

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Although arthrodesis has been a favourable option for end stage ankle arthritis with its good clinical outcomes,123 concerns still exist about loss of motion and increased risk of adjacent joint arthritis.45 First-generation total ankle arthroplasty (TAA) used to end in failure due to high rates of loosening of implants and residual pain.6 Development of implant design and technologies with mobile bearing concepts as well as increased surgical skills have led to improved clinical outcomes of TAA.67 As a result, TAA has been emerging as an attractive option for end stage ankle arthritis in the last 20 years.89 Recent research reported that alternative use of TAA for ankle arthrodesis in the United States has increased from 3.1% in 1991 to 12.6% in 2010.5710
Although TAA has gained popularity worldwide, the complication rate of TAA is still higher compared to that of arthroplasties of the hip and knee joints.111213 The failure rate of TAA is reported to be about 10%–20% in the last 10 years.14 Knowledge about the epidemiology of primary TAA and rate of revision can aid not only patient counselling but also future development of TAA technology. Although recent literature reports trends of TAA and revision procedures in some countries,6151617 knowledge about TAA epidemiology still seems insufficient, especially in the Asian region.
Therefore, we investigated incidence of TAA procedures and revision in Korea. The aim of this study was to examine national surgical trends of primary TAA and revision procedures in Korea during the 11-year observation period using the national population-based data from the National Health Insurance Service (NHIS).
Go to : 
METHODS
Data source
People of Korea must enrol in the National Health Insurance (NHI) program. About 97% of the entire population has enrolled. Healthcare providers submit their patients' data to the Korean Health Insurance Review and Assessment Service (HIRA) to request reimbursement for medical costs from the NHIS. Seventy percent of medical costs are covered by the NHIS. The data submitted to the HIRA includes diagnosis coded according to the International Classification of Diseases, 10th revision (ICD-10); procedure codes; prescriptions; medical costs; and other demographic data. Most people (up to 3% of the total population) who did not enrol in the NHI program have healthcare insurance coverage by the Medical Aid Program. The claim data for reimbursement of medical costs of these patients are also submitted to the HIRA. Therefore, almost all medical records history in Korea are available in the HIRA. We analysed the national population-based data obtained from the HIRA from 2007 to 2017.
Data processing
The data of all patients who underwent TAA during the 11-year observation period from 2007 to 2017 in Korea were included. Specific procedure codes used for identification of TAA procedures are summarised in Table 1. For some procedure codes containing arthroplasties of the ankle, elbow, and wrist joints simultaneously (N0713, N0716), we included only cases with diagnosis code specific to the ankle joint pathology. Diagnosis for primary TAA was determined by filtering diagnosis codes specific to the ankle pathology defined by ICD-10. Annual primary TAA and revision procedure incidences, revision rates, and compound annual growth rate (CAGR) were obtained. The annual revision rate is the total number of revision procedures divided by total number of primary TAA within same year. The CAGR is used to estimate trends over time.1 It can be calculated using the following formula.
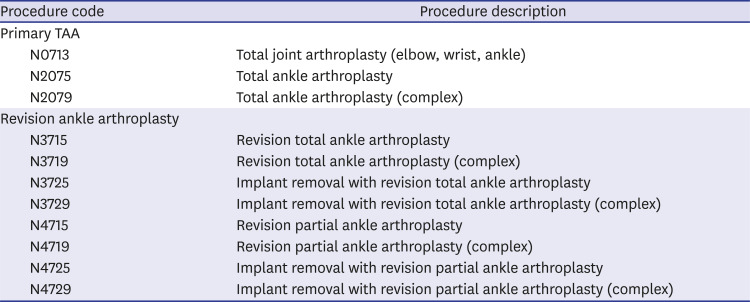
Table 1
Surgical procedure code for TAA in Korea
![]()

Incidence per 100,000 person-years was also calculated using epidemiologic data of each year from the “Statistics Korea” website (http://www.kosis.kr). All identified procedures were filtered according to age, gender, and hospital grades. Hospital grades were classified as follows in Korea: a “clinic” is a healthcare institution with less than 30 inpatient beds, a “hospital” has between 30 and 99 inpatient beds, a “general hospital” has more than 100 inpatient beds, and a “tertiary hospital” has a minimum of 20 specialised medical departments.18 The total hospitalisation cost was averaged, and the proportions paid by patient themselves and by the NHIS were identified.
Ethics statement
The Institutional Review Board (IRB) of the Hallym University Dongtan Sacred Heart Hospital approved the present study (HDT 2019-07-007). The IRB waived the need for informed consent because all the data used in the current study were anonymous.
Go to :
RESULTS
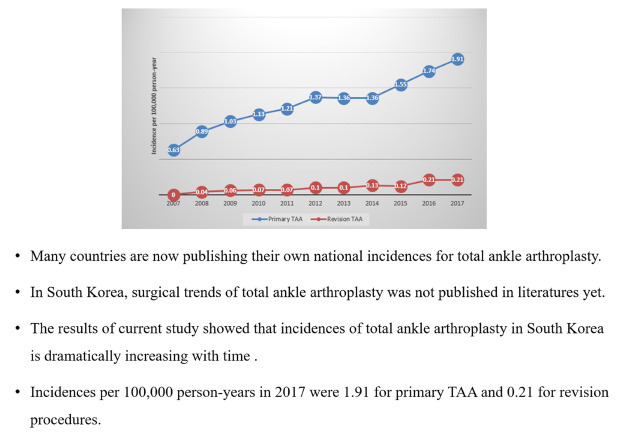
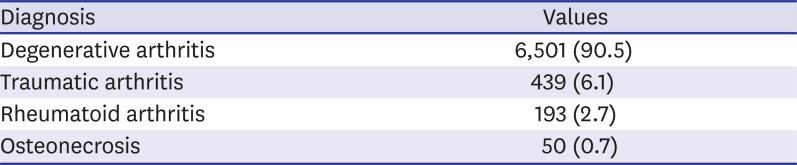
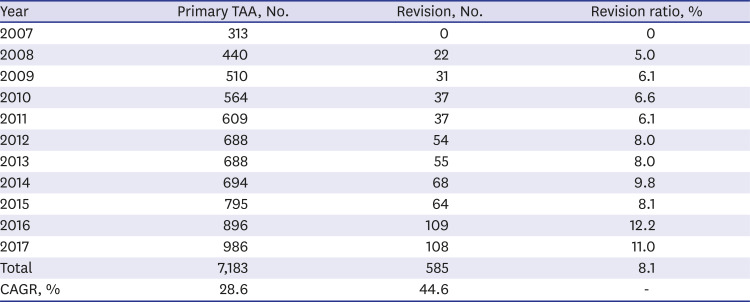
The causes of primary TAA are summarised in Table 2. Most diagnoses were of degenerative arthritis (6,501; 90.5%). Annual trends of primary TAA and revision procedures are summarised in Table 3. The number of primary TAA procedures in 2007 and 2017 were 313 and 986, respectively. The CAGR was 28.6% during the 11-year observation period. The number of revision procedures in 2007, 2008, and 2017 were 0, 22, and 108, respectively. The CAGR was 44.6% during the 10-year period (2008 to 2017). The period included in the CAGR calculation for revision procedures starts from 2008 because the number of cases in 2007 was zero. Revision rate also increased from 5.0% in 2008 to 11.0% in 2017. Annual incidences per 100,000 person-years are depicted in Fig. 1. Incidence of primary total ankle procedures was 0.63 per 100,000 persons in 2007; it increased to 1.91 per 100,000 persons in 2017. Incidence of revision procedures was 0 in 2007 and increased to 0.21 per 100,000 persons in 2017.
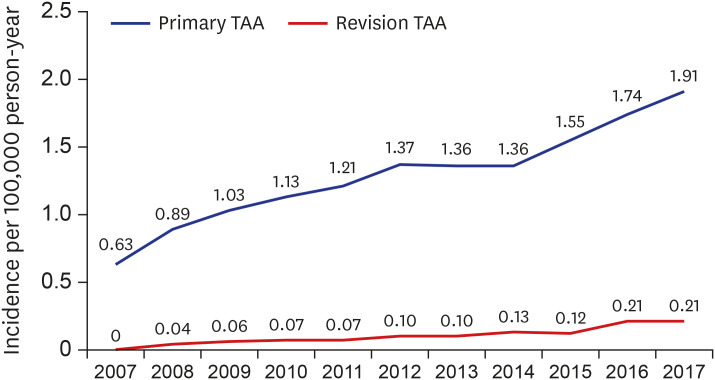 | Fig. 1Annual incidences per 100,000 person-years of primary TAA and revision procedures.TAA = total ankle arthroplasty.
|
Table 2
Causes of primary total ankle arthroplasty
| Diagnosis | Values |
|---|---|
| Degenerative arthritis | 6,501 (90.5) |
| Traumatic arthritis | 439 (6.1) |
| Rheumatoid arthritis | 193 (2.7) |
| Osteonecrosis | 50 (0.7) |
![]()
Table 3
Annual trends of primary TAA and revision procedures
![]()
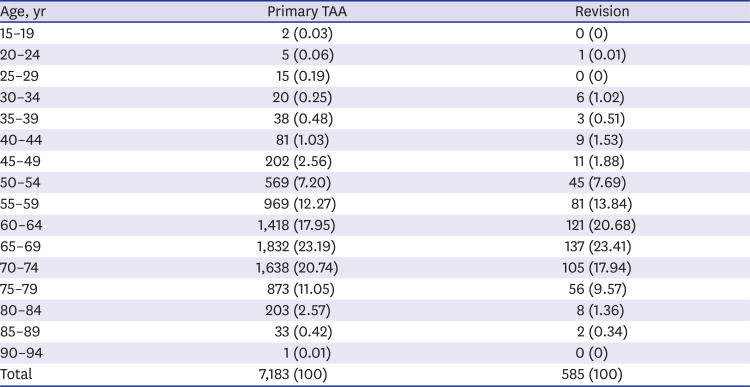
The age distribution of patients with primary TAA and revision procedures is listed in Table 4. A total of 92.4% and 93.2% procedures were distributed over the age range of 50 to 79 years for primary TAA and revision arthroplasty, respectively. Surgical trends according to gender are listed in Table 5. Men have a greater incidence of primary TAA (52.35% vs. 47.65%). Women have a greater incidence of revision (52.08% vs. 47.92%). The proportion of hospital grades where primary TAA and revision procedures were performed are depicted in Fig. 2. The primary TAA procedures were most often performed by “hospital” grade health providers, however, revision procedures were most frequently performed in tertiary hospitals. Patterns of insurance coverage are depicted in Fig. 3. The average total hospitalisation cost for one primary TAA was USD 4,293. The average cost paid by patients themselves was USD 813.0 and the average cost paid by the NHIS was USD 3,480.3. Most (92%) of the insurance coverage was provided by the NHIS.
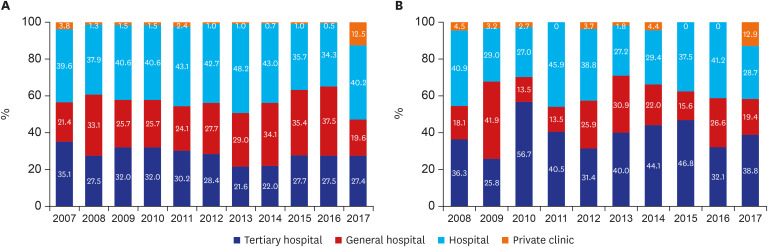 | Fig. 2Annual surgical proportions (in percentages) according to hospital grades. (A) Primary total ankle arthroplasty. (B) Revision procedures.
|
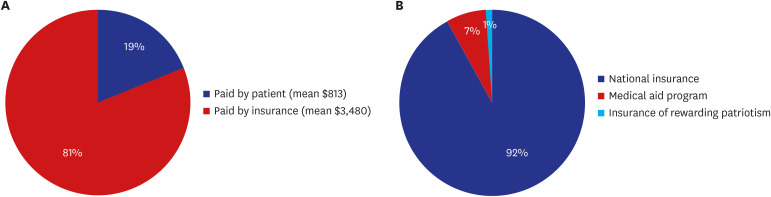 | Fig. 3Total cost per primary total ankle arthroplasty, and insurance coverage pattern. (A) Percentage of average cost paid by patients. (B) Percentage of insurance coverage types.
|
Table 4
Surgical trends of primary TAA and revision procedures according to age
![]()

Go to :
DISCUSSION
This is the second population-based study of surgical trends of TAA procedures in an Asian country. The current study concludes that TAA procedures have steadily increased over the years in Korea. Surgical incidence per 100,000 persons was 1.91 in Korea in 2017, which is much higher than that in Japan. Incidence of TAA in Japan was 0.2 procedures per 100,000 persons in 2013.6 It is about seven fold lower compared to the incidence in Korea in 2013 (1.36 TAA per 100,000 persons). Matsumoto et al.6 noted that most hospitals in Japan perform less than 5 cases of TAA annually, and the dispersion of a low number of TAA procedures over several hospitals seems to make the research of clinical outcomes difficult. They insisted that this may be the one reason for the slow growth of TAA procedures in Japan. In addition, they noted that limited number of available designs of TAA in the Japanese market is another reason for slow growth of TAA. They described that there are only two available designs of TAA in Japan; the TNK ankle (Kyocera Medical, Osaka, Japan) and the FINE ankle system (Teijin Nakashima Medical, Okayama, Japan).6
Incidence of TAA in Korea is comparable to Western countries. Incidence of TAA in Sweden, Norway, and the United Kingdom was reported to be about 1 per 100,000 persons.6 Incidence of TAA procedures in Germany was reported to be about 2 per 100,000 persons,612 and of United states was 1.9 to 4.0 per 100,00 persons.819
Low burden of surgical cost for patients in Korea seems to play a role in the relatively high surgical incidence in Korea. The current study reveals that patients paid only an average of $813 for one TAA surgical procedure. The remaining average of $3,480 was paid by the NHI system, under which 92% of the patients are covered.
Surgical incidence for revision procedures also have been steadily rising in Korea. Incidence per 100,000 persons for revision procedures in 2008 was 0.04; it increased in 2017 to 0.21, approximately five fold the incidence in 2008. Ratio of revision to primary TAA procedures were 12.2% and 11.0% in 2016 and 2017, respectively, in Korea. It corroborates the results of previous research, which state a revision rate of 16.0% to 19.93%.120 Revision ankle arthroplasty is a complex procedure with longer operative time, and previous literature noted that it has 6.4 fold more risk to develop deep surgical site infection compared to primary procedure.721 Moreover, failed TAA procedures can lead to serious consequences, including even below the knee amputation.2223 Surgeons who perform primary TAA procedures should keep in mind the revision incidence and revision burden of TAA.
The current study has limitations. First, like other population-based research, an inaccurate code for diagnosis can result in a bias in primary diagnosis for TAA procedures. However, we used specific procedure codes for detecting surgical incidences. In virtue of a relatively simple code system for each procedure, it seems that surgical trends of TAA investigated in the current study may have a low risk of under-or over-estimation of surgical incidences. Second, health insurance data did not contain preoperative severity and type of implant used for the procedure. We were only able to detect surgical incidences. For providing more insights into revision procedures, detailed data including pre- and post-surgical functional outcome, implant type, and radiological finding are needed. Despite these limitations, a large cohort of population-based research can reveal generalised trends for TAA. Currently, application of big data science is growing in various aspects of our life. In the future, big data in medicine may allow inclusion of more detailed data of patients. Third, we did not perform statistical comparison because this data is not a sample but a whole population. Another reason for not performing statistical analysis was that, due to the large sample size, it surely has high statistical significance.
In conclusion, incidences of primary TAA and revision procedures in Korea have been growing quickly during the past 11 years. Due to the possible serious consequences of revision procedures of TAA, surgeons should always consider revision rate of primary TAA procedures.
Go to :
 XML Download
XML Download