

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Endoscopic examination has undergone massive advancements to enable its use in pediatric patients, while being used for the last 30 years to diagnose and treat various gastrointestinal (GI) diseases. In addition to routine diagnostic esophagogastroduodenoscopy (EGD) or colonoscopy, procedures such as polypectomy, endoscopic hemostasis, therapeutic foreign body removal, endoscopic retrograde cholangiopancreatography, and endoscopic ultrasound are also conducted in pediatric patients.123 The prevalence of using endoscopies for diagnoses and treatments in pediatric patients is gaining popularity particularly in Korea, as observed in other countries, and the number of trials is gradually increasing. However, unlike adults, pediatric patients may experience increased discomfort while undergoing invasive tests such as endoscopy, because of preconceived abstinence from the procedure or anxiety and adherence issues.456 Moreover, endoscopy is a painful procedure, unlike magnetic resonance imaging or electroencephalography, often requiring the use of analgesic medications. Especially, the risk of complications increases if the patient cannot cooperate with the procedure.67 Therefore, it is increasingly common to plan deep-level sedation for pediatric patients prior to undergoing endoscopy.89 However, in clinical practice in healthcare institutions in Korea, sedation is induced and monitored in most cases by the endoscopy operator who performs the endoscopic examination rather than a specialist in anesthesiology. This challenge is multi-factorial, and there is a dearth of data on the type and dose of the drugs used for sedation. Further, there is a considerable level of panic among pediatric patients during endoscopic procedures, thereby eliciting forcible suppression by assistants.
Most importantly, in Korea, no studies have yet described the types of sedation drugs, effects of sedation, and efficiency of endoscopy with respect to the sedation instructor. Hence, in this study, we investigated the effectiveness of sedative procedures performed by anesthesiologists.
Go to : 
METHODS
Patient selection
We retrospectively reviewed the medical records of patients aged < 18 years who underwent endoscopy at the Chung-Ang University Hospital during March 2014–July 2019. The endoscopy room in the hospital is used jointly for adult and pediatric patients. At our hospital, during adult and pediatric endoscopies, sedation is performed and monitored by anesthesiologists and nurses of the anesthesiology department since 2014; this is in contrast to the procedure followed in most other hospitals in Korea. The drugs used for sedation in endoscopy include intravenous midazolam (Midazolam Bukwang Inj. 5 mg/5 mL, 1 mg/mL; Bukwang Pharmaceutical Co., Ltd., Seoul, Korea), ketamine (Huons Ketamine HCl Inj. 10 mL, 50 mg/mL; HUONS, Seongnam, Korea), and propofol (50 mL [vial] of Fresofol Mct 1% Inj. 50 mL [vial] 1% strain, 10 mg/mL; Fresenius Kabi Austria GmbH, Graz, Austria). Subsequently, the postprocedural recovery time was checked by an anesthesiologist. This is a routine process performed for almost all endoscopic procedures; however, the endoscope operator may perform the sedation intermittently during the weekend or when an anesthesiologist is unavailable. During the study period, the endoscope operator was common for all pediatric endoscopies, and sedations in all cases were performed by the same operator or a single anesthesiologist.
Endoscopic examinations performed in the neonatal intensive care unit, operation room, and intensive care unit were excluded from the study. Patients with neurological problems or structural abnormalities in the GI tract, such as esophageal duplication, were excluded because these problems might affect the type and dose of sedation drugs and the recovery time. We also excluded the cases of therapeutic endoscopies, such as those involving bleeding control, polypectomy, or foreign body removal. Finally, we analyzed the records of all patients aged < 18 years who underwent upper or lower GI endoscopy for simple diagnosis or examination in general with no underlying illnesses. The final selection of patients was classified based on the sedation performed by the endoscope operator and sedation performed by the anesthesiologist.
We collected data of the patients' clinical background, the doctor who conducted sedation, type and dose of the drug, complications, and extent of recovery after sedation, through medical records. The examination time was measured since the first endoscopic image was recorded while the endoscope was inserted into the oral cavity or through the anus to the time point of recording the last image just before the tube was removed from the oral cavity or anus to complete the examination. The degree of recovery from anesthesia was determined by checking eye-opening, verbal response, and orientation recovery as cognitive parameters and correlated with the time to reach a ≥ 9 score per the standard of discharge in the Aldrete scoring system.1011 To exclude variations according to the combination of drugs used, we analyzed only those for whom almost the same dose of midazolam was used first for inducing sedation and then for maintenance of sedation with increased propofol dosage. Patients for whom sedation was maintained through ketamine were excluded from the analysis of recovery. The recovery time was determined based on the drug dose per body weight according to the procedure time.
Statistical analysis
Statistical analysis was performed using SPSS 18.0 statistical software (SPSS Inc., Chicago, IL, USA). The χ2 test and Student's t-test were used to compare the groups and the mean and standard deviations were presented. The Mann-Whitney test was used to compare the group that underwent colonoscopy and EGD with the group that underwent only colonoscopy. The linear regression test was used to compare the sedation time and recovery time according to the use of propofol.
Ethics statement
This study was conducted with approval from the Institutional Review Board (IRB) of the Chung-Ang University Hospital (IRB No. 1706-004-16074), and informed consent was waived due to the retrospective nature of the study.
Go to :
RESULTS
Clinical characteristics of all pediatric patients undergoing endoscopy
Between March 2014 and July 2019, 257 patients aged under 18 years underwent diagnostic endoscopies at Chung-Ang University Hospital, which were conducted by the same pediatric endoscopist (Table 1). Of them, 217 patients (mean age, 11.8 ± 4.1 years; 40.1% male) underwent EGD and 40 patients (mean age, 15.1 ± 2.7 years; 45.0% male) underwent colonoscopy. Overall, 54 (24.9%) and 16 (40.0%) patients were diagnosed with organic diseases, such as GI invasion of Henoch-Schönlein purpura, Helicobacter pylori gastritis, and inflammatory bowel disease, based on EGD and colonoscopy findings. Of the patients who underwent EGD, 29 (13.4%) underwent sedation by the pediatric endoscopist and 188 (86.6%) underwent sedation by the anesthesiologist. All 40 patients who underwent colonoscopy were sedated by the anesthesiologist.
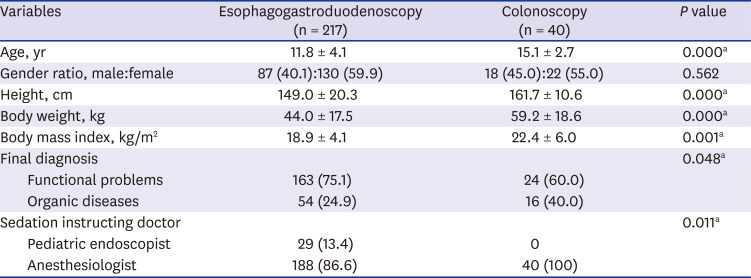
Table 1
Clinical characteristics of all pediatric patients undergoing endoscopy
![]()
Table 2 displays the different clinical characteristics according to the sedation instructor for 217 patients who underwent EGD. There were no differences in age, sex, height, weight, or body mass index between both groups. When the anesthesiologist performed the sedation, organic diseases were less frequently diagnosed (22.9% vs. 37.9%); however, this difference was statistically nonsignificant. Endoscopic examinations consumed more time when the anesthesiologist induced anesthesia than when the sedation was performed by the pediatric endoscopist (401.0 ± 135.1 seconds vs. 274.9 ± 106.1 seconds, P < 0.001).
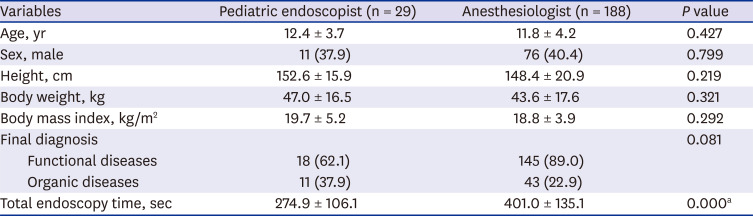
Table 2
Clinical characteristics of esophagogastroduodenoscopy patients according to the sedation instructor
![]()
Comparison of drugs for sedation in pediatric patients undergoing endoscopy
Among the 217 pediatric patients who underwent EGD, sedation drugs were compared according to the sedation instructor (Table 3). Midazolam was used in all patients of both groups, but there was a significant difference in the dosage and the dose per weight (4.35 ± 0.91 mg vs. 0.89 ± 1.47 mg, P = 0.000; 0.10 ± 0.03 mg/kg vs. 0.03 ± 0.08 mg/kg, P = 0.000, respectively). Ketamine did not show any difference between both groups in terms of the total dosage (P = 0.776); however, higher doses per body weight were used by the anesthesiologist (0.50 ± 0.10 mg/kg vs. 0.65 ± 0.42 mg/kg, P = 0.005). The pediatric endoscopist did not use propofol, but the anesthesiologist used a 2.50 ± 0.95 mg/kg dose of propofol in 181 patients (96.3%).
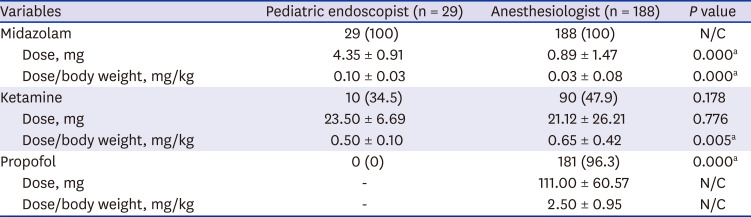
Table 3
The drugs used for anesthesia in esophagogastroduodenoscopy patients according to the sedation instructors
Data are presented as mean ± standard deviation or number (%).
N/C = not checked
aSignificant findings at P < 0.05.
![]()
Of the 40 colonoscopy cases, 36 were those of colonoscopy with EGD and 4 underwent colonoscopy alone. No significant differences were observed in the drugs used or their doses between the patients who underwent colonoscopy with EGD and those who underwent colonoscopy only; the endoscopy duration was 35.0 (25–65) minutes and 26.5 (26–36) minutes for both sub-groups, respectively (P = 0.028).
We compared the doses of drugs used by the anesthesiologist for inducing anesthesia before EGD and colonoscopy (Table 4). The number of cases of midazolam administration, the dose, and dose per body weight used did not differ between the two groups (P = 0.175, P = 0.539, and P = 0.344, respectively). Ketamine was used in more patients who underwent EGD alone than in those who underwent EGD and colonoscopy (47.9% vs. 20.0%, P = 0.001); however, the dose in patients using ketamine did not differ between the two groups (dose and dose per body weight, P = 0.54 and P = 0.165, respectively). Propofol was used in both groups. Unlike the cases of administering midazolam and ketamine, when propofol was used, the total drug dose and dose per body weight increased since colonoscopy lasted longer than EGD (111.00 ± 60.57 mg vs. 268.08 ± 98.25 mg, P = 0.000; 2.50 ± 0.95 mg/kg vs. 4.71 ± 1.66 mg/kg, P = 0.000, respectively).
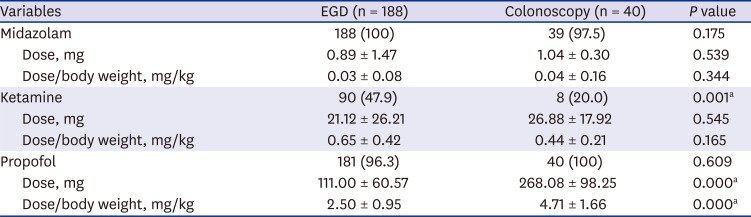
Table 4
Comparison of drug doses in patients sedated by the anesthesiologist
Data are presented as mean ± standard deviation or number (%).
EGD = esophagogastroduodenoscopy.
aSignificant findings at P < 0.05.
![]()
Comparison of recovery time after sedation and dose per weight of propofol according to endoscopy time
Tables 5 and 6 show the comparison of recovery time after sedation and the dose per weight of propofol according to endoscopy time. The recovery time was measured in 80 (midazolam dose, 0.015 ± 0.008 mg/kg) patients who underwent EGD alone and 25 (midazolam dose, 0.016 ± 0.003 mg/kg) patients who underwent colonoscopy. In EGD, which had a relatively short endoscopy time, the dose of propofol per endoscopy time was significantly correlated with cognitive parameters such as eye-opening, verbal response, and time of orientation recovery (P = 0.024, P = 0.018, and P = 0.019, respectively). Conversely, the recovery time with an Aldrete score of 9 and above as standard of discharge was not correlated with the dose of propofol per the endoscopy time (P = 1.000). In contrast, colonoscopies had a relatively long endoscopy duration and the dosage of propofol according to the duration of endoscopy was nonsignificantly associated with any indicator of recovery.


Table 5
Comparison of recovery time according to the propofol dose per weight and endoscopic time: Recovery characteristics of patients who underwent EGD with maintenance doses of propofol (n = 80)
| Variables | Time, min | P value | β |
|---|---|---|---|
| Eye opening | 19.91 ± 11.10 | 0.024a | 0.253 |
| Verbal | 20.49 ± 10.74 | 0.018a | 0.264 |
| Orientation | 22.04 ± 10.03 | 0.019a | 0.263 |
| Score 9 | 23.81 ± 9.97 | 1.000 | 0.185 |
EGD = esophagogastroduodenoscopy; Score 9 = the time required for accomplishing an Aldrete score ≥ 9.
aSignificant findings at P < 0.05.
![]()
Table 6
Comparison of recovery time according to the propofol dose per weight and endoscopic time: Recovery characteristics of patients who underwent colonoscopy with maintenance doses of propofol (n = 25)
| Variables | Time, min | P value | β |
|---|---|---|---|
| Eye opening | 23.80 ± 9.82 | 0.342 | 0.198 |
| Verbal | 24.88 ± 9.60 | 0.303 | 0.214 |
| Orientation | 26.52 ± 9.12 | 0.385 | 0.182 |
| Score 9 | 28.40 ± 9.19 | 0.666 | 0.091 |
EGD = esophagogastroduodenoscopy; Score 9 = the time required for accomplishing an Aldrete score ≥ 9.
![]()
Drug use for endoscopic sedation and subsequent complications
Some complications were reported in 1 patient (3.4%) and 23 patients (12.2%) in both groups (P = 0.214). Among the sedations performed by the endoscopist, we noted one case of ketamine overdose caused hypotension due to a dose measurement error that required oxygen administration. Among the cases of sedation performed by the anesthesiologist, one patient, who cried severely before the endoscopic procedure, required 5-litre O2 administration because of ≤ 90% desaturation with cough and secretion after the endoscopy. Additionally, there was 1 case of bradycardia and 1 case of dystonia. In other cases, complications, such as transient cough, hiccup, snoring, irritability, chilling, intravenous line leakage, dizziness, and diplopia, were noted; however, these cases recovered without special treatment. Unlike when sedation was performed by an endoscopic operator, in the case of sedation performed by the anesthesiologist, there were no cases of complaints of pain, memory related to the sleep process, or discomfort due to insufficient sedation.
Go to :
DISCUSSION
As mentioned previously, the anesthesiologist determines the use of drugs for sedation and monitors the process during endoscopic procedures, which occurs only at the Chung-Ang University Hospital in Korea. Therefore, to the best of our knowledge, this is the first report in Korea on anesthesia conducted by an anesthesiologist in pediatric endoscopy. In the present study, we report the successful implementation of performing sedation by anesthesiologists as opposed to the conventional practice of inducing anesthesia by pediatric endoscopists.
Substantial immobilization of uncomfortable and emotionally disturbed pediatric patients is essential for the successful implementation of pediatric GI procedures, such as endoscopy.1213 In some cases, light sedation was used, but was often considered as insufficient. Therefore, currently, general anesthesia is regularly used.1314 Nevertheless, there are limitations to this for reasons such as the lack of anesthesiologists and cost-related concerns. Additionally, it is not an easy procedure to perform, especially in Korea. With this background, our experience of sedation performed by anesthesiologists in the endoscopy room revealed important aspects. First, when sedation was performed by an anesthesiologist, various drugs could be used in sufficient doses. Antidote-free analgesic drugs such as ketamine were also safe to use, and propofol was also available in sufficient doses. Nonetheless, significant complications were infrequent and were mostly temporary. Secondly, the endoscopist could concentrate on the endoscopy itself and could sufficiently examine the patient since the patient's sedation need not be monitored. Sedation-related monitoring was conducted by a specialist, and, in the cases of incomplete sedation, endoscopies could be performed in a stable state due to the use of additional drugs. Moreover, patient satisfaction was also very high.
The guidelines of the American Society for Gastrointestinal Endoscopy recommend this sedation protocol to ensure the safety, comfort, and cooperation of pediatric patients undergoing endoscopy.141516 Nearly all children who receive GI procedures are advised to opt for endoscopist-administered moderate sedation or anesthesiologist-administered deep sedation, and general anesthesia. Moreover, previous studies emphasized the advantages of anesthesiologist-administered sedation.591516 In addition to the same advantages we experienced, previous studies reported that sedation can be adequately performed in patients with various risk factors, and the risks of complications were lower. In particular, the effects of sedation with propofol were emphasized. Propofol is an ultra-short acting sedative agent that rapidly crosses the blood-brain barrier, enabling early-onset action. Because of its very short distribution half-life and prompt recovery, it has recently become preferable in endoscopy.17 Previous studies confirmed that propofol can be used relatively safely without severe complications in pediatric endoscopy.1218192021 However, the use of propofol alone does not rule out the possibility of cardiorespiratory complications, which may occur with a significantly higher incidence than with other regimens.22 There is still considerable debate about endoscopist-administered propofol.2324 The use of propofol in pediatric patients requires further analysis.25 Therefore, procedures such as pediatric endoscopy should be proactive and specialists in anesthesiology should be recruited such as, anesthesiologists, in Korea to induce sedation. In our experience, the safety, effectiveness, and patient satisfaction with propofol administration by anesthesiologists were excellent.
In our case, the effects of the use of midazolam or ketamine did not differ for colonoscopy according to the procedure time; only the dose of propofol was increased for prolonged procedures. This was because propofol was used to maintain sedation after its induction. Because of this characteristic, low doses of midazolam were used for induction before administering propofol. This combination is widely used to relieve patient tension, increase the effectiveness of other drugs, and reduce side effects.26272829 As shown in the review by Yoon et al.,17 propofol is used for inducing sedation in EGD, but in colonoscopy, an additional propofol dose is required to maintain sedation during prolonged endoscopies.
In pediatric patients, recovery after anesthesia is influenced by various factors. It may also be affected by the type of examination or the usual anxiety, with the variations depending on the drug type, combination of drugs, and the dose of each drug.3031323334 In our study, recovery after sedation was expected to vary according to the drug type, such as midazolam, ketamine, and propofol, and their doses. We also expected it to vary depending on dose per body weight, obesity, and procedure time. However, it was difficult to assess all these variations because of the limitations of a retrospective study design and the small number of patients in each group. In the case of sedation performed by an anesthesiologist, since the midazolam doses were low during induction in all patients and propofol was used in more patients, recovery time was confirmed only based on the dose of propofol per body weight. Prolonged colonoscopies with a higher dose of propofol showed no correlation with recovery time. However, in EGD with a short endoscopy time and low propofol dose, simple cognitive parameters such as eye-opening, verbal response, and orientation differed significantly depending on the dose of propofol. The Aldrete score, which reflects overall sleep time and standard of discharge after sedation, was not associated with the propofol dose in EGD or colonoscopy. Our results demonstrate that increasing the propofol dose does not negatively impact the time of discharge.
Meanwhile, extensive investigations of propofol-related recovery in pediatric endoscopy are necessary. In particular, the results of a randomized double-blinded study on recovery time after MRI conducted by Schmitz et al.30 were similar to ours. Compared to that in the patient group that was sedated using relatively high doses of only propofol and that using ketamine with relatively low-dose propofol, the recovery time was shorter in the group sedated with low-dose propofol. In general, propofol affects the central nervous system via cerebral vasoconstriction, which is directly proportional to the administered dose.18 Cerebral blood flow and a decrease in metabolic demand for oxygen may be associated with the action of propofol.3536 Propofol was reported to affect the normal neurological functions, but its clinical significance is still unclear.18 Increasing sedation time through propofol use in children has been associated with prolonged sedation in premature infants or motor function reduction and blindness in 23-month-old infants.3738 These neurological effects and differences in recovery time are thought to be related, but further research is needed to confirm this finding. The effects and half-life of propofol differ according to age group and weight.18 Therefore, there is a risk of overdose in obese patients, and sedation may be insufficient if the dose is reduced.394041 In our study, recovery time was determined using dose per body weight according to the procedure time; however, additional prospective studies stratifying patients according to body weight or age group may provide further details on this issue.
This study had several limitations; first, it was not a prospective study that evaluated a specific drug, dose, or method of administration, but a retrospective study that analyzed medical records over the 5-year study period. Second, this study may reflect Korea's policies on the use of anesthetic drugs, internal hospital regulations, or personal preferences of anesthesiologists. Despite these few limitations, our study is the first report in Korea on sedation conducted by anesthesiologists in pediatric patients for endoscopy, which shows the various advantages of this approach. We suggest that during pediatric endoscopy, sedation should be performed by anesthesiologists in more centers and that drug combinations for sedation and recovery from sedation should be further investigated.
Go to :
 XML Download
XML Download