

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Eosinophilic gastrointestinal disorder (EoGID) is a mixed type of gastrointestinal (GI) allergic disease that selectively affect segments of the GI tract with eosinophilic inflammation in the absence of secondary causes for tissue eosinophilia.12
The prevalence of EoGID was reported as 1–30 per 100,000 people in the general population34 and 19.4 per 100,000 people in the pediatric population.5 To date, there has been no data on prevalence of EoGID in children in Asia, including Korea. Although it is assumed to be uncommon compared with Western countries, it is an increasingly emerging condition.6 Previously, prevalence of EoGID was considered very low in Korean children, but recently, it is considered to be more common than previously recognized, and research on this is being actively conducted.78
The occurrence of EoGID tends to be underestimated because its clinical symptoms are nonspecific GI symptoms and endoscopy cannot be performed in all patients with those symptoms, although determining the total number of infiltrating eosinophils per high-power field is essential to the diagnosis. Therefore, noninvasive markers that can reflect the presence of EoGID are needed in practice to screen and diagnose the disease. However, to date, only increased serum levels of total immunoglobulin E (IgE) and hypereosinophilia in the peripheral blood have been suggested to be supportive of the clinical suspicion of EoGID with limitations.9
Fecal calprotectin (FCal) is an intracellular calcium- and zinc-binding protein found in the cytosol of neutrophils with bacteriostatic and fungistatic properties.10 FCal concentration is directly proportional to neutrophil migration toward the GI tract and closely correlates with leucocyte excretion in the feces.1112 Thus, it has been used as a noninvasive biomarker for intestinal inflammation to differentiate organic GI diseases such as inflammatory bowel disease (IBD) from functional abdominal pain disorders (FAPD) in children with chronic GI symptoms.131415 Furthermore, there are some studies on the association between FCal with non-IgE mediated cow's milk allergy, juvenile polyps, and celiac disease. However, no studies have been conducted to clinically apply FCal to EoGID in both adults and children despite its clinical importance.161718
Therefore, this study aimed to evaluate the diagnostic accuracy of FCal for GI inflammation in EoGID patients and to investigate the optimal cutoffs for differentiating EoGID from FAPD in children with chronic GI symptoms.
Go to : 
METHODS
Subjects
Children and adolescents aged ≤ 18 years who underwent upper endoscopy and colonoscopy with biopsies and FCal for chronic GI symptoms at the Department of Pediatric Gastroenterology of the Seoul National University Bundang Hospital were recruited. EoGID and IBD were diagnosed on the basis of clinical, laboratory, radiologic, endoscopic, and histopathologic findings. Children without any evidence of organic disease in above-mentioned evaluations were included in the FAPD group; these children met the ROME IV criteria.19 The FAPD group included patients diagnosed with various conditions such as constipation, functional dyspepsia, irritable bowel syndrome, childhood functional abdominal pain, and abdominal migraine. Those who had a history of previous treatment for underlying disease or a concurrent diagnosis of any other conditions were excluded from the study. The study also excluded patients whose endoscopic finding identified other definite diseases causing chronic abdominal pain or in whom specific infection was confirmed by stool test. Finally, a total of 253 children were recruited, except for 38 patients diagnosed with IBD, and divided into the two groups; 1) EoGID (n = 28) and 2) FAPD (n = 187).
Medical records on demographic data, laboratory test results including FCal levels, and radiologic, endoscopic, and pathologic findings were retrospectively reviewed in all subjects.
Laboratory tests and measurement of FCal levels
Laboratory tests including white blood cell count (WBC), absolute neutrophil count (ANC), eosinophil count, erythrocyte sedimentation rate (ESR), highly sensitive C-reactive protein (CRP), liver function tests, serum amylase, lipase, serum electrolytes, urinalysis and urine cultures, stool examination for parasites, fecal occult blood, stool cultures for bacteria, and the levels of FCal as well as abdominal X-ray and abdominal ultrasonography were performed in all children.
FCal was measured at the initial diagnosis in all subjects using a fluorescence enzyme immunoassay (Calprotectin, Phadia AB, Sweden). The normal range was set at < 50 mg/kg according to the manufacturer's recommendations.
Endoscopic biopsy, histopathology, and diagnosis of EoGID
Esophagogastroduodenoscopy was performed using a GIF-Q260 or GIF-XP260 scope (Olympus, Tokyo, Japan), while colonoscopy was performed using a PCF-Q260AL, GIF-Q260, or GIF-XP260 scope (Olympus).
Endoscopic mucosal biopsies were obtained from the esophagus, gastric antrum and body, duodenum, terminal ileum, cecum, ascending, transverse, descending, and sigmoid colon, and rectum, respectively. Biopsy tissues were immediately fixed in formalin and processed in paraffin wax. Sections were cut at 3 μm and stained with hematoxylin and eosin for histopathologic examination.
Eosinophils were counted in five randomly selected high power fields (HPF). Quantification of eosinophils was performed using an Axioskop40 microscope (Mirax-Carl Zeiss, Oberkochen, Germany) at 400× magnification. Cell counting was performed by two pathologists who were blinded to the patients' statuses, and the average value over the five HPFs was calculated for each subject.
The histopathologic diagnosis of EoGID was made when the total number of infiltrating eosinophils per HPF exceeded 15 in the esophagus, 20 in the stomach and duodenum, and 25 in the colon and rectum. Terminal ileum and cecum were excluded, considering that tissue eosinophils may be present in normal children.20212223
Statistical analysis
Data for continuous variables are presented as mean ± standard deviations for parametric variables. Categorical variables are presented as a percentage of the total number.
Continuous variables were analyzed using Student t-test. The χ2 test was used to compare categorical variables. Pearson correlation analysis was performed to analyze the correlation between FCal and other inflammatory markers. Receiver-operating characteristics plot analysis was used to evaluate optimal cutoff levels of FCal.
For all statistical analyses, a two-sided P value < 0.05 was considered statistically significant. All statistical analyses were performed using PASW Statistics (SPSS version 22.0; SPSS Inc., Chicago, IL, USA).
Ethics statement
This study was approved by the Institutional Review Board of Seoul National University Bundang Hospital (No. B-1707/409-105). The data used for this study did not include any identifiable personal information and informed consent was waived by the board.
Go to :
RESULTS
Patients characteristics
A total of 253 children (122 boys, 131 girls; mean age, 12.2 ± 3.6 years; range, 2.9–17.8 years) were recruited and divided into the FAPD (n = 186) and EoGID (n = 67) study groups. Baseline demographic data and laboratory test results including FCal levels of pediatric patients are listed and compared between the two groups in Table 1.
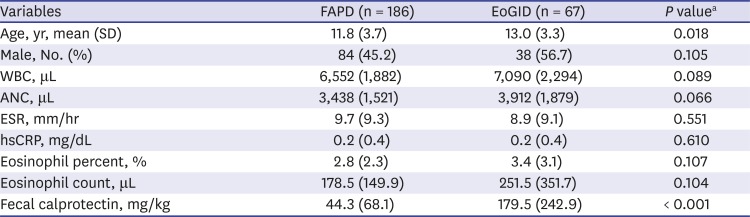
Table 1
Comparison of demographic data and laboratory findings among children with functional abdominal pain and eosinophilic gastrointestinal diseases
FAPD = functional abdominal pain disorder, EoGID = eosinophilic gastrointestinal disorder, SD = standard deviation, WBC = white cell count, ANC = absolute neutrophil count, ESR = erythrocyte sedimentation rate, hsCRP = highly sensitive C-reactive protein.
aP value < 0.05 was set to be statistically significant.
![]()
FCal levels according to underlying gastrointestinal diseases
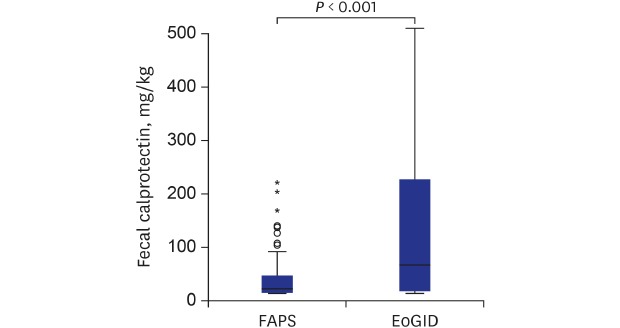
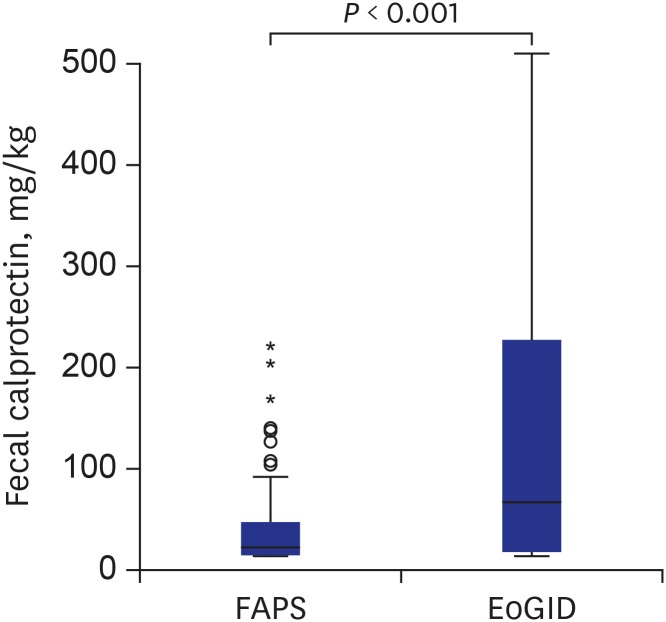
FCal levels were significantly higher in the EoGID group than in the FAPD group (mean, 179.5 ± 242.9 mg/kg vs. 44.3 ± 68.1 mg/kg; P < 0.001) (Fig. 1). WBC, ANC, ESR, CRP, and eosinophil count did not differ between the two groups (all P > 0.05).
Correlation of FCal levels with inflammatory markers
FCal levels weakly correlated with WBC (r = 0.127, P = 0.044), ANC (r = 0.166, P = 0.009), and hsCRP (r = 0.126, P = 0.049) but not with ESR and eosinophil count (both P > 0.05). However, when analyzing in the EoGID group, FCal did not correlate with any inflammatory markers such as WBC, ANC, ESR, CRP, and eosinophil count.
Optimal cutoffs and diagnostic accuracy of FCal
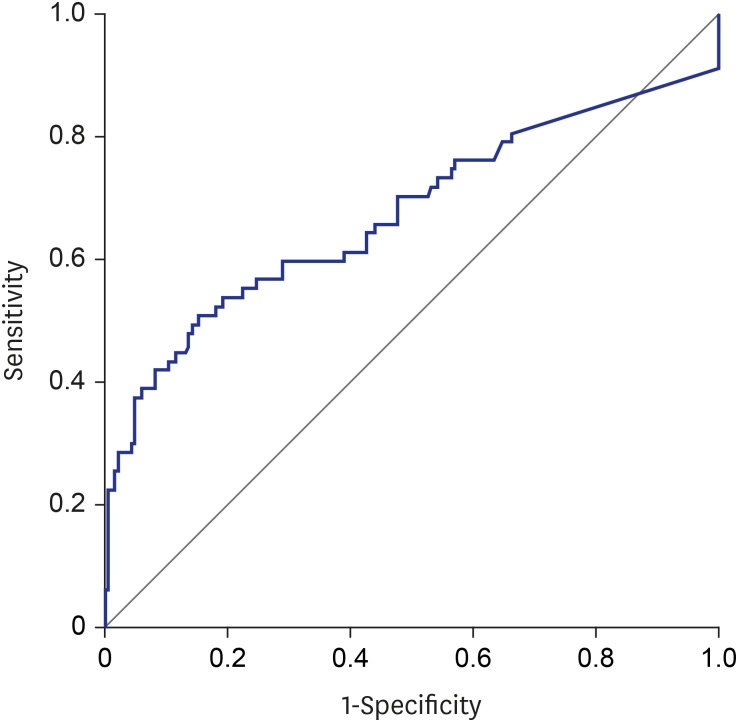
An optimal cutoff of FCal 73.2 mg/kg distinguished EoGID from FAPD with a sensitivity of 50.7% and specificity of 84.6% with an area under the curve (AUC) of 0.672 (95% confidence interval [CI], 0.584–0.759) (Fig. 2).
Go to :
DISCUSSION
The present study is the first to examine the clinical application of FCal measurements for screening and diagnosing EoGID in practice. Our study results revealed that FCal levels significantly increased in pediatric patients with EoGID compared to those with FAPD, which made it possible to distinguish EoGID from FAPD in children manifesting with various GI symptoms.
EoGID causes various chronic GI symptoms such as abdominal pain, nausea, vomiting, early satiety, diarrhea, and weight loss in pediatric patients,21 and it is an important organic disease that should be considered when a patient visits hospital complaining of these symptoms. However, in clinical practice, it is difficult to detect and approach EoGID because its diagnosis requires histopathologic findings through invasive endoscopic biopsy.2021 Unlike FAPD, which does not usually require other specific treatments, appropriate treatment including dietary therapy and, if needed, medications such as montelukast or glucocorticoid therapy should be initiated in patients with EoGID.2024 Without any treatment, symptoms may not improve; in some cases, progress to severe malabsorption, malnutrition, and faltering growth.25 Therefore, it is necessary to properly rule out EoGID before confirming the diagnosis of FAPD in children with chronic GI symptoms.
Although hypereosinophilia in the peripheral blood and possibly increased serum total IgE levels may be supportive of the clinical suspicion of EoGID in some patients, peripheral eosinophil counts or serum total IgE levels can be within normal range in the others.26 Thus, it is not easy to decide whether to perform invasive diagnostic investigations such as endoscopy with biopsies in many cases.
FCal is a clinically useful noninvasive test that reflects GI tract inflammation without being affected by inflammation other than that of the GI tract.131415 Therefore, an increase in FCal can help distinguish FAPD from other organic diseases; if the appropriate cutoff value is suggested, it can be helpful in the diagnosis of certain inflammatory GI diseases such as IBD and EoGID. In patients with EoGID, the exposure to specific food allergens causes tissue eosinophilia of the GI tract, in which eosinophils activate eosinophil-active cytokines that cause GI inflammation.2 Therefore, an increase in FCal can be expected theoretically in EoGID. In our study, FCal levels of the patients with EoGID were significantly different from those of FAPD. Therefore, our study results suggest that the increase of FCal level indicates a higher possibility of the presence of organic GI diseases such as EoGID as well as IBD; thus further evaluations including endoscopy with biopsies should be considered in practice.
The next step of our study was to determine the optimal cutoff values of FCal to differentiate EoGID from FAPD, which revealed that a cutoff of 73.2 mg/kg was optimal for distinguishing EoGID from FAPD with a sensitivity of 50.7% and a specificity of 84.6% at AUC of 0.672. Therefore, based on our study results, the increase of FCal levels beyond the above-suggested cutoff values can assist pediatricians decide whether to perform further diagnostic investigations such as endoscopy with biopsies to diagnose EoGID.
Our analysis also showed a weak positive correlation between FCal and inflammatory markers such as WBC, ANC and CRP. However, this correlation was not significant in each group.
Since WBC and CRP was more closely related to FCal than ESR and peripheral eosinophil count in our study, these may be an additional supportive inflammatory marker for screening patients with chronic GI symptoms.
EoGID has no definitive histological criteria for diagnosis except for eosinophilic esophagitis. Many experts consider 20–25 eosinophils per HPF as a cutoff for normal eosinophil count in the stomach and small bowel. However, the criteria for diagnosis of eosinophilic enteritis and colitis in terminal ileum and colon vary widely from 20 to 50 or more eosinophils per HPF, depending on the study design.20212227 In the present study, we established the diagnostic criteria for EoGID on the basis of previous studies on the eosinophil count of pediatric GI tract and the diagnosis of EoGID including ours.23
Although we tried to establish appropriate diagnostic criteria, the absence of universal histological criteria for the EoGID diagnosis is still a limitation of our study. If further studies and guidelines on the histologic diagnosis of EoGID are made and reliable universal diagnostic criteria are available, it might be useful for the diagnosis of EoGID and related studies. Other limitations of our study are its retrospective design and the fact that the FCal cutoff value had relatively low sensitivity in distinguishing EoGID from FAPD. This may be related to the small number of study subjects with EoGID and that one patient showed an exceptionally high FCal level without any evidence of other organic causes. Nevertheless, our study could present an optimal cutoff that can distinguish EoGID from FAPD in children with a sensitivity of 50.7% and a specificity of 84.6%.
In conclusion, FCal is a useful and reliable noninvasive marker in differentiating EoGID from FAPD in Korean children manifesting with chronic GI symptoms, when optimal cutoffs are applied.
Go to :
 XML Download
XML Download