

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Posttraumatic stress disorder (PTSD) is one of the most common consequence of sexual assault with one-third of raped women meeting the diagnostic criteria.1 Rape and sexual assault are reported as two of the three traumas accounting for the highest proportions of PTSD worldwide.2 In a prospective study with rape victims, PTSD characterized 94% of victims within 2 weeks postassault and 47% of victims within 3 months postassault.3 In a pilot study in Korea, 68% of female victims of sexual assault met diagnostic criteria for PTSD after 1 to 2 months following the trauma.4 A number of studies have examined correlates of the PTSD symptomatology in sexual assault victims to identify those survivors most likely to develop PTSD after the traumatic event. These studies have presented that various factors including demographic background, traumatic event characteristics, and postassault victims' responses may be predictive of PTSD. The ultimate goal of these numerous studies is to provide effective initial intervention for victims of sexual assaults by detecting the threat early.
Recent research has reported individual differences in how people respond to trauma.56 Some people after trauma experience minimal emotional distress and transient disruptions in their ability to function, while others suffer more intense pain that lasts longer.5 Researchers have suggested that the ability to buffer and avoid the negative effects of sexual assault, termed resilience, may lie in specific social and cognitive protective factors.78 Longitudinal studies generally focused on people highly distressed by sexual assault,34 while most researchers have not shown interest in prognosis for the low distressed people. Victims of sexual assault need suitable intervention even if they don't seem to be suffering from the trauma. Therefore, information about the factors involved in the progress for both high distressed and low distressed victims in the early days from the trauma is requested to provide appropriate intervention for victims of sexual assault.
Assault characteristics associated with PTSD symptoms include perceived life threat, substantial use of verbal and physical force and completed rapes.91011 The literature of assault related risk factors shows highly discrepant results.12 It has been found that rape victims of a stranger have an increased risk of PTSD compared with victims of other offenders,1314 whereas others have found that rape victims of current partners have the highest risk of developing PTSD.15
Post-traumatic negative cognition plays an important role in the development and persistence of PTSD in the traumatized victims.16 Ehlers and Clark17 also proposed that negative appraisals of traumatic events increase the fear, which makes PTSD symptoms and anxiety persist. Thoughts about one's perceived weaknesses and the dangers of the world affect the development of PTSD in rape victims.18 Similarly, negative thoughts about the world and one's incompetence mediate the development of PTSD after sexual assault.1920 Foa's and Ehlers-Clark's groups have demonstrated the importance of post-traumatic cognitions related to persistence and reduction of PTSD symptomatology.162122 However, how post-traumatic cognition contributes to the PTSD according to the initial response to trauma remains unclear.
The purpose of the current study was to examine the short-term progress of PTSD symptoms in female victims of sexual trauma. We hypothesized that initially low-distressed victims would show a different course of PTSD symptomatology from initially high-distressed victims. Moreover, the study aimed to investigate the relationships between assault-related factors, trauma-related cognitions, and PTSD severity.
Go to : 
METHODS
Participants and procedure
Data were obtained from the Sunflower Center of Southern Gyeonggi for Women and Children Victims of Violence at the Ajou University Hospital in Korea. The Sunflower Center is a government-sponsored center that provides victims of violence with medical care, social service, psychological support and criminal investigative services. At registration, victims signed consent forms for assessment. For this study, we investigated the records of 94 female victims who visited the Sunflower Center of Southern Gyeonggi for Women and Children Victims of Violence to receive services following sexual violence between December 2014 and November 2016.
Demographic characteristics and the features of the sexual violence were obtained from data recorded at the initial assessment. At the initial assessment, victims completed a self-report questionnaire to examine the severity of post-traumatic stress symptoms, and trauma-related cognition. One month after the initial assessment, victims were contacted by telephone and re-evaluated for the severity of post-traumatic stress symptoms.
Measures
Background characteristics of participants and the sexual violence were obtained at the initial assessment. Assault-related factors including type of sexual assault, relationship with the perpetuator, repetitions of sexual assault, violence in the assault and photographs taken during the assault were investigated.
At the initial assessment, victims completed the post-traumatic cognitions inventory (PTCI) to assess trauma-related thoughts and beliefs. The PTCI consists of 33 items and uses. The PTCI produces three subscores based on the mean of items for each subscale: negative cognitions about the self (negative-self, 21 items), negative cognitions about the world (negative-world, 7 items), and self-blame for trauma (self-blame, 5 items). The PTCI subscales have good test-retest reliability (0.75–0.89), good internal consistency (Cronbach's α = 0.86–0.97), and moderate-to-high correlations with post-traumatic stress symptom severity (Foa et al.20). The PTCI items were translated into Korean by the first author, and subsequently reviewed by a fluent bilingual psychiatrist with a PhD in psychiatry.23 Cronbach's α in this study was 0.96.
The PTSD symptoms scale, self-report version (PSS-SR), was administered at the initial assessment and 1 month later to assess the severity of post-traumatic stress symptoms. The 17 items of PSS-SR correspond to the Post-traumatic stress disorder symptoms listed in the Criteria B items in Diagnostic and Statistical Manual of Mental Disorder 4th edition.24 The PSS-SR has an acceptable-to-good reliability and validity.19 Participants defined as belonging to the high-distress group were those participants having a high score on the PSS-SR at the initial assessment, i.e., scores higher than 20, cut-off score of PSS-SR.25 Participants having a score lower than 20 on the PSS-SR at the initial assessment were assigned to the low-distress group.
Data analysis strategy
In this study, the sample of 94 participants were divided into two groups depending on the PSS-SR scores at initial assessment: High-distress group and Low-distress group. Categorical variables were compared with the χ2 test, and continuous variables were compared with the independent t-test. Repeated-measures analyses of variance (ANOVA) was used to determine changes across time points. Correlations between trauma-related cognition and PTSD symptom severity were calculated using Pearson's statistic. Stepwise multiple regression analysis was used to examine assault-related factors and trauma-related cognitions predicting PTSD symptom severity after 1 month. Both of the correlation and regression analyses were conducted separately for each group. All statistical tests were two-sided. Statistical analysis PASW statistics software version 18.0 (SPSS Inc., Chicago, IL, USA) was used for statistical analyses.
Ethics statement
All procedures of the present study were reviewed by the Institutional Review Board (IRB) of Ajou University Medical Center (IRB No. AJIRB-SBR-SUR-15-081). Individual informed consent was waived due to retrospective design of the study.
Go to :
RESULTS
A total of 510 females reporting sexual victimization visited the Center between December 2014 and November 2016. Among these victim records, 94 women had completed the psychological measures (PTCI, PSS-SR, and follow-up PSS-SR by telephone interview) and recorded assault characteristics (type of sexual assault, type of perpetuator, repeated sexual assaults, violence and taken photographs during the assault) without missing data.
The background characteristics of the participants are shown in Table 1. The mean age of the participants was 24.78 ± 6.89 years at the time of the initial assessment. Among the 94 female victims included in the analysis, 71 (71.5%) were rape victims and 59 (62.8%) were victimized by acquaintances. Twenty-two (23.4%) victims experienced violence during the assault and photographs were taken during the assault in 7 cases (7.5%). Eighteen (19.2%) have experienced sexual assaults more than once. Comparisons revealed that the type of sexual assault, experiencing violence during the assault, having photographs taken during the assault, and repeated sexual assaults were not significantly different between the low-distress and high-distress groups. Only type of perpetuator showed a significant difference between the groups, i.e., the high-distress group victims were more likely to have been victimized by acquaintances.
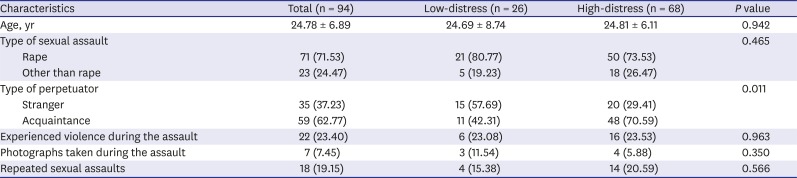
Table 1
Background characteristics of the participants
![]()
The mean PSS-SR scores at each time point are presented in Table 2. Repeated-measures ANOVAs were conducted with time (initial vs. 1 month follow-up) as the within-group factor and group (Low-distress vs. High-distress) as the between-group factor. A main effect for time was observed with PSS-SR reexperience scores (F [1, 92] = 4.112, P = 0.045). A significant interaction between time and group was observed with PSS-SR total (F [1, 92] = 10.062, P = 0.002), reexperience (F [1, 92] = 5.767, P = 0.018), avoidance (F [1, 92] = 8.530, P = 0.004), and arousal scores (F [1, 92] = 4.675, P = 0.033).
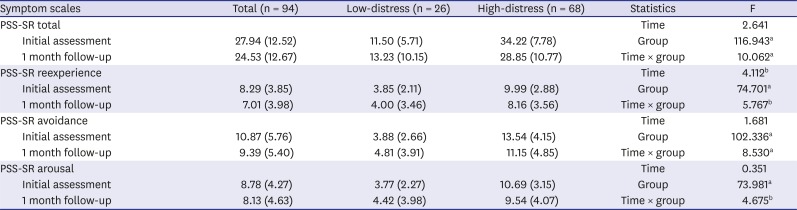
Table 2
Severity of post-traumatic stress symptoms at each time point
Values are presented as number (%).
PSS-SR = posttraumatic stress disorder symptoms scale, self-report version.
aP < 0.01; bP < 0.05.
![]()
PTCI total score (r = 0.626, P = 0.001), scores of negative-self subscale (r = 0.667, P < 0.000), negative-world subscale (r = 0.400, P = 0.043), and self-blame subscale (r = 0.464, P = 0.017) showed a statistically significant correlation with follow-up PSS-SR score in the low-distress group. In the high-distress group, PTCI total score (r = 0.411, P < 0.000), negative-self (r = 0.380, P = 0.001), and negative-world (r = 0.509, P < 0.000) showed a statistically significant correlation with follow-up PSS-SR score (Table 3).

Table 3
Correlations between trauma-related cognitions at initial assessment and post-traumatic symptoms at the 1 month follow-up
| PTCI | PSS-SR score at the 1 month follow-up | |
|---|---|---|
| Low-distress (n = 26) | High-distress (n = 68) | |
| Negative-self | 0.667a | 0.380a |
| Negative-world | 0.400b | 0.509a |
| Self-blame | 0.464b | 0.084 |
| Total score | 0.626a | 0.411a |
PSS-SR = posttraumatic stress disorder symptoms scale, self-report version, PTCI = post-traumatic cognitions inventory.
aP < 0.01; bP < 0.05.
![]()
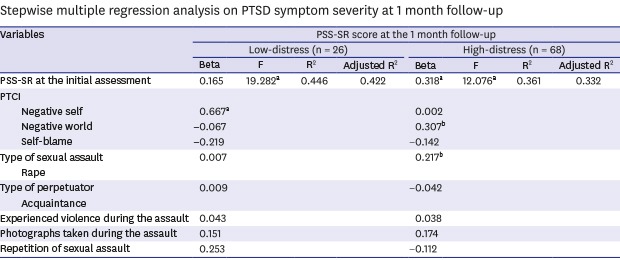
The PSS-SR score at the initial assessment, PTCI subscale scores and characteristics of sexual assault were included as independent variables in stepwise multiple regression. Stepwise multiple regression analysis showed that PSS-SR score at the initial assessment (β = 0.318, P = 0.009), negative-world score of PTCI (β = 0.307, P = 0.013) and type of sexual assault (β = 0.217, P = 0.037) predicted PTSD symptoms severity one month later in the high-distress group. The regression model, factoring in PSS-SR score at the initial assessment, negative-world, and type of sexual assault, showed a 36.1% explanatory power regarding the PSS-SR score at the 1 month follow-up. In the low-distress group, only negative-self score of PTCI (β = 0.667, P < 0.000) predicted PTSD symptoms severity at the 1 month follow-up with 44.6% explanatory power (Table 4).

Table 4
Stepwise multiple regression analysis on PTSD symptom severity at 1 month follow-up
PSS-SR = posttraumatic stress disorder symptoms scale, self-report version, PTCI = post-traumatic cognitions inventory; PTSD = posttraumatic stress disorder.
aP < 0.01; bP < 0.05.
![]()
Go to :
DISCUSSION
In consistency with prior studies, we found a high prevalence of posttraumatic symptomatology in the sample. At the initial assessment, 68 (72.3%) victims reported significant posttraumatic stress symptoms, higher than the cut-off score of PSS-SR. This study investigated the assault-related risk factors of PTSD symptoms in initially high-distress and low-distress female victims of sexual trauma. Comparison analysis revealed that most of the assault-related factors including type of sexual assault, experiencing violence during the assault, having photographs taken during the assault, and repeated sexual assaults were not significantly different between the high-distress and low-distress groups depending on the PSS-SR scores at initial assessment. These results were different from the findings of previous studies which reported that completed rape, physical injury, and life threat related to PTSD in female crime victims.1226 These discrepancies may be due to the small sample size of “other than rape” victims (23%), violence (22%), taken photographs (7%), and repeated sexual assaults (18%) in this sample and a less powerful single-item, dichotomous measuring. Only victims of acquaintance rapes showed higher PTSD symptoms compared with victims of strangers in this study. Similarly, Temple et al.15 reported victims of partners have the highest risk of developing PTSD. However, some studies have not found any association between differences in victim-offender relationships and PTSD,1327 while others reported stranger rapes as a risk factor of PTSD.28 Although quite a few studies have been conducted trying to clarify the relationship between assault related factors and the PTSD symptom severity after rape, the results have been highly discrepant. Thus, future studies should be designed with comprehensive information about traumatic events to fully understand the effects of assault characteristics to post assault sequelae.
We compared the process of PTSD symptoms between the low-distress and high-distress group. Repeated-measures ANOVA revealed significant interaction between time and group was observed with PTSD symptoms. Concretely, the high-distress group showed that PTSD symptom severity decreased over the month. The low-distress group did not show significant change in PTSD symptom severity, but rather PTSD symptom severity was slightly increased over the month even though not statistically significant. Recent theories have proposed distinct trajectories of psychological health following traumatic stress: resilience, recovery, chronic impairment, and resistance trajectories.56 Several studies have supported these trajectories following various traumas including serious illness or severe injury, deployment to a peacekeeping mission, and mass disaster.29303132 We also need to consider delayed-onset PTSD. Delayed-onset PTSD, diagnosed more than 6 months after the traumatic event, were observed in 25% of all PTSD cases, but few developed the disorder without early sub-threshold PTSD symptoms.33 However, Steenkamp et al.32 identified distinct trajectories of PTSD symptomatology during the early aftermath of sexual assault and suggested trajectories of mental health in victims of sexual assault are different from other traumas. Because sexual assaults are severe interpersonal trauma involving marked initial emotional chaos, further studies about trajectories following sexual trauma are needed.
This study also investigated if assault-related factors and trauma-related cognitions were associated with later PTSD symptoms in female sexual assault victims in a relatively short-term follow-up period. In correlation analysis, negative cognitions about the assault were strongly correlated with PTSD symptom severity one month later in both of low-distress and high-distress groups. In particular, negative cognitions about the self at the initial assessment predicted the PTSD symptoms one month later with a high explanatory power (42.2%) in the low-distress group. In the high-distress group, PTSD symptoms at the initial assessment, negative cognitions about the world, and type of sexual assault, i.e., rape, predicted the PTSD symptoms one month later with a 33.2% explanatory power. These results were comparable to those of a prospective study that reported that dysfunctional cognitions concerning sexual assault seem to strongly affect the maintenance and severity of PTSD symptoms.41634 This study confirmed the role of negative appraisals of trauma in maintaining PTSD symptomatology. Dunmore et al.35 have proposed that the role of cognitive factors in the maintenance of PTSD has been a particularly robust finding with victims of assault. The predictive power of these trauma-related cognitions suggests the effectiveness of cognitive therapeutic intervention for victims of sexual assault both of high-distressed and low-distressed people. Specifically, sense of psychological autonomy seems to play an important role in the low-distress group, and confidence in the world is significant in the high-distress group for recovery from the trauma sequelae.
Our findings should be interpreted with some caveats. First, only 18.4% of the victimized women were eligible to be included in the analysis, so these results must be viewed very cautiously. This limitation suggests that systematic data gaining is needed to yield comprehensive and representative results. Second, current results may have limited generalizability because they reflect responses of sexually traumatized female subjects, which are likely to differ from other trauma subjects or male subjects. However, homogeneity of the trauma sample in this study is a strength that distinguished it from previous studies. Second, the findings on posttraumatic cognition and PTSD symptom severity relied on self-report questionnaires. Thus, person-to-person interviews with structured formats should be featured in a future study.
Despite these limitations, strengths of this study are that we investigated the relationship among assault-related factors, trauma-related cognitions in high-distress and low-distress female victims of sexual violence at the early stage of trauma, and PTSD symptoms one month later after the initial assessment. In this study, the results show that the low-distress group and high-distress group show different progresses of PTSD symptoms at short-term follow-up, and that trauma-related cognitions are more important predictors of PTSD severity one month later rather than assault-related factors. Our results suggest that cognitive appraisal regarding the dangerousness of the world is crucial in the maintenance of PTSD in high-distressed victims at the early trauma phase, while cognitive appraisal concerning psychological autonomy seems to play an important role in initially low-distressed victims. In conclusion, our results highlight the importance of research into PTSD risk factors as well as evidence-based treatment for victims of sexual assault.
Go to :
 XML Download
XML Download