 0.005) within 30-days and 2.53-fold (aRR; 95% CI, 1.62–3.94; P < 0.001) within 60 days compared to the no-dialysis group. The effect of renal dialysis on all-cause mortality was 1.72-fold (aRR; 95% CI, 1.34–2.21; P < 0.001) within 1-year after hip fracture compared to the no-dialysis group (Table 2). The effect of renal dialysis of in-hospital mortality was 2.72-fold (aRR; 95% CI, 1.71–4.33; P < 0.001) compared to the no-dialysis group.
Go to :
DISCUSSION
The main findings of this study are as follows: ESRD patients who underwent preoperative dialysis among older patients with hip fracture were only 0.69% of the total; however, the 1-year mortality rate was very high at 35.34%. The in-hospital cumulative mortality rates were 4.02% in the no-dialysis group, and 13.79% in the dialysis group. The effects of renal dialysis on all-cause mortality were 2.29-fold within 30 days, 2.72-fold during hospitalization, and 1.72-fold within 1-year after hip fracture compared to the non-dialysis group.
Kidney disease increases the risk of cardiovascular disease and type 2 diabetes.18 The causes of increasing risk for cardiovascular disease are associated with chronic kidney disease-mineral bone disorder syndrome (CKD-MBD), such as vascular calcification, elevated fibroblast growth factor 23, hypophosphatemia, osteodystrophy, and others.19 The CKD-MBD disrupt the normal physiology in kidney, skeleton, cardiovascular system and have a negative impact on survival for elderly patients.20 Nitsch et al.21 reported that hip fracture-related mortality doubled in patients with GFR below 45. Mittalhenkle et al.22 reported a 1.99-fold increase in average relative risk of mortality in patients with ESRD (Table 3).21222324 Hung et al.4 performed a nationwide population-based observational study in China and reported that adjusted hazard ratios after fracture in ESRD patients were 2.58, 2.95, 2.84, and 2.39 within 3 months, 3 months to 1 year, 1 to 6 years, and 6 to 10 years, respectively. Lin et al.25 performed a national cohort study in Taiwan and reported that in-hospital mortality was 3.2% and 1-year mortality was 25.4% after hip fracture. Mittalhenkle et al.22 found that 1-year survival of ESRD patients after hip fracture was 50%. Ibarra Melogno et al.26 reported mortality rates after hip fracture in the dialysis group with mean age 72.3 years; mortality rates at 30 days, 180 days, 1 year and 5 years were 7.1%, 18.2%, 29.3%, and 82.6%, respectively. The 1-year mortality rate after hip fracture in ESRD patients varied from 4.4% to 44.4% depending on the type of fracture and the surgical method.2728293031
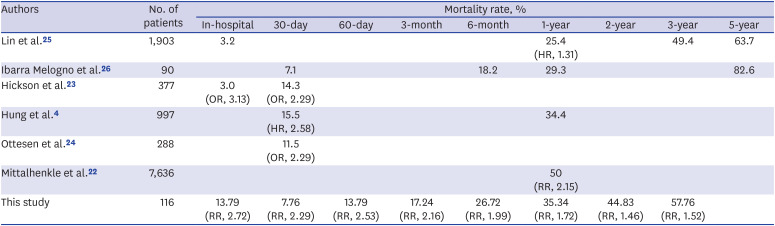
Table 3
Summary of mortality rates in previous studies for dialysis patients with hip fracture
| Authors | No. of patients | Mortality rate, % | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| In-hospital | 30-day | 60-day | 3-month | 6-month | 1-year | 2-year | 3-year | 5-year | ||
| Lin et al.25 | 1,903 | 3.2 | 25.4 (HR, 1.31) | 49.4 | 63.7 | |||||
| Ibarra Melogno et al.26 | 90 | 7.1 | 18.2 | 29.3 | 82.6 | |||||
| Hickson et al.23 | 377 | 3.0 (OR, 3.13) | 14.3 (OR, 2.29) | |||||||
| Hung et al.4 | 997 | 15.5 (HR, 2.58) | 34.4 | |||||||
| Ottesen et al.24 | 288 | 11.5 (OR, 2.29) | ||||||||
| Mittalhenkle et al.22 | 7,636 | 50 (RR, 2.15) | ||||||||
| This study | 116 | 13.79 (RR, 2.72) | 7.76 (RR, 2.29) | 13.79 (RR, 2.53) | 17.24 (RR, 2.16) | 26.72 (RR, 1.99) | 35.34 (RR, 1.72) | 44.83 (RR, 1.46) | 57.76 (RR, 1.52) | |
![]()
In the present study, the 30-day, 60-day, 90-day, 180-day, 1-year, 2-year, and 3-year cumulative mortality rates were 7.76%, 13.79%, 17.24%, 26.72%, 35.34%, 44.83%, and 57.76% in the dialysis group, respectively. The in-hospital cumulative mortality rates were 13.79% in the dialysis group. Hung et al.4 reported that short-term mortality rates were 5.9%–22.9% and long-term mortality rates were 19.8%–45.2%, depending on the degree of renal function according to GFR. The various mortality rates in previous studies were due to differences in kidney function, although fracture types and surgical methods varied. The mortality rates of the present study are comparable to those reported in previous studies.
Hip fracture patients are susceptible to surgical delay, a factor that can increase postoperative mortality.11 Cha et al.1 reported that surgical delay increased 30-day mortality 2.78-fold. One of the most important factors affecting death due to delay in surgical treatment is underlying disease.1 In dialysis patients, electrolyte abnormalities and metabolic acidosis due to kidney dysfunction are common and are frequently accompanied by anemia.11 Bleeding associated with hip fracture causes hemoglobin levels to fall. Even if hip fracture surgery is performed after control of the dialysis schedule, their rehabilitation progress is slow and postoperative complication rates are high (e.g., wound hematoma and infection).11 For these reasons, in-hospital mortality is greater and lengths of stay after the hip fracture are prolonged in dialysis patients. Kim et al.9 reported that dialysis patients had a 1.69-fold increased risk of in-hospital mortality compared to those with normal renal function, as well as greater lengths of stay and treatment costs. In the present study, the mean length of stay in the dialysis group was 43.87 days, longer than that of no-dialysis patients, associated with a 2.72-fold higher risk of in-hospital mortality.
This study has several limitations. First, bone mineral density, laboratory data (such as vitamin D, calcium, body mass index, and dialysis adequacy), patient compliance, nutritional status, sarcopenia were not considered because this study was based on national claims data. For this reason, other risk factors for mortality might not have been considered. Nevertheless, we attempted to overcome this limitation by adjusting for CCS and socio-economic factors such as income level and residential area. Second, the national claims data did not collect information about preoperative medical optimization or postoperative prevention programs. For this reason, our results do not reflect differences in protocols between hospitals. Third, the criteria of this study for inclusion of osteoporotic hip fracture does not reflect the injury mechanism, such as falling from a height. However, the reference study for these criteria suggested high predictive values for osteoporotic hip fracture, and we added the restriction of age over 65 years for reinforcing limitations of inclusion criteria of reference study.
In conclusion, elderly patients who underwent dialysis have very high mortality rates after hip fracture. Therefore, it is considered that postoperative care through multidisciplinary management and understanding of pathophysiology for the ESRD patients is necessary.
Go to :
 XML Download
XML Download