

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Physician home visits were widespread in the western history of medicine until the 19th century and then declined sharply with the formation of a hospital-oriented medical system in the mid-20th century. Over the last 30 years, Aging in Place has been emphasized due to population aging and rising medical expenditures among older adults, and home-based primary care has also started to gain attention.123 Various attempts have been made to develop a home care service with the discussion on primary health care reform for the older population. For example, preventive home visit programs have received much attention in the past two decades and become part of national policy in several countries, such as Denmark, Japan and Australia.4 Comprehensive preventive home visits have the potential to reduce the disability burden among older adults when based on multidimensional assessment with clinical examination567 and a biobehavioral/environmental approach.8 By contrast, trials in the Netherlands and the UK in the 1990s showed that home visits did not seem to be useful for the general population of older people. The United Kingdom withdrew this pilot program in 2004 based on the results of a large national trial.49 In their editorial, Stuck and Kane10 indicated that older persons at higher risk or those already disabled are likely to benefit from only ‘multidisciplinary interventions’ that target ‘specific problems.’1112 But still, the economic arguments for these programs, such as cost-effectiveness, remained to be corroborated.
In recent years, there has been an opinion that Korea needs to establish an alternative medical model based on the community, including a primary geriatric physician system and home-based primary care for homebound older adults with increasing concerns about frailty.13141516 The Korean government recently announced the Community Care Policy in 2018, which includes: 1) strengthening community-based health care services, 2) ensuring health rights for vulnerable groups, 3) setting up a discharge pathway from hospital to returning home, and 4) building a community-based public-private partnership system. The role of primary care physicians in community care is to organize and coordinate various outpatient and home care services. An outpatient-oriented medical practice cannot successfully manage chronic diseases without home-based primary care, which enables continuous observation and monitoring of patients, especially for homebound older adults. According to Kim and Jang,15 at least 600,000 older adults (about 10% of the entire population aged 65 and over) were estimated to be homebound, not being able to go freely outside to use local outpatient clinics in Korea. These adults are the medically isolated people who are obviously excluded from the primary care system unless physician home visits are available in their hometown. Along this line, Lee17 stimulated the vision and rhetoric to Korean primary physicians, “Now it's time to see the community - outside the clinic.” However, compared to these social demands, there are only a handful of studies on physician home visits17 and particularly little research on the valuation and willingness to pay (WTP) from the perspective of the older population.
The process of selecting medical services for users consists of several steps, such as problem recognition, information search, evaluation of alternatives, choice of medical institutions, and post-use behavior.18 This process cannot necessarily be done rationally. Various criteria can be applied according to the subjective viewpoint of medical users. To enhance medical consumers' satisfaction, efforts to provide desired services based on empirical data from the perspective of consumers should be a basic and core strategy.19 In addition, the cost of physician home visits, that is, who pays for them and how much they cost, is essential for achieving feasibility and quality of service.20 WTP is a contingent valuation method that is commonly used to assess how patients value the personal utility of new healthcare technologies and services. WTP assesses the maximum amount of money an individual would pay for the health intervention and still consider him/herself better off.21
In order to advance beyond the descriptive commentary on why patients need physician home visits, we aimed to conduct a nation-wide opinion survey from the perspective of consumers. Our aim was to determine the need and WTP for physician home visits among the community-dwelling older population in Korea. Our second aim was to examine the hypothesis concerning the most important factors that influence older adults to make the choice to use a physician home visit service. Through the above analyses, our intention was to gain knowledge on which subgroup of older people needs physician home visits the most. Before outlining and testing the analytic model, we briefly discuss the hypothesis of the study.
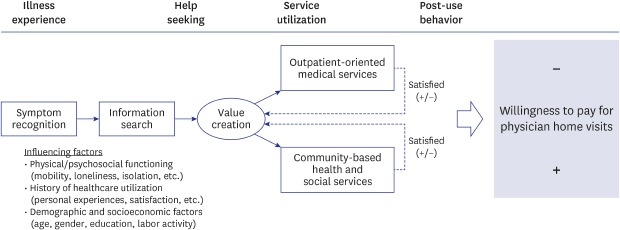
What is the process through which people make a choice to pay for a physician home visit service? In the present study, we developed a theoretical model of the WTP for physician home visits based on a literature review of medical sociology and service marketing.15181920 According to Fig. 1, the process is comprised of four stages: illness experience, help seeking, service utilization, and post-use behavior. An individual who gets sick will make a choice as to which type of service is more appropriate to relieve his or her symptoms through information gathering. This process might be influenced by a variety of factors, which include not only the current health problem (e.g., physical and psychosocial functioning) but also past experiences of healthcare service utilization (e.g., personal judgement, satisfaction). During the process, the value of physician home visits will be created personally. Finally, the individual will choose one of two types of healthcare services: 1) outpatient-oriented medical services or 2) community-based health and social services. Behavior after the selection will also affect the process of valuation. For example, the less the individual is satisfied with the use of outpatient-oriented medical services, the more the individual will prefer to use community-based health and social services.
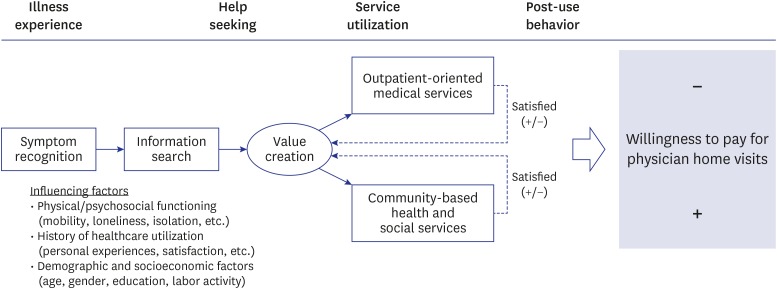
Based on the theoretical process, the hypothesis of this study can be summarized as follows:
H1. The lower the individual's physical or psychosocial functioning, the higher the individual will valuate physician home visits.
H2.1. The less the individual is satisfied with the use of outpatient-oriented medical services, the higher the individual will valuate physician home visits.
H2.2. The more the individual is satisfied with the use of community-based health and social services, the higher the individual will valuate physician home visits.
METHODS
Study participants and survey
A total of 800 people aged 60 years or older were selected nationwide using a multi-stage stratified random sampling method in consideration of the distribution of gender, age and five wide residential areas including Seoul, Gyeonggi, Yeongnam, Honam, and Gangwon. Gender distribution were assigned to include men and women evenly. Age distribution were applied in accordance to the national age distribution by 10 years from 60 years old to 90 years old or over. As for the residential area, sampling was distributed evenly by five regions. The researchers trained interviewers on the questionnaires before the survey. Voluntary face-to-face direct interviews were conducted with older adults living in the community who were able to communicate without cognitive distortion and/or hearing loss and able to understand the purpose of this study. Participants with missing data were excluded; the resulting study population consisted of 797 participants.
Measurements
The outcome variable was the value for physician home visits, which was measured using two methods. First, the need for physician home visits was measured using the following question: “Do you want a doctor's home visiting service when you need help?” Second, WTP for physician home visits was measured using one open question measured in Korean won (KRW): “For a doctor's home visit, what is the appropriate amount per visit that you could pay?”
Independent variables were categorized into two groups: 1) health-related factors and 2) service utilization factors. For health-related factors, variables of EuroQol-five dimensions (EQ-5D), number of falls, and subjective loneliness were measured to assess physical and psychosocial functioning, respectively. The EQ-5D is comprised of the following five dimensions: mobility; self-care; usual activities; pain/discomfort; and anxiety/depression. The results were summed to produce a global score ranging from 5 (best) to 15 (worst). The number of falls was also reported by participants to assess physical functioning based on their experience during the past year. We assessed psychosocial functioning as subjective loneliness (scored from 1 to 3). To assess service utilization, current experiences concerning outpatient-oriented medical services and community-based health and social services were measured. In this study, we supposed that currently available community-based health and social services in Korea included the following components: 1) National Preventive Home Visits (NPHV, provided by visiting nurses from a public health center); 2) Advanced Home Care Service (AHCS, provided by nurse practitioners from a general hospital); 3) Home Helper Visiting Service (HHVS, provided by home helpers financed by the Long Term Care Insurance); 4) Senior Health Promotion Program (SHPP, provided by a social welfare center or Gyeong-ro-dang); and 5) community service provided by a public health center. We regarded an outpatient-oriented medical service as equal to service from a local private clinic. All of the experiences of utilization were dichotomized, and satisfaction was scored on a Likert scale ranging from 1 to 5.
Information regarding demographic and socioeconomic status included gender, age, educational level, residential area, family size, marital status, social participation, household income, and occupational status (i.e., salary earners, self-employed or other jobs, out of work). Using information on household income and family size, the categorical variable of absolute poverty, indicating people living beneath the minimum cost of living, was formulated.
Statistical analysis
A statistical summary was first used to characterize study participants. The logit model for regression was used to analyze the association between the need for physician home visits (dichotomized variable) and each of the independent variables. Lastly, the Tobit model was used in order to identify the association between WTP (censored continuous variable) and the independent variables. In the present study, 61.5% of the study participants reported that they valuated physician home visits at zero KRW. This is the classic example of censoring, which Tobin22 referred to in his study of household expenditures. It is reasonable to assume that dependent variables are censored to zero, because no one would easily suppose that a medical doctor would come to one's house if he or she could not pay a certain minimum amount (e.g., 10,000 KRW). In this case, he or she may respond with zero instead of reporting an exact value. The Tobit model has an advantage in that it can estimate the coefficient with less bias without loss of sample by assuming a censored normal distribution. All analyses were adjusted for gender, age, family size, residential area, educational level, marital status, social participation, household income (log transferred), poverty status, and occupational status. A P value less than 0.05 from two-sided tests was considered statistically significant. All analyses were conducted by Stata 15.
RESULTS
The general characteristics of the study participants are described in Table 1. The mean age was 70.6 (standard deviation 7.5). Most participants were residing in an urban area (77.2%), and almost half of them did not participate in a labor activity (53.0%). About 25.6% of participants reported that their monthly household income was below the absolute poverty line. The mean and standard deviation of the EQ-5D score were 6.2 ± 1.6. Satisfaction related to using a local private clinic and public health center were recorded as 3.9 ± 0.5 and 3.7 ± 0.6, respectively.
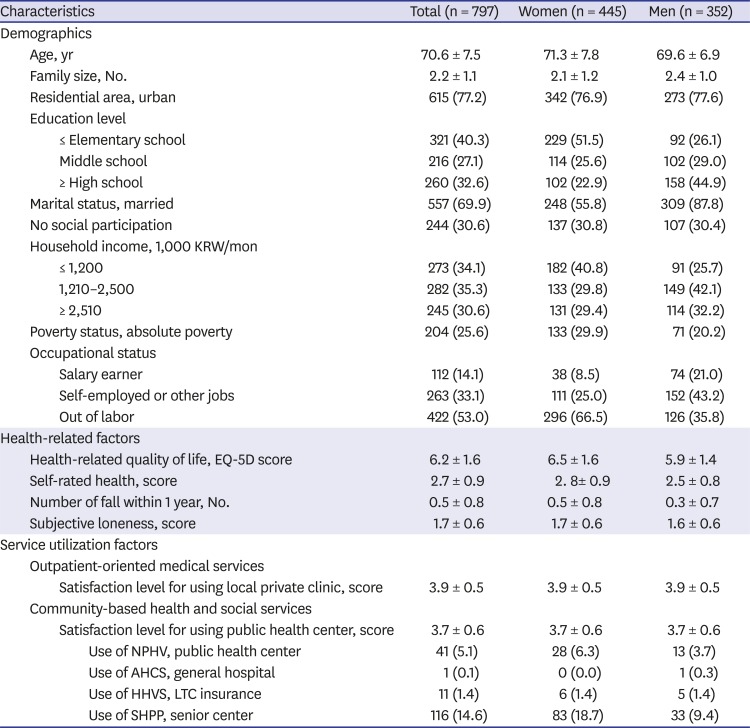
Table 1
General characteristics of the study participants
Data are presented as mean ± standard deviation or number of case (%).
KRW = Korean Won, EQ-5D = EuroQol-five dimensions, NPHV = national preventive home visits provided by visiting nurses from public health center, AHCS = advanced home care service provided by nurse practitioners from general hospital, HHVS = home helper visiting service provided by home helpers financed from the long-term care insurance, LTC = long-term care, SHPP = senior health promotion program provided by social welfare center or Gyeong-ro-dang.
P values were calculated by χ2 test, Fisher's exact test, and independent t-test.
Total sum of scores are listed as follows: EQ-5D (15), self-rated health (5), subjective loneliness (3), satisfaction of local private clinic (5), satisfaction of public health center (5).
![]()
Table 2 shows the results of the valuation of physician home visits according to general characteristics. Three hundred and thirteen participants (39.3%) reported that they wanted a physician's home visit when they needed help. Among all study participants, the WTP amount for physician home visits was 8,683 ± 15,395 KRW. When we restricted the sample only for the subgroup of participants who reported that they needed a physician home visit service (n = 313), the mean and standard deviation of WTP was 21,982 ± 17,546 KRW. Table 2 also describes the group differences in value for physician home visits. Older adults who had an occupational status of out of labor or self-employed (P = 0.042) were more likely to need a home visit service than others. Those who were satisfied with a public health center (P = 0.046) were also more likely to need a home visit service compared with their counterparts. A younger age, below 75 years old (P = 0.030), higher educational level (P = 0.002), married status (P = 0.007), social participation (P = 0.018), and self-employed or out of labor as occupational status (P= 0 .036) were also found to be significant factors associated with higher WTP for physician home visits. One thing to note is that only a weak correlation was observed between household income and WTP for physician home visits (Pearson's correlation coefficient, r = 0.053, n = 797), even though we analyzed the poor (r = 0.094, n = 204) and the non-poor (r = 0.021, n = 593) separately (Supplementary Fig. 1). This means that a physician home visit service is a kind of common necessity good that has an income elasticity of demand between 0 and 1.
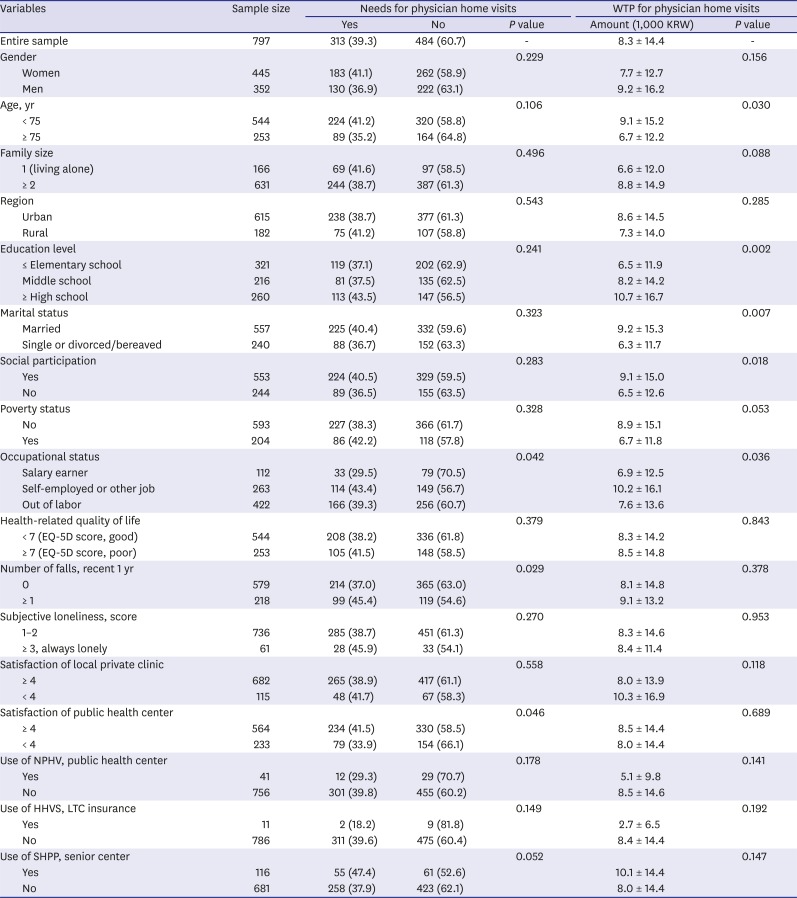
Table 2
Needs and WTP for physician home visits
Data are presented as mean ± standard deviation or number of cases (%).
WTP = willingness to pay, KRW = Korean Won, EQ-5D = EuroQol-five dimensions, NPHV = national preventive home visits, HHVS = home helper visiting service, LTC = long-term care, SHPP = senior health promotion program.
P values were calculated by χ2 test, Fisher's exact test, independent t-test, and one-way ANOVA.
![]()
Table 3 provides results from the logit and Tobit regression models to show the most important factors that affect the valuation of physician home visits. To verify the first and second hypothesis of this study, we input both variables of health-related factors (H1) and service utilization factors (H2) into the regression model. Out of three health-related factors, only health-related quality of life (i.e., EQ-5D score) was significantly associated with the need for a physician home visit service (odds ratio [OR], 1.13; 95% confidence interval [CI], 1.01–1.27; P = 0.035), but not with WTP in the Tobit model. Out of five service utilization factors, the satisfaction level with a public health center (OR, 1.32; 95% CI, 1.02–1.72; P = 0.034) and current use of SHPP provided from a social welfare center or Gyeong-ro-dang (OR, 1.61; 95% CI, 1.04–2.50; P = 0.033) were associated with a higher need for physician home visits. However, for the Tobit model, only SHHP utilization was found to significantly increase WTP for physician home visits (beta coefficient [β], 8.39; standard error [SE], 3.63; P = 0.021). This finding means that persons who are currently using a community-based social service tend to pay 8,390 KRW more than those who are not using the service to purchase doctor home visits. Among the general characteristics, only higher educational status (i.e., above high school graduation) was significantly associated with an increased need (OR, 1.67; 95% CI, 1.05–2.67; P = 0.030) and WTP for physician home visits (β, 8.49; SE, 3.86; P = 0.028).
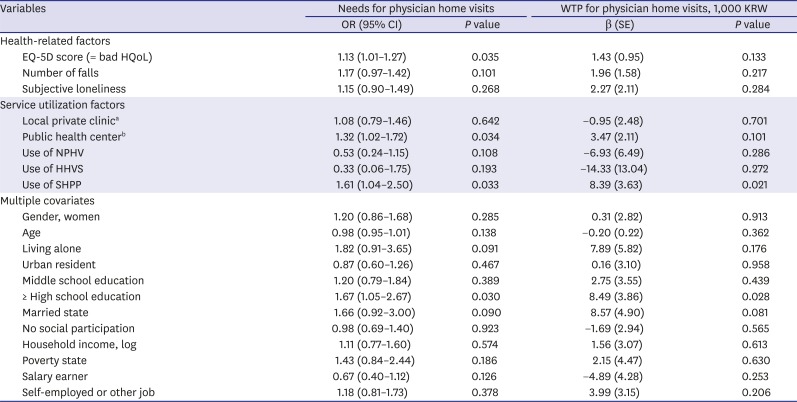
Table 3
Influencing factors associated with preference for physician home visits among Korean older population (n = 797)
WTP = willingness to pay, KRW = Korean Won, OR = odds ratio, CI = confidence interval, β = beta coefficient, SE = standard error, EQ-5D = EuroQol-five dimensions, HQoL = health-related quality of life, NPHV = national preventive home visits service, HHVS = home helper visiting service, SHPP = senior health promotion program.
aLocal private clinic: satisfaction score of using local private clinic; bPublic health center: satisfaction score of using public health center.
![]()
Tables 4 and 5 provide the results of the subgroup analyses, which show a moderate effect of gender and satisfaction level with using an outpatient-oriented medical service in Korea. Among female older adults (n = 445), health-related factors such as the EQ-5D score (OR, 1.21; 95% CI, 1.04–1.41; P = 0.015; β, 2.26; SE, 1.02; P = 0.028) and number of falls (OR, 1.41; 95% CI, 1.09–1.80; P = 0.008; β, 4.15; SE, 1.68; P = 0.014) were identified as significant factors associated with an increasing need and WTP for physician home visits. This means, for example, as the number of falls increased by one unit, the value of physician home visits generally increased 4,150 KRW among female older adults. When we restricted the study participants who were not satisfied with using a local private clinic (n = 115), the only factors that affected the need for physician home visits were identified as health-related factors, such as the number of falls (OR, 2.22; 95% CI, 1.08–4.57; P = 0.031) and subjective loneliness (OR, 3.19; 95% CI, 1.32–7.70; P = 0.010). Among the subgroup of non-satisfied, as the level of subjective loneliness increased by one unit (i.e., from not at all to sometimes, or from sometimes to always), WTP for physician home visits generally increased 17,520 KRW. Among this subgroup population, no other influencing factors reached significance at the 0.05 level. This indicates that valuation process for physician home visits among older adults is based upon the complex interaction between health-related factors, service utilization factors, and general characteristics of the population.
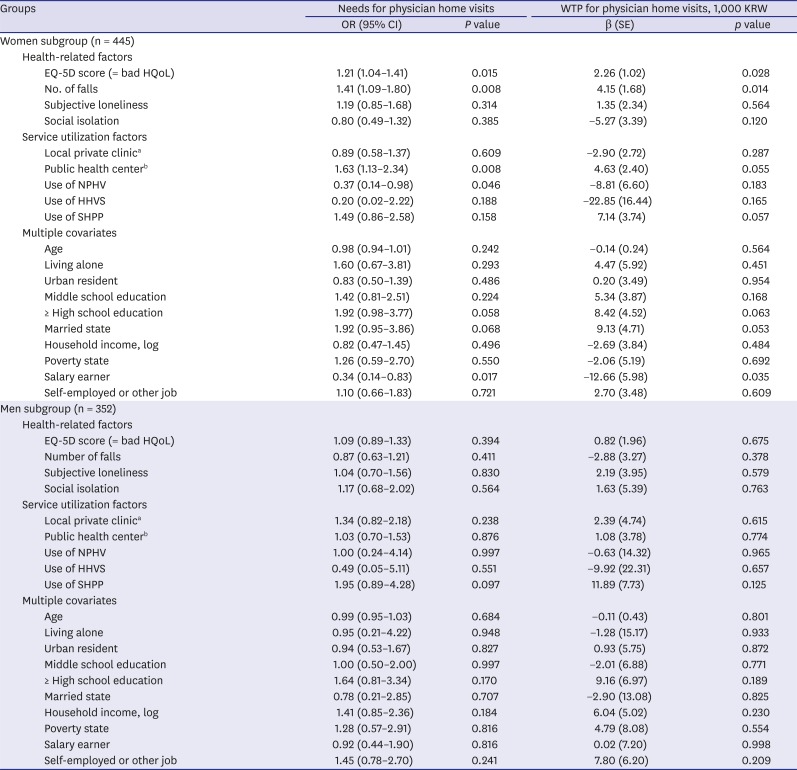
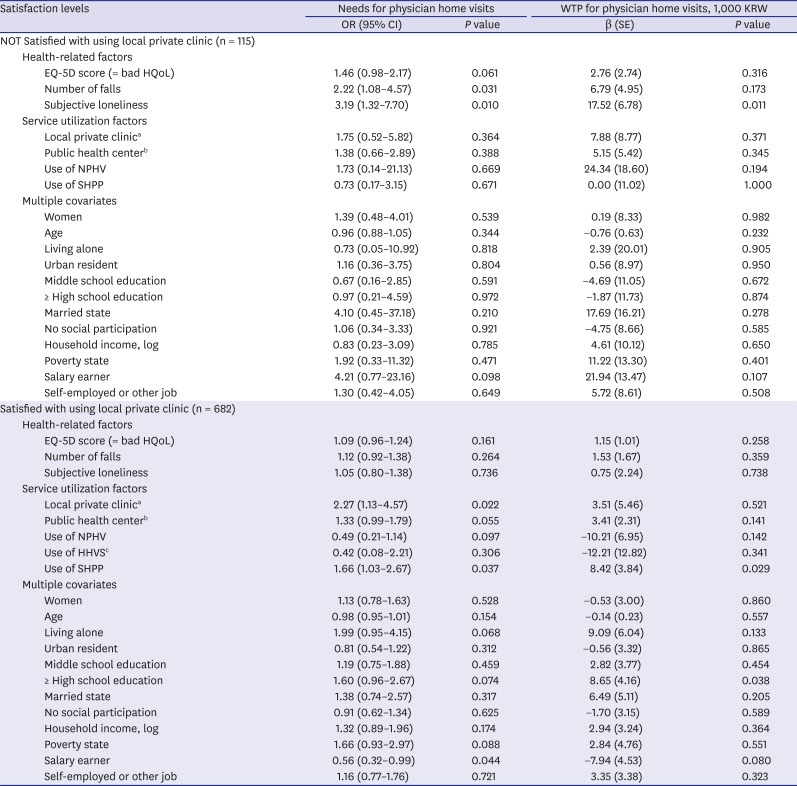
Table 4
Influencing factors associated with preference for physician home visits among subgroup participants along with gender
WTP = willingness to pay, KRW = Korean Won, OR = odds ratio, CI = confidence interval, β = beta coefficient, SE = standard error, EQ-5D = EuroQol-five dimensions, HQoL = health-related quality of life, NPHV = national preventive home visits service, HHVS = home helper visiting service, SHPP = senior health promotion program.
aLocal private clinic: satisfaction score of using local private clinic; bPublic health center: satisfaction score of using public health center.
![]()
Table 5
Influencing factors associated with preference for physician home visits among subgroup participants along with satisfaction level for using local private clinic
WTP = willingness to pay, KRW = Korean Won, OR = odds ratio, CI = confidence interval, β = beta coefficient, SE = standard error, EQ-5D = EuroQol-five dimensions, HQoL = health-related quality of life; NPHV = national preventive home visits service, SHPP = senior health promotion program, HHVS = home helper visiting service.
aLocal private clinic: satisfaction score of using local private clinic; bPublic health center: satisfaction score of using public health center; cVariable of ‘use of HHVS’ was omitted due to perfect collinearity.
![]()
DISCUSSION
This study aimed to estimate the proportion of the Korean older population who needed physician home visits and suggest influencing factors associated with the value of physician home visits. Overall, about 40% of older adults reported that they needed physician home visits. Those who were in need of physician home visits also reported that they were able to afford the service and willing to pay an average of 22,000 KRW per doctor's home visit. In this study, we also examined the most important factors that influenced older adults to decide to use a physician home visit service. Results showed that a higher valuated need for physician home visits was associated with an individual with a lower level of physical/psychosocial functioning (e.g., EQ-5D) and a higher level of satisfaction with using community-based health and social services (e.g., public health center, social welfare center or Gyeong-ro-dang).
To the best of our knowledge, no previous studies have published the results of a population survey concerning WTP for physician home visits in Korea. Currently, there is a heated debate about the fee for physician home visits under the Community Care Policy in Korea. In December 2018, for the first time in Korean history, legal foundations for physician home visits were established. According to the revised version of the National Health Insurance Act (41-5), a medical doctor can now conduct medical treatment in a patient's home (i.e., outside the clinic) if the patient has a condition (illness or injury) making it uncomfortable to move outside the house. These changes were announced in June 2019, and debates about how much the insurer (the National Health Insurance) should pay to physicians for home visits are being seriously discussed between the government and medical associations. With this background, this study emphasized that the fee for physician home visits should be valuated based on the empirical data of WTP, which comes from a consumer-centered perspective. According to the survey of the Korean older population in our research, the total fee for a physician home visit service could be set as high as 73,000–220,000 KRW, if we assume the copayment ratio (i.e., out-of-pocket payment share of the total fee for the service) is set as 10%–30%. This is a somewhat higher payment than the fee for a physician home visit set in the Primary Care Service for Disabilities (73,850 KRW, 10% copayment) and Home-based Hospice-Palliative Care Service (83,870 KRW, 20% copayment), which are currently being implemented.
This study is also significant in that it suggests a theoretical model of value creation for physician home visits. From the consumer-centered perspective, we assume that each individual develops a personal valuation system as cognitive processes that guide his or her choice decisions among various health-related service providers. In Korea, there are broadly two different settings of healthcare services: 1) outpatient-oriented medical services and 2) community-based health and social services. Value negotiation will occur as to which type of service is the most appropriate to relieve a patient's symptoms with consideration of the individual's physical and psychosocial functioning, personal experiences of service utilization, and basic demographic factors. This study provides evidence that choice decisions to pay for physician home visits are based upon complex interaction among these factors. The majority of participants (approximately 60%) did not report the necessity for physician home visit care. It is possible that older adults in need of physician home visits included home-bound elderly who are more likely to be vulnerable in terms of health status and economic condition. According to the previous study,15 the prevalence of homebound older adults is estimated as 30.1%. In addition, the value-creating process of physician home visits can be influenced by past experiences of healthcare service utilization. Most of the elderly had little experience in physician home visiting in Korea, thus it would be difficult to respond positively to the need for visiting care.
On the basis of the empirical analyses, two subgroups of older adults were identified as most in need of physician home visits: 1) female older adults who have limited physical functioning and 2) older adults who feel loneliness and are not satisfied with using medical services in a local private clinic. These results have some implications. First, a gender difference was noticed in the valuation process of physician home visit services. Compared with men, older women in Korea were willing to pay for physician home visits when they encountered problems with physical functioning (e.g., recurrent falls). Perhaps this kind of difference may be a feature of Korean society with gender inequality in caring roles under the patriarchal tradition.23
Second, psychosocial functioning, such as subjective loneliness, also affected the value-creating process of physician home visits. A previous study conducted in the Netherlands reported that preventive home visiting improved metal health rather than physical health. These results are consistent with previous studies that suggested that services in the home care setting should be provided with an interdisciplinary team.524 To be called home-based primary care, one of the alternatives to primary care in several countries, a physician should provide comprehensive and continuous healthcare services through interdisciplinary teams at a patient's home.152425
Third, community-based social services may contribute to expanding a new healthcare market for physician home visits. Interestingly, in this study, using healthcare services from a social welfare center or Gyeong-ro-dang was analyzed as the most significant factor that increased both the need and WTP for physician home visits. Maybe the learning effect of Aging in Place and Community Care Policy has worked. From the viewpoint of community-dwelling older adults, various types of community-based services may promote the value of physician home visits. This implies that community-based social services are not just a competitive substitute for outpatient-oriented medical services, but a cooperative complement that play a significant role in expanding the healthcare market into new areas. For example, the metropolitan government of Seoul initiated the ‘Chat-Dong,’ and ‘Seoul-Care’ recently.15 Chat-Dong is the universal home visit program by nurses and social workers for older adults aged 65 and 70 years old. ‘Seoul-Care’ is the integrated chronic disease management program by multidisciplinary teams including physicians, nurses, social workers, nutritionists, and athlete trainers working in the public health center. Similar programs have been started inside Community Care Program to several regions in Korea from 2018. Connecting subjects and collaborating services with these community based social services can be both a benefit and an advantage for the physician home visit care.
This study has some methodological limitations. First, although the research design of this study helps identify general characteristics of people who are most in need of physician home visits, it is difficult to make causal inferences using a cross-sectional study. Second, not all confounding factors that affected the results were included in the analyses. For example, we were unable to measure variables concerning chronic disease or comorbidity. If we assume that the number of chronic diseases has a positive correlation with WTP for physician home visits, as is generally supposed, the results of our study would be overestimated by omitting that variable. Third, the results have limited generalizability due to the relatively small sample size. For example, the generalizability of the results to persons who are beneficiaries of the National Long-Term Care Service or persons with a homebound status is unknown. Although we used nationwide survey data selected by a multi-stage stratified random sampling method, further surveys with participants of a different age, functional status, and medical condition are needed to generalize the results of the study.
In conclusion, about 30% of community dwelling older adults reported that they need physician home visit services. And we can expect that consumer power might be stronger than the Korean government has acknowledged because patients' WTP was somewhat higher than the fee for physician home visits set in the Primary Care Service for Disabilities. The decision to pay for physician home visits is based upon the complex interactions among an individual's physical and psychosocial functioning, personal experiences of service utilization, and demographic factors. The value for physician home visits should be qualified based on the WTP empirical data, which comes from a consumer-centered perspective.
 XML Download
XML Download