

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Coronary artery disease accounts for approximately 80% of sudden cardiac arrest (SCA).12 Of the coronary artery diseases, acute coronary syndrome with coronary stenosis due to atherosclerosis is principally related to SCA, while SCA related to coronary vasospasm is a minority.2 However, the Asian population has high incidence of variant angina or SCA related to coronary vasospasm,345 because they have a diffuse coronary vasomotor reactivity as compared to Caucasians.6 Apart from racial differences, recreational drug overdose-related death, which might be due to coronary vasospasm, is increasing.789 Therefore, coronary vasospasm is considered to be an important cause of SCA that cannot be ignored.
Coronary vasospasm, which is characterized by reversible ischemia without any structural pathology in the coronary arteries,10 can also lead to lethal arrhythmias, myocardial infarction, and SCA.11121314 Although vasospasm-related SCA is believed to have a better prognosis due to its pathogenesis, previous studies reported that out-of-hospital cardiac arrest (OHCA) survivors with coronary vasospasm etiology demonstrated considerable long-term mortality or major adverse events after cardiac arrest.1314 Previous studies attempted to elucidate the significance of variant angina manifesting as OHCA. However, they only compared variant angina with and without SCA.1314 Therefore, little is known about whether vasospasm-related SCA has better clinical outcomes than SCA due to stenotic coronary artery disease, which is the most common cause. To evaluate the characteristics and clinical outcomes of vasospasm-related SCA, it should be compared with atherosclerotic coronary artery syndrome-related SCA.
We hypothesized that OHCA due to coronary vasospasm would be different as compared to OHCA due to stenotic coronary artery disease. Therefore, we included OHCA survivors who underwent coronary angiography (CAG) and compared the survival and neurologic outcome 30 days after cardiac arrest between the coronary vasospasm and stenosis groups. To examine whether a difference in outcome arises from clinical characteristics, we used propensity score-matching to balance the characteristics between the vasospasm and stenosis groups.
METHODS
Study design and population
This multicenter, retrospective, observational, registry-based study was conducted at 8 tertiary university affiliated teaching hospitals in Korea. Data were extracted from registries of consecutive patients with OHCA since January 2010.15
We extracted OHCA survivors with presumed cardiac etiology who underwent CAG at any time during admission. We included patients who demonstrated > 50% stenotic coronary lesions or vasospasm on CAG between January 2010 and December 2015. The patients who had undergone a previous coronary artery bypass graft, had no stenotic coronary artery, or had minimal to ≤ 50% of coronary artery stenosis, were excluded.
Management and data collection
An interventional cardiologist at each hospital decided the timing of CAG and judged the angiographic findings. This individual also planned medical treatment with/without percutaneous coronary intervention (PCI). During the study period, comatose OHCA patients underwent targeted temperature management (TTM) according to the standard protocols at each hospital. Target temperature of 33°C or 36°C was maintained for at least 24 hours. After completion of the maintenance period, patients were rewarmed at a rate of 0.25 to 0.5°C/hr. The attending physician decided about the use of vasopressors, nitrate, intra-aortic balloon pump (IABP), or extracorporeal membrane oxygenation (ECMO) according to the status of patients.
We obtained the following data: age, gender, pre-existing illness, presence of a witness on collapse, bystander cardiopulmonary resuscitation (CPR), first monitored rhythm, time from collapse to return of spontaneous circulation (ROSC), prehospital ROSC, Glasgow Coma Scale (GCS) after ROSC, ST segment elevation on electrocardiogram, angiographic finding, ventricular fibrillation after CAG or PCI, requirement of vasopressor (norepinephrine, vasopressin, epinephrine, dopamine, and dobutamine), nitrate, IABP, ECMO, or TTM, survival and neurologic outcomes at 30 days after cardiac arrest.
Based on angiographic findings, patients were divided into either vasospasm or stenosis groups (> 50% stenosis on any coronary artery). The diagnosis of vasospasm was made with spontaneous coronary spasm on CAG or documented coronary spasm on an ergonovine provocation CAG.16 Patients with mixed vasospasm and stenotic lesions were designated to either the vasospasm or the stenosis group based on the dominant pathology, which was decided by the interventional cardiologist.
The primary outcome was survival 30 days after cardiac arrest and the secondary outcome was a good neurologic outcome 30 days after cardiac arrest. Neurologic outcome was measured using the cerebral performance category (CPC) scale and we defined good neurologic outcome as CPC 1 and 2.17
Statistical analysis
We described categorical variables as frequencies with percentages, and continuous variables as mean with standard deviation (SD) or median with interquartile range, according to normality testing. Comparisons between the vasospasm and stenosis groups were performed using the χ2 test or Fisher's exact test for categorical variables, and independent t-test or Mann-Whitney U test for continuous variables.
To reduce the selection bias and potential confounding factors in an observational study, we calculated a propensity score and performed matching between the vasospasm and stenosis groups. The propensity score was calculated using a multivariate logistic regression model based on variables, with P < 0.2 between vasospasm and stenosis groups (Table 1). Propensity score matching was performed in a one-to-one fashion between the two groups using calipers with a width equal to the SD of the logit of the propensity score. We examined the difference between the vasospasm and stenosis groups by calculating absolute standard differences. An absolute standardized difference ≥ 10% between the two groups was considered to be significant. We used the McNemar's test for categorical variables and Wilcoxon signed-rank or paired t-test for continuous variables, for comparison between the two groups in the propensity score-matched cohort.
Table 1
Characteristics of out-of-hospital cardiac arrest survivors compared with coronary vasospasm and coronary stenosis
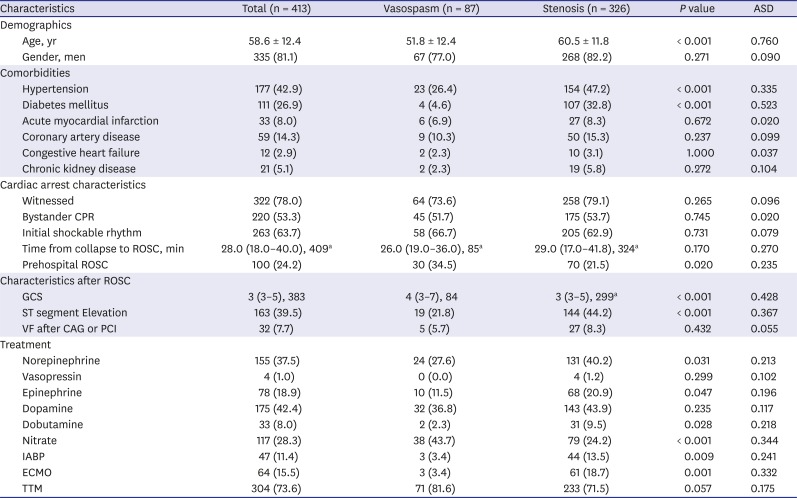
All data presented as mean ± standard deviation or median (interquartile range) for continuous variables, and number (%) for categorical variables.
ASD = absolute standardized difference, CPR = cardiopulmonary resuscitation, ROSC= restoration of spontaneous circulation, GCS = Glasgow Coma Scale, VF = ventricular fibrillation, CAG = coronary angiogram, PCI = percutaneous coronary intervention, IABP = intra-aortic balloon pump, ECMO = extracorporeal membrane oxygenation, TTM = targeted temperature management.
aIncluded number of patients for analysis.
We used multivariate regression analysis to assess the association between the vasospasm group and clinical outcomes. All variables with P < 0.2 in univariate comparisons between survivors and non-survivors and between good and poor neurologic outcomes were included in the multivariate logistic regression model. We used a backward stepwise approach, sequentially eliminating variables with P > 0.10 to build a final model. Goodness of fit of the final model was evaluated using the Hosmer–Lemeshow test. We presented the logistic regression analyses results as odds ratio (OR) and 95% confidence interval (CI). We used the log-rank test to compare the length of survival until 30 days after cardiac arrest. Survival statistics at the end of 30 days after cardiac arrest were constructed using the Kaplan–Meier plot and compared with the log-rank test. We performed all analyses with SPSS version 18.0 (IMB Corp., Armonk, NY, USA) and Stata version 13.1 (StataCorp., College Station, TX, USA). Statistical significance was set as two-sided P values < 0.05.
Ethics statement
The protocol of this study was based on the ethical standards of the Declaration of Helsinki and was approved by the Institutional Review Board of the Chonnam National University Hospital (CNUH-2016-246). Informed consent was waived due to the retrospective nature of the study. The OHCA registry enrolled adult non-traumatic OHCA survivors.
RESULTS
Patient selection
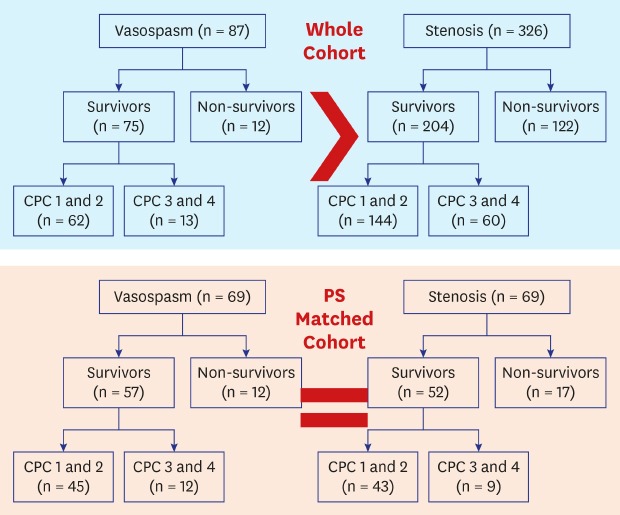
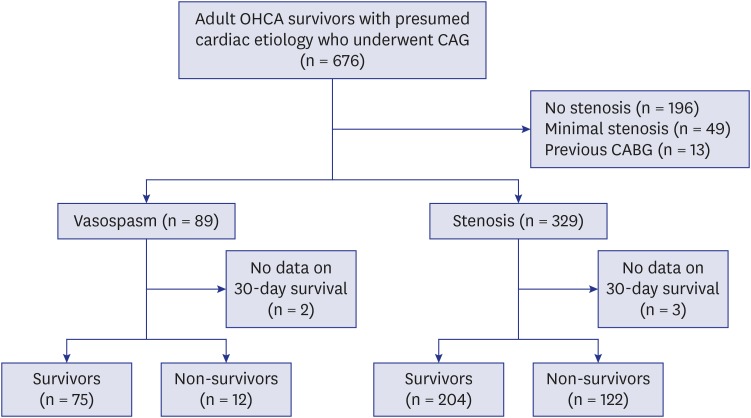
A total of 676 OHCA survivors with presumed cardiac etiology underwent CAG during the study period; of them, 258 were excluded due to no vasospasm, no stenosis, or stenosis < 50%. Of the remaining 418 patients, 89 were designated to the vasospasm group and 329 to the stenosis group, while 2 and 3 patients were excluded due to lack of outcome data in each group, respectively. Thus, 413 patients were included in the study (Fig. 1).
Comparison between coronary vasospasm and stenosis groups
Characteristics of the patients before propensity score matching are summarized in Table 1. The vasospasm group patients were younger, and less likely to have hypertension and diabetes. The vasospasm group achieved a higher rate of prehospital ROSC, had a higher GCS, and were less likely to have ST segment elevation on an electrocardiogram. The vasospasm group required lesser vasopressors, IABP, and ECMO, while they required more nitrates. The vasospasm group had a significantly higher survival and good neurologic outcome in the entire cohort (Fig. 2). Survival analysis with the Kaplan-Meier plot shows better survival in the vasospasm group at the end of 30 days after cardiac arrest in the entire cohort (log-rank P < 0.001) (Fig. 3).
Fig. 2
Survival and good neurologic outcome on 30 days after cardiac arrest between out-of-hospital cardiac arrest survivors with coronary vasospasm and with coronary stenosis. (A) Vasospasm group has higher survival and good neurologic outcome in the whole cohort. (B) Survival and neurologic outcome are not different between vasospasm and stenosis groups in the propensity score-matched cohort.
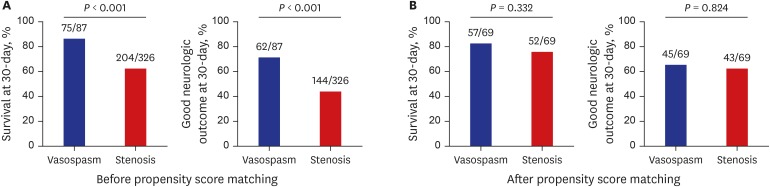
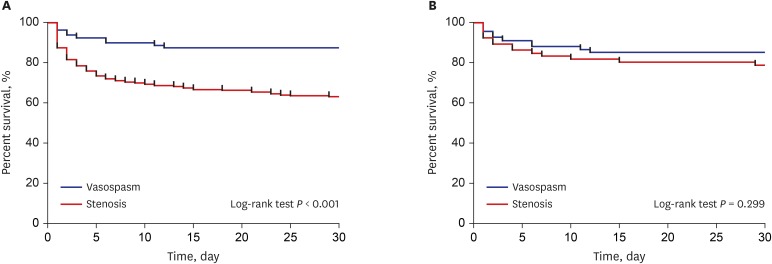
Fig. 3
Kaplan-Meier plots until occurrence of all causes of mortality during 30 days after cardiac arrest in the vasospasm and stenosis groups. (A) The vasospasm group has higher cumulative survival than the stenosis group (P < 0.001) in the whole cohort. (B) Vasospasm and stenosis groups have similar cumulative survival in the propensity score-matched cohort (P = 0.299).
Comparison between coronary vasospasm and stenotic groups
There were 279 (67.6%) survivors and 206 (49.9%) patients who had good neurologic outcomes 30 days after cardiac arrest in the entire cohort. Table 2 demonstrates a comparison of characteristics between survivors and non-survivors and between good neurologic outcome and poor neurologic outcome groups. Survivors had a higher frequency of vasospasm than non-survivors (26.9% vs. 9.0%, P < 0.001). However, vasospasm was not independently associated with survival (OR, 0.980; 95% CI, 0.400–2.406) (Table 3). The use of dopamine, IABP, and ECMO was associated with decreased survival, while use of nitrate was associated with increased survival. The good neurologic outcome group had a higher frequency of vasospasm than the poor neurologic outcome group (30.1% vs. 12.1%, P < 0.001). However, the vasospasm group was not independently associated with a good neurologic outcome (OR, 0.870; 95% CI, 0.359–2.108) (Table 3). The use of dopamine, epinephrine, and IABP was associated with poor neurologic outcome, while the use of nitrate was associated with good neurologic outcome.
Table 2
Characteristics stratified as per the primary and the secondary outcomes
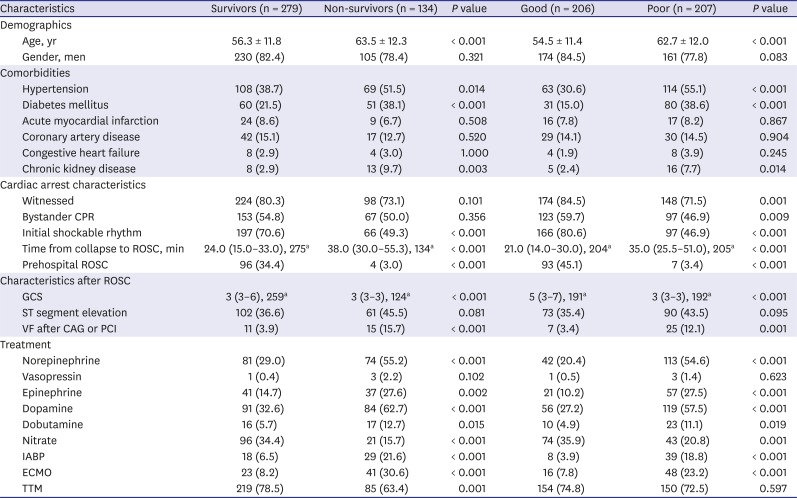
All data presented as mean ± standard deviation or median (interquartile range) for continuous variables, and number (%) for categorical variables.
CPR = cardiopulmonary resuscitation, ROSC = restoration of spontaneous circulation, GCS = Glasgow Coma Scale, VF = ventricular fibrillation, CAG = coronary angiogram, PCI = percutaneous coronary intervention, IABP = intra-aortic balloon pump, ECMO = extracorporeal membrane oxygenation, TTM = targeted temperature management.
aIncluded number of patients for analysis.
Table 3
Multivariate logistic regression analyses for survival and good neurologic outcome on 30 days after cardiac arrest
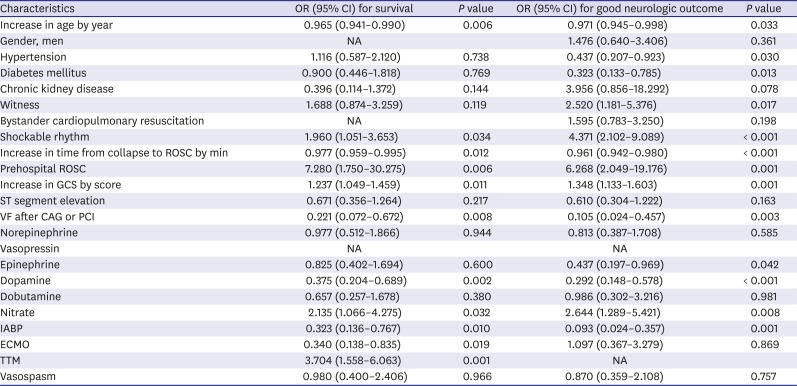
OR = odds ratio, CI = confidence interval, NA = not applicable, ROSC = restoration of spontaneous circulation, GCS = Glasgow Coma Scale, VF = ventricular fibrillation, CAG = coronary angiogram, PCI = percutaneous coronary intervention, IABP = intra-aortic balloon pump, ECMO = extracorporeal membrane oxygenation, TTM = targeted temperature management.
Propensity score matched cohort
After matching the propensity score, each group included 69 patients (Table 4). No variable was significantly different between the vasospasm and stenosis groups and the absolute standard difference in propensity score-matched cohort improved. Survival and good neurologic outcome were not different between the vasospasm and stenosis groups (Fig. 2). Survival analysis with a Kaplan-Meier plot showed similar survival in both groups in propensity score-matched cohort (log-rank P = 0.299) (Fig. 3).
Table 4
Characteristics of out-of-hospital cardiac arrest survivors with coronary vasospasm and coronary stenosis in propensity score-matched cohort
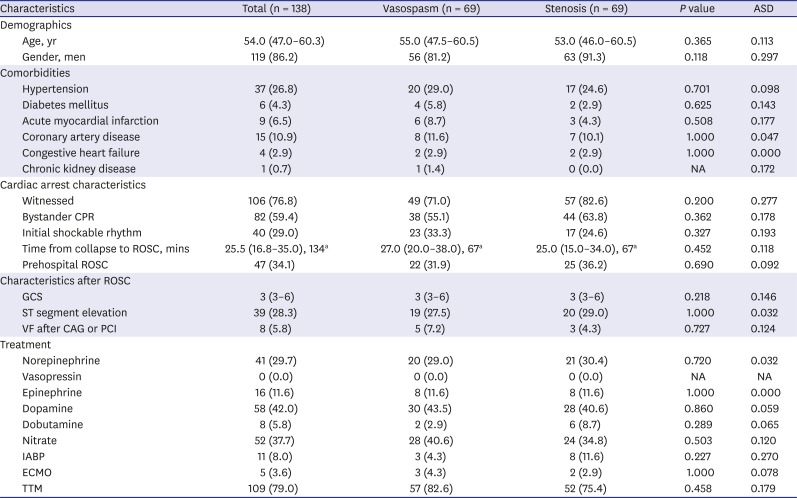
All data presented as median (interquartile range) for continuous variables, and number (%) for categorical variables.
ASD = absolute standardized difference, CPR = cardiopulmonary resuscitation, ROSC= restoration of spontaneous circulation, GCS = Glasgow Coma Scale, VF = ventricular fibrillation, CAG = coronary angiogram, PCI = percutaneous coronary intervention, NA = not applicable, IABP = intra-aortic balloon pump, ECMO = extracorporeal membrane oxygenation, TTM = targeted temperature management.
aIncluded number of patients for analysis.
DISCUSSION
OHCA with vasospasm had affirmative clinical characteristics for survival and good neurologic outcome. However, in the propensity score-matched cohort, OHCA survivors with coronary vasospasm had 30-day survival and neurologic outcomes similar to those of OHCA survivors with coronary stenosis.
Vasospasm-related SCA differs in incidence according to race and is less frequent than SCA associated with acute coronary syndrome.2345 In Tokyo, vasospasm-related OHCA was 11.0% (17/155) in OHCA survivors who underwent CAG.3 In Paris, the incidence of SCA related to vasospasm was 2.0% (31/1,557) in patients with a definite cardiac etiology.5 Nevertheless, in the present study, we reported a higher incidence of 13.1% (89/676) vasospasm-related OHCA survivors among those who underwent CAG than did previous works, indicating that vasospasm-related OHCA incidence might be underestimated. Delayed provocation test for the diagnosis of vasospasm in patients with normal coronary arteries on CAG right after ROSC, is usually performed for safety reasons. However, poor neurologic outcome patients who showed normal coronary arteries on CAG or did not undergo CAG after ROSC might have no further opportunity to undergo a provocation test.18 Therefore, an undiagnosed vasospasm could be underreported, suggesting that the possibility of vasospasm in OHCA survivors should be considered.
Variant angina develops at a younger age than the angina secondary to atherosclerosis and is known not to exhibit classic coronary risk factors.10 Patients with SCA related to vasospasm were younger and less likely to have diabetes mellitus compared to other acute coronary syndromes in a prospective, population-based registry of OHCA.5 We also found similar associations of vasospasm with diabetes and age in the present study (Table 1). Diabetes is a well-known risk factor for development of coronary atherosclerotic changes. Although endothelial dysfunction is a common link between diabetes and vasospasm,1920 diabetes was not independently associated with vasospasm.21 Diabetes is not only a risk factor for occurrence of OHCA but also can mitigate the effect of TTM in cardiac arrest survivors after ROSC.2223 Older age is independently associated with higher mortality and poor neurologic outcome in OHCA and/or in-hospital cardiac arrest survivors.2425 Therefore, a lower incidence of diabetes and younger age seemed to play an important role in better outcomes following vasospasm compared to stenosis in the whole cohort, while the vasospasm and stenotic groups with similar incidence of diabetes and age in the propensity score-matched cohort showed no difference in survival and neurologic outcomes.
Initial shockable rhythm and time from collapse to ROSC are robust prognostic factors contributing to the outcome of cardiac arrest survivors.2627 Coronary vasospasm can also induce life-threatening ventricular arrhythmias due to both transient myocardial ischemia and reperfusion.28 Previous works reported similar shockable rhythms in both vasospasm and non-vasospasm OHCA groups.35 The frequency of shockable rhythm and time from collapse to ROSC was not different between the vasospasm and stenosis groups in the present study. However, our findings demonstrated that the vasospasm group achieved higher prehospital ROSC which is a strong indicator of better outcome in OHCA. Higher prehospital ROSC in the vasospasm group is presumed to contribute to the higher GCS after ROSC, better survival, and better neurologic outcomes 30 days after cardiac arrest in the whole cohort of this study. Under circumstances of emergency medical services which provided only basic life support and defibrillation during the study period,29 the higher prehospital ROSC in the vasospasm group was postulated to be related to the transient myocardial ischemic nature of vasospasm without any structural lesion in the coronary artery. However, on the contrary, the vasospasm and stenotic groups had comparable prehospital ROSC in the propensity score-matched cohort and showed similar clinical outcomes. The lesser ST segment elevation on electrocardiogram in the vasospasm group seems to be associated with lesser ischemic insult to the heart. Our findings demonstrated that lesser requirement of vasopressors, mechanical circulatory support in the vasospasm group is consistent with the assumption of more preserved heart function from ischemic insult than in the stenosis group.5 Likewise, the vasospasm and stenotic groups in the propensity score-matched cohort had no difference in ST segment elevation and circulatory support measures. This might be associated with the insignificant differences in survival and neurologic outcomes.
The adjusted ORs of the vasospasm group versus the stenosis group for 30-day survival and good neurologic outcomes were insignificant in the present study. The difference in the 30-day survival and neurologic outcomes between the vasospasm and stenosis group disappeared after balancing the characteristics between the two groups, as well. The covariates included a logistic regression model, and variables which were balanced through propensity score-matching in the present study are considered as the characteristics of vasospasm. Due to these characteristics, the vasospasm group can be expected to show a better outcome. Vasospasm-related cardiac arrest is generally believed to have better outcome than coronary stenosis-related cardiac arrest.1030 However, the result of the present study suggests that vasospasm-related cardiac arrest itself has a severity equivalent to coronary stenosis-related cardiac arrest. Even if findings such as younger age, lower risk of atherosclerosis, and transient myocardial ischemic characteristics suggest vasospasm-related cardiac arrest, standard post-cardiac arrest care including CAG should be provided in accordance with coronary stenosis.
A previous study showed that the high dose vasopressor was associated with increased mortality in OHCA survivors.31 In line with the previous study, greater use of vasopressors or circulatory supports was associated with increased mortality and poor neurologic outcomes, irrespective of the presence of coronary vasospasm or stenosis in the present study. On the other hand, the association between nitrate and survival or good neurologic outcomes can be explained by the avoidance of nitrate in hypotensive or shock status.
This study has a few limitations. First, we included OHCA survivors who underwent delayed CAG due to the issue of safety for the provocation test. However, survivors with poor neurologic outcomes tended to undergo no further CAG to elucidate the cause of collapse, which may have led to a selection bias. Although the provocation test with acetylcholine or ergonovine is a confirmative diagnostic procedure for coronary vasospasm, not all patients in the vasospasm group were diagnosed using the provocation test. Future studies are warranted on OHCA with presumed cardiac etiology, who routinely received CAG and provocation tests (if required), to elucidate the true incidence of vasospasm-related SCA and the association between coronary pathology and outcomes. Second, we defined > 50% stenosis of the coronary artery as clinically significant stenosis. There is a debate on the threshold value of clinically significant stenosis from 50% to 75%,323334 with 70% stenosis recently accepted as clinically significant. However, we presumed that > 50% coronary stenosis could be causative, because all patients in the present study were OHCA survivors without any obvious extra-cardiac causes. Third, we designated the patients with mixed vasospasm and stenotic lesions based on the dominant pathology, which might have produced bias. Fourth, owing to the retrospective observational study design, we could only identify an association but not causation between vasospasm and clinical outcomes. Fifth, we performed propensity score-matching to balance the intergroup differences. However, intergroup differences could still have been possible. Sixth, although the attending physician provided post-resuscitation care according to the standard protocols of each hospital, the difference in infrastructure among hospitals may be a potential confounding factor. Seventh, we were not able to address the location and severity of coronary vasospasm and treatment, such as calcium channel blocker and implantation of intracardiac defibrillator, due to a lack of data. Eighth, the results generated by the present study cannot be generalized because vasospasm is disproportionately prevalent within Asian—compared to Caucasian—populations. Ninth, we did not analyze the association between details of vasopressors (dose, timing, and retention) and outcomes due to the lack of data.
In conclusion, vasospasm-related OHCA survivors have good baseline and cardiac arrest characteristics, which are responsible for better survival and good neurologic outcome 30 days after cardiac arrest. However, vasospasm-related OHCA survivors have survival and neurologic outcomes similar to stenosis-related OHCA survivors after adjustment or balancing the characteristics.
 XML Download
XML Download