

 PDF
PDF Citation
Citation Print
Print



At present, Korea has one of the largest outbreak of coronavirus outside of China, bringing the country's total infection to more than 9,000.1 More than half of these cases have been reported in Daegu, 300 kilometers away from Seoul. Meanwhile a major cluster of infections in Seoul was identified during February 21–26, in an 800-bed university hospital in Eunpyeong-gu, northwest Seoul, linking 14 coronavirus disease 2019 (COVID-19) cases out of 65 cases in the capital at that time.2
Two community-acquired 2019 novel coronavirus (severe acute respiratory syndrome coronavirus 2 [SARS-CoV-2]) pneumonia cases were diagnosed in-hospital. Both of them were male in their 60–70s, and had symptoms of mild fever, generalized weakness, and myalgia. Chest CTs showed multiple, ground-glass opacities in both lungs. There was a delay in the diagnosis as there were no high risk epidemiologic factors such as visit to Wuhan city, elsewhere in China, and Hong Kong or a close contact with confirmed cases, as the announced Korea Centers for Disease Control and Prevention (KCDC) case definition was narrow at that time. Two more confirmed cases (1 hospital staff responsible for transporting patients, and 1 caregiver) were identified in-hospital.3 Rest of the 10 cases were those who contacted the confirmed cases but were either discharged before the in-hospital COVID-19 cases were identified or family members or caregivers of the confirmed cases. These 10 cases were diagnosed outside the hospital.
This was the first major cluster infection that occurred in Seoul, a megacity. Fearing mass outbreak, the city government took excessive measures to temporarily close the entire outpatient service including the emergency room for two weeks under the guidelines set during the 2015 Middle East respiratory syndrome (MERS) outbreak.4 Here we report the 17 days closing of Eunpyeong St. Mary's Hospital in Seoul, Korea (Fig. 1).
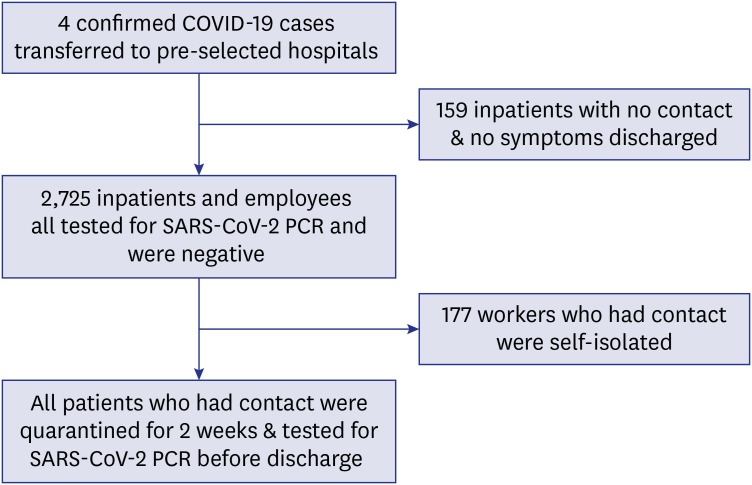
The 4 cases that were identified inside the hospital were transferred to preselected hospitals where infectious disease units were ready for isolation of confirmed cases. Then the hospital conducted a full-scale contact tracing and isolated people who contacted the patients. The 159 patients who did not contact the confirmed patients and had no symptoms were discharged. It is known that transmission of COVID-19 may be possible even from asymptomatic contacts.5 To prevent in-hospital transmissions, all 2,725 inpatients and employees (212 doctors, 1,069 nurses, 455 administrative and medical support employees, 483 inpatients, 79 guardians and caregivers, and 427 contract workers) had undergone SARS-CoV-2 polymerase chain reaction (PCR) testing by nasopharyngeal aspirate and all were tested negative.
The 177 employees who had contact were self-isolated although PCR results were negative, as the PCR testing may not initially return positive.6 During the hospital shutdown period, the rest of the employees commuted by their personal cars and did not use public transportation as a measure of social distancing.7 Those who could not use a car were not allowed to come to work.
The patients (49–134 people depending on the time of contact) who had contact with the confirmed patients were quarantined during the suspension period and placed in single rooms. Since caregivers (professional or family) were not allowed to stay at wards, the medical staff provided care for inpatients 24 hours a day in shifts. All the employees used gowns, gloves, medical masks and eye protection when providing care to all remaining patients. Among the patients who were either discharged during the suspension period or quarantined, we repeated SARS-CoV-2 PCR before discharge as there was the possibility of delayed positivity in coronavirus testing in relation to illness onset.6 All of the repeated PCR results were negative. Those who were quarantined had terminated isolation on the day the suspension period ended. After the hospital re-opened, all of the new employees had to be tested SARS-CoV-2 PCR negative to enter the building.
Closing and isolating the hospital seemed to have played a useful role in preventing the spread of COVID-19 in-hospital and to the local community. However concerns have been raised due to the prolonged suspension period set by the government following the old guidelines established during the MERS outbreak.4 Many studies have shown that although human coronaviruses can remain infectious on inanimate surfaces for up to 9 days, it can be significantly disinfected within 1 minute exposure time using 0.1% sodium hypochlorite or 62%–71% ethanol.8 Also based on 12 air changes per hour, it takes only 30 minutes for removal efficiency of 99.9% of airborne contaminants.9 These evidences show that revision of the current infection control guideline is inevitable. The existing patients could not receive timely treatments and some were denied care elsewhere during the shutdown period. Therefore extreme measures to close the entire hospital were considered unreasonable by many people. There were also controversial questions of the quarantine period as a majority of our patients were asymptomatic and found the days in-hospital too grueling.
We repeated SARS-CoV-2 PCR twice to confirm it was negative before de-isolating, however regarding the exam cost, this may not be applicable to other districts or countries.10 More data is needed to refine and establish the in-hospital quarantine and de-isolation processes based on the various epidemiological and clinical settings.
 XML Download
XML Download