

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Patients with idiopathic growth hormone deficiency (GHD) have been treated with DNA-derived recombinant human growth hormone (rhGH) since 1985.1 In Korea, rhGH has been approved for administration to patients with idiopathic GHD since 1999. Currently, the diagnosis and treatment of GHD in childhood and adolescence follows consensus guidelines of the growth hormone (GH) Research Society.2 The first-year response of GH therapy seems to be the most important factor in determining the overall success of GH treatment.3 It does not predict the final outcome, but a good initial response is encouraging for further treatment.
Many publications have been conducted to predict the growth response to GH therapy and to figure out the affecting factors to GH responses. Some studies have reported that birth weight, mid-parental height (MPH), bone age and height at the start of GH treatment are important factors for successful outcome of GH treatment in children with idiopathic GHD.4 Other reports also suggested that the characteristics of patients including birth weight, severity of GH deficiency, GH dose, serum insulin-like growth factor-1 (IGF-I) level and weight at start of GH treatment were found to be correlated with the efficacy of GH therapy.56 However, these results are based on small subject number and cross sectional data.
The application of the growth prediction model is the attempt to be more tailored and personalized during GH treatment. In particular, Ranke et al.7 proposed a “data-driven” approach based on the quantitative analysis of a large cohort of patients in the KIGS database (Pfizer International Growth Database; Pfizer Health AB, Strangnas, Sweden) to make growth prediction model. The LG Growth Study (LGS) is a long-term observational cohort study and non-interventional registry evaluating the long-term safety and effectiveness of rhGH, Eutropin® inj., Eutropin AQ® inj. (LG Chem, Seoul, Korea) in Korean children.8 There is no predictive model of the first year response to GH treatment in prepubertal Korean children with idiopathic GHD. We developed a predicting model to estimate the first year growth response to a GH treatment in prepubertal idiopathic GHD children using a ‘data-driven’ approach by Ranke and LGS database.
Go to : 
METHODS
Selection of the study population
LGS is a multi-center (total 73 sites), noninterventional registry study approved by the Ethics Committees of the participating institutions.9 There were 783 patients aged from 2 years to 10 years old who were diagnosed with idiopathic GHD and who had received rhGH between September 2011 and December 2017. The diagnosis of idiopathic GHD was made by the physician according to the LGS etiology classification, as defined by maximum GH levels less than 10 ng/mL in at least two GH stimulation tests. Children with pituitary or hypothalamic lesions were excluded. The subjects had been treated with rhGH for at least 1 year and who remained prepubertal (defined as a testicular volume of less than 4 mL in boys or Tanner breast stage 1 in girls) during treatment. Among the 783 participants, subjects who had received once weekly rhGH injection (n = 115), and/or those with inappropriate auxological data (n = 323) were excluded. Ultimately, our study population included 345 children (195 males and 150 females) (Fig. 1) (Table 1).
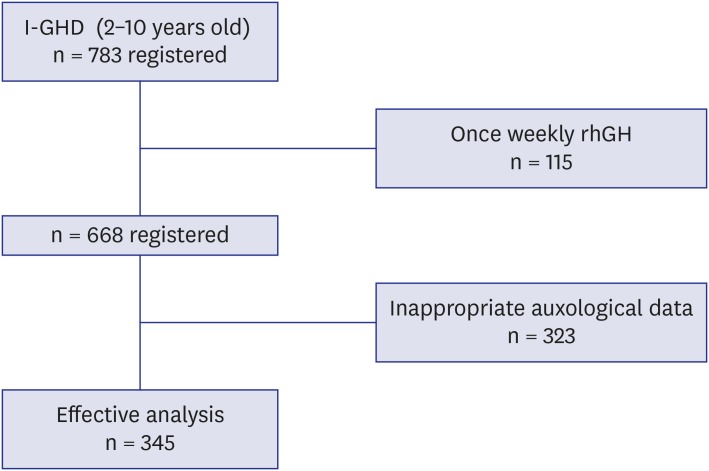 | Fig. 1A flow chart of cohort. Among the 783 participants, subjects who had received once weekly rhGH injection (n = 115), and/or those with inappropriate auxological data (n = 323) at 12 ± 3 months after GH treatment were excluded. Ultimately, our study population included 345 children (195 males and 150 females).GHD = growth hormone deficiency, rhGH = recombinant human growth hormone.
|
Table 1
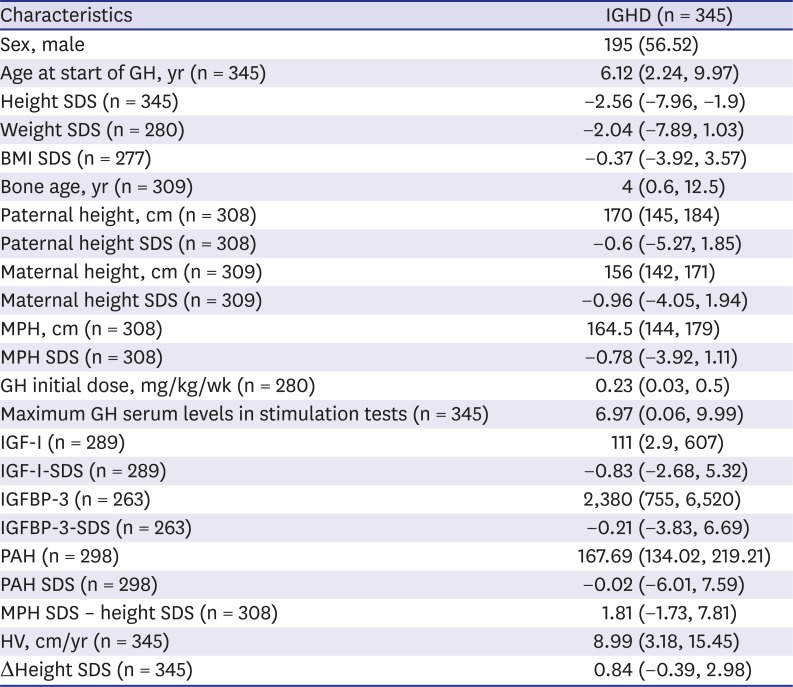
Characteristics of patients with I-GHD at the start of GH treatment
Data are presented as median (range) or number (%).
GHD = growth hormone deficiency, GH = growth hormone, SDS = standard deviation score for chronological age, BMI = body mass index, MPH = mid parental height, IGF-I = insulin-like growth factor-I, IGFBP-3 = insulin-like growth factor binding protein-3, PAH = predicted adult height, HV = height velocity, Δheight SDS = change in height standard deviation score between before and after 1 year GH treatment.
![]()
Auxological and clinical data
Anthropometric data were extracted from the LGS database: sex, chronological age, height, weight, body mass index (BMI), bone age, maternal height, paternal height, MPH, GH dose (mg/kg body weight/week), maximum GH serum levels in stimulation tests, serum IGF-I and insulin-like growth factor-binding protein-3 (IGFBP-3) levels. The predicted adult height (PAH) and the standard deviation score (SDS) were calculated based on LMS from the 2017 Korean National Growth Charts for children and adolescents,10 height and bone age at the start of GH treatment. The MPH SDS was calculated by male (MPH = [paternal height + maternal height + 13]/2); Female (MPH = [paternal height + maternal height − 13]/2), then MPH were transformed into SDS values. Bone ages were calculated according to the method of Greulich and Pyle(Greulich WW, 1959 #657) by the treating physician. Serum IGF-I levels collected by multiple investigators were incorporated into ng/mL and transformed into SDS values based on age-specific normative references.11 Annual height velocity (HV, cm/year) and growth responses in height (Δheight SDS) were measured by auxological data obtained 12 ± 3 months after GH treatment.12
Statistical analysis
The prediction model for growth response (Δheight SDS) during first-year growth in response to GH treatment was developed using a multiple linear regression analysis fitted by least squares and the REG procedure in the SAS® version 9.4 (SAS Institute, Inc., Cary, NC, USA). A hierarchy of predictive factors was derived by the all-possible regression approach. First, we selected significant variables from the simple regression analysis (Table 2). The significant variables by the simple regression analysis. Second, multiple regression analysis with variance inflation factor was performed. To avoid duplication, we exclude variables with high correlation with suspected co-linearity when variance inflation factor was over 10. The final model was determined by selecting a model with Mallow's C(p) criterion.1314 In order to illustrate the variability in the responsiveness of individuals, the studentized residual were presented. The studentized residual was calculated as the observed HV minus the predicted HV for each observation and divided by its standard error. Data are presented as median (range) or number (%) and missing data were not substituted. A P < 0.05 was considered statistically significant.
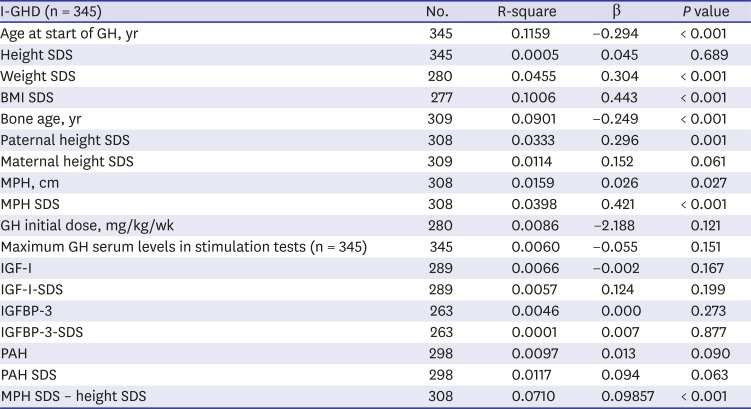
Table 2
Simple regression analysis between Δheight SDS during 1st year of GH treatment and characteristics of patients with I-GHD at the start of GH treatment
SDS = standard deviation score for chronological age, GH = growth hormone, GHD = growth hormone deficiency, BMI = body mass index, MPH = mid parental height, HV = height velocity, Δheight SDS = change in height standard deviation score between before and after 1 year GH treatment, IGF-I = insulin-like growth factor-I, IGFBP-3 = insulin-like growth factor binding protein-3, BMI = body mass index, PAH = predicted adult height.
![]()
Ethics statement
Our study protocol was reviewed and approved by the Institutional Review Board of The Catholic University of Korea (VC12OSME0004) and written informed consent was obtained from the parent or guardian on behalf of the child. The present study was registered at ClinicalTrials.gov (identifier: NCT01604395).
Go to :
RESULTS
The demographic characteristics of the subjects at the start of GH treatment
The characteristics of the 345 prepubertal Korean children with idiopathic GHD (195 males, 150 females) at the start of GH treatment are listed in Table 1. The chronological age (years) of the subjects at start of GH was 6.12 years old (ranged from 2.24 to 9.97 years). The auxological parameters of their paternal pairs (n = 308, paternal height SDS = −0.6) and their maternal pairs (n = 309, maternal height SDS = −0.96) were available. The peak GH concentration after GH stimulation was 6.97 µg/L (range, 0.06–9.99 µg/L). The initial GH treatment dose for patients was 0.23 mg/kg/week. The Δheight SDS during the first year of GH treatment was 0.84 (range, −0.39 to 2.98).
Simple regression analysis between Δheight SDS during 1st year of GH treatment and characteristics of patients with I-GHD at the start of GH treatment
The Δheight SDS during the first year of GH treatment was correlated positively with weight SDS (β = 0.304, P < 0.001), BMI SDS (β = 0.443, P < 0.001), paternal height (β = 0.054, P = 0.001), paternal height SDS (β = 0.296, P = 0.001), MPH (β = 0.026, P = 0.027), MPH SDS (β = 0.421, P < 0.001), MPH SDS minus baseline height SDS (β = 0.099, P < 0.001) and negatively with chronological age at the start of GH therapy (β = −0.294, P < 0.001), bone age (β = −0.249, P < 0.001) (Table 2).
Prediction model of Δheight SDS during 1st year of GH treatment in prepubertal Korean children with idiopathic GHD
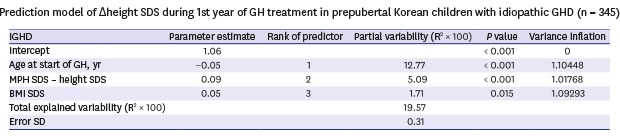
The growth prediction model for Δheight SDS during the first year of treatment was derived by Mallow's C(p) criterion with high R2 and low C(p) values described in methods section. The growth prediction model was established using the following variables: age, BMI SDS, bone age, paternal height, MPH SDS − baseline height SDS, initial dose of GH, and sex. The ranked order of the predictors, the overall correlation coefficients of the prediction model, and the R2 values of the prediction model are listed in Table 3. The equation describing the Δheight SDS during 1st year of GH treatment in prepubertal Korean children with idiopathic GHD is as follows: Δheight SDS during the first year of GH treatment = 1.06 − 0.05 × age + 0.09 × (MPH SDS − baseline height SDS) + 0.05 × BMI SDS. This model explained 19.6% of the variability of the response, with an standard error of 0.31. In order to illustrate the variability in the responsiveness of individuals, the studentized residual were presented. The plots of the studentized residuals are illustrated in Fig. 2.

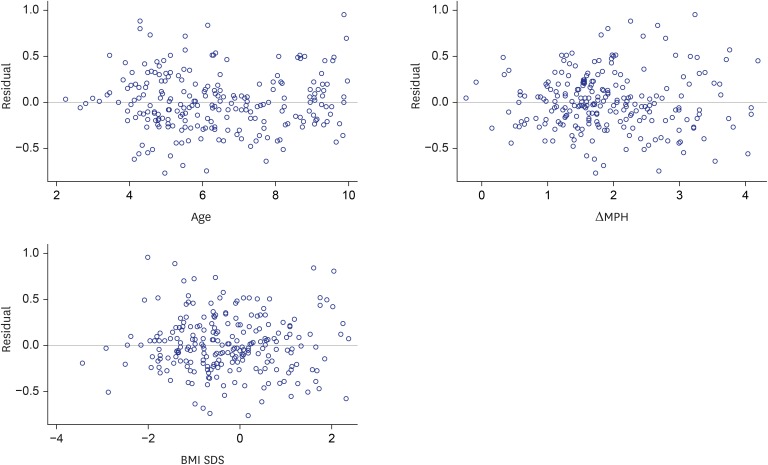 | Fig. 2Studentized residuals for prediction model of Δheight SDS. The studentized residuals and predicted value graphs in the validation of prediction models were distributed randomly between −2 and 2, and there were no values outside −3 and 3.SDS = standard deviation score, MPH = mid-parental height.
|
Table 3
Prediction model of Δheight SDS during 1st year of GH treatment in prepubertal Korean children with idiopathic GHD (n = 345)
The estimated regression equation is as follows Δheight SDS during 1st year of GH treatment = 1.06 − 0.05 × age + 0.09 × (MPH SDS – height SDS) + 0.05 × BMI SDS.
SDS = standard deviation score for chronological age, GH = growth hormone, GHD = growth hormone deficiency, IGHD = idiopathic GHD, MPH = mid parental height, BMI = body mass index, Δheight SDS = change in height SDS between before and after 1 year GH treatment, Error SD = standard deviation of error.
![]()
Go to :
DISCUSSION
The first-year response of GH therapy was important for the second-year response.15 In predicting HV during the second year or later, the HV in the first year was the most prominent predictor.16 First-year growth response reported as major determinant of adult height outcomes of short children.17 The effect of GH wanes with time, and the first year of treatment usually produce the greatest growth increment. For clinical practice, it would be desirable for a prediction model to formulate individualized GH treatment plans and to improve the outcomes of GH treatment in patients with idiopathic GHD. In this study, we present a prediction model that can be used to predict the first year response to GH treatment in prepubertal children with idiopathic GHD in Korea. We analysed the data from LGS, and have developed a model that fulfills the criteria required for routine use by a “data-driven” approach, following the recommendations of Ranke et al.7 (Table 3).
The most reliable variable for evaluating the GH response is HV, expressed as Δheight SDS. The prediction model we suggest showed that Δheight SDS during the first year of GH treatment was correlated negatively with chronological age and positively with the difference between MPH SDS and the child's present height SDS, and BMI-SDS. These findings imply that the younger, smaller, and heavier the child is, and the higher his or her genetic potential is (expressed as the MPH), the greater the first-year growth response to GH therapy will be.
These results are in accordance with other prediction models derived from other cohorts of the first-year response to GH treatment.18 Previous studies have reported that genetic potential (expressed as the MPH) and chronological age at GH therapy have the greatest influence on final height during GH therapy in subjects with idiopathic GHD.19 The prediction model of Ranke et al.16 also presents negative correlations with age, height, and height SDS minus MPH SDS, and positive associations with weight SDS. This evidence strongly supports the early recognition, referral, diagnosis, and treatment of idiopathic GHD as an important step toward optimizing growth potential.
Despite more than 50 years of experience with GH treatment in children of short stature, GH dosing remains largely uncertain. The GH dose has often been found to have a positive effect on the short-term growth response.20 The first-year HV prediction model previously published using KIGS database includes the GH dose in patients with GHD.18 It has been reported that the correlation between the GH dose and HV persists during 4 years after the start of GH treatment.16 However, no significant correlations were found between the GH dose and long-term GH treatment strategies.21 In this study, we found no significant associations between the GH dose and the first-year response to GH treatment in prepubertal Korean children with idiopathic GHD. In addition, the IGF-I-SDS and IGFBP-3-SDS have been reported to show negative correlations with the outcomes of GH therapy in other studies.22 The IGF-I-SDS and IGFBP-3-SDS were generally suggestive of GH secretion and considered an alternative approach to the diagnosis of GHD.2324 However, in this study, the IGF-I-SDS and IGFBP-3-SDS were not significantly correlated with the GH response in simple regression analysis. IGF-I and IGFBP-3 values were derived from a multiple hospitals and medical centers choosing multitude of commercial or in-house assays. The IGF-I assay-specific normal reference ranges are very different for each measuring instrument.25 The lack of central laboratory analysis in LGS might limit the interpretation of relevant blood analyses, especially IGF-I and IGFBP-3. However, IGF-I measurements had reached a higher degree of standardization.26 In addition, IGF-I and IGFBP-3 values were transformed into SDS values in LGS. Therefore, the no significant association of IGF-I-SDS with the GH response in this study might provide some information relating to these parameters in predicting first-year growth response. More careful concerns including control over immunoassay measurements are needed to establish the relationship of IGF-related assays, which can reflect the GH status.
To the best of our knowledge, this is the first study to predict first-year growth in response to GH treatment in prepubertal Korean children with idiopathic GHD. This prediction model captured 19.6% of the variation in the first-year response, and the standard error was 0.31. Compared with other predictive models that captured at least 40% of the variation, the R2 values (predictive power) of this study were relatively low.27 However, the degree of accuracy was not low compared to other papers. Furthermore, the large scale cohort dataset from LGS give support to the result of the present study can be considered reliable.
The results presented above may have a few limitations. This study is an observational study without an untreated control group. It is difficult to confirm patient compliance. Moreover, laboratory parameters, such as IGF-I and IGFBP-3, were measured at each institutions, which might contribute to an inter laboratory measurement bias. To overcome these limitations and to minimize the risk of bias due to missing data, we used a systematic approach to data collection. Although this prediction model will need further improvement and validation, it might allow more tailored and personalized GH treatment in Korean prepubertal children with idiopathic GHD.
Go to :
 XML Download
XML Download