

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Hospital medicine, a medical field originating in the United States (US), focuses on improving the quality and efficiency of general medical care for hospitalized patients.1 Evidence indicates that hospital medicine can improve various outcomes, including readmission rate, length of stay (LOS), and patient satisfaction.23 As a result, hospitals in the US have rapidly adopted the concept of hospital medicine; with more than 50,000 hospitalists, the field has grown larger than any other subspecialty of internal medicine.4
The need for hospitalists has emerged in Korea because of regulatory changes that limit working hours for training residents, reduction of the training period in internal medicine and general surgery, and because of safety issues with inpatient care.567 Recognizing these imminent problems, hospitalist pilot programs were launched with government initiatives in 2016. Three years after the launch of the programs, more than 120 physicians serve as hospitalists in Korea in 2019.8 A group in Korea showed reduced LOS and emergency department waiting time after the introduction of an acute medical unit operated by hospitalists in a tertiary hospital.9 A recent study also reported that hospitalist-based care is associated with a lower LOS in patients with comorbidity burden by the Charlson comorbidity index (CCI) of with pneumonia or urinary tract infection.10
The variety of hospitalist pilot programs in Korea range from weekday models in which two or more physicians care for inpatient units during weekdays, to full-time, 24-hour and 7-day coverage models in which five or more dedicated doctors work as a hospitalist team.11 With this initial expansion in hospitalist volume, discussions on optimal care models for hospital medicine in Korea are still ongoing. However, to our knowledge, the effects of differing depth of coverage by hospitalists on clinical outcomes remain unknown in Korea. Therefore, this study assessed the effects of the completeness of 24/7 hospitalist services on clinical outcomes in a single inpatient unit of internal medicine in a tertiary academic hospital.
Go to : 
METHODS
Hospitalist work schedules and study population
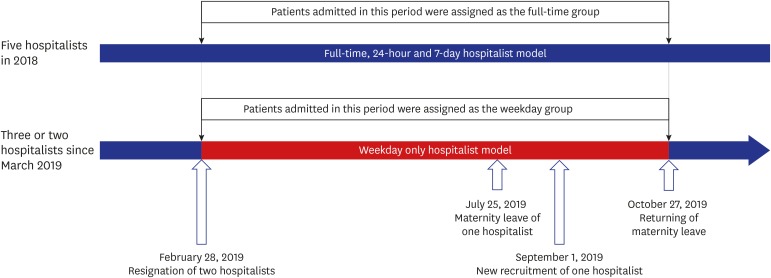
Since March 2017, five hospitalists had been working as a hospitalist team on a 24/7 basis at the hospitalist unit of the Department of Internal Medicine at Seoul National University Hospital. From March 1 to October 27, 2019, two or three hospitalists worked only during weekdays due to two hospitalist vacancies and one maternity leave. Meanwhile, internal medicine board certified physicians in clinical fellowship program affiliated to varying subspecialties cared patients on every weekends of the period. All patients admitted to the hospitalist unit through emergency department after March 1 and discharged before October 27, 2019 were defined as the weekday group. All patients admitted to the same unit in the same period of 2018 were defined as the full-time group. Patients admitted from the outpatient department were excluded from the analysis (Fig. 1).
Data collections and outcome definitions
Data on age, gender, and medical history were collected to calculate CCI scores.12 Information was also collected about which departments in internal medicine were associated with major cause of admission. In-ward mortality, unplanned intensive care unit (ICU) admission, incidence of cardiopulmonary resuscitation, transfer to the specialist, transfer to local hospitals, unexpected readmission within 30 days, and LOS were analyzed as clinical outcomes.
Statistical analysis
The categorical variables “baseline characteristics” and “clinical outcomes” were analyzed using Pearson's χ2 or Fisher's exact tests. Continuous variables were expressed as mean and standard deviation or median and interquartile range. Continuous variables with a non-normal distribution including LOS were analyzed using Mann-Whitney U test. Univariate and multivariate logistic regression analysis were performed to identify independent predictive factors of in-ward morality. Two-tailed P values less than 0.05 were considered statistically significant. All statistical analyses were performed using IBM SPSS Statistics for Windows, version 23.0 (IBM Corp., Armonk, NY, USA).
Ethics statement
This study was approved by the Institutional Review Board of Seoul National University Hospital (approval No. 1910-058-1069). As this study involved a retrospective review of medical records, the requirement for informed consent was waived.
Go to :
RESULTS
Baseline characteristics of the study population
A total of 513 patients were included and 238 patients were assigned to the full-time group. The median age of this group was 65 years (range, 25–98 years) and 137 patients (57.6%) were men. The mean CCI score in this group was 6.5 (range, 0–15 points), and 133 (55.9%) patients were admitted for the treatment of Hemato-oncological problems. No patient was hospitalized for regularly planned chemotherapy, which was not indicated for admission to the hospitalist unit in this hospital. The weekday group included 275 patients with a median age of 65 years (range, 17–103 years). Among the patients in the weekday group, 191 (69.5%) were men. The mean CCI score of this group was 6.5 (range, 0–14 points), and 142 were Hemato-oncological patients (51.6%). The proportion of men was higher in the weekday group than in the full-time group (69.5% vs. 57.6%, P = 0.005). There were no significant differences in age, CCI, departments associated with major problem, or vital signs at admission (Table 1).
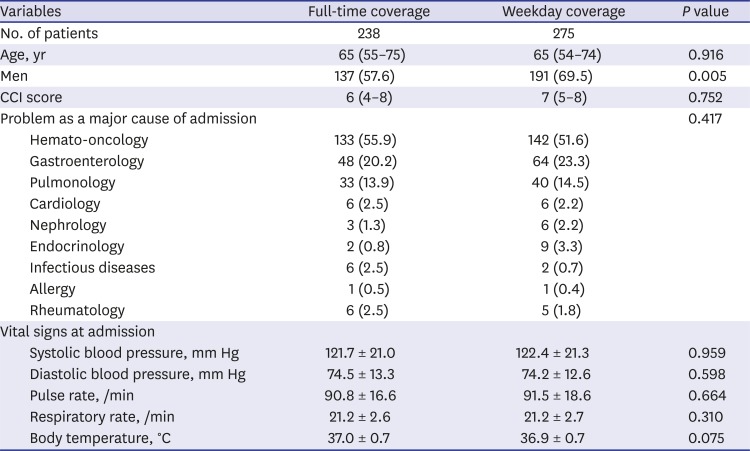
Table 1
Comparison of baseline characteristics according to the completeness of hospitalist coverage
Data are presented as median (interquartile range), mean ± standard deviation, or number (%).
CCI = Charlson comorbidity index.
![]()
Clinical outcomes of the study population
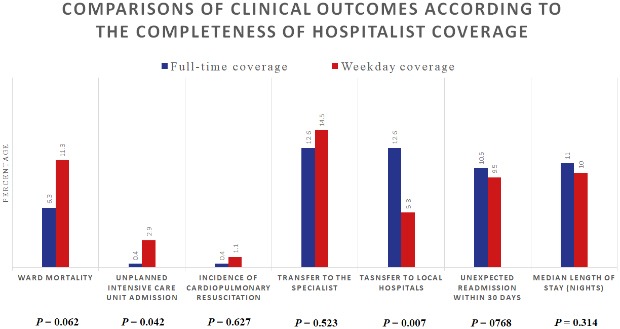
In-ward mortality tented to be lower in the full-time group (6.3%) than the weekday group (11.3%) without statistical significance. Only one patient in the full-time group was admitted to the ICU, while eight patients were admitted to ICU in the weekday group (P = 0.042). A patient with terminal lung cancer in the full-time group was admitted to the ICU at the request of guardians, and died during ICU stay. Of eight patients admitted to the ICU in the weekday group, 7 had terminal cancer, 6 died during ICU stay, and 3 were admitted to the ICU on weekends. Incidence of cardiopulmonary resuscitation were 3 in the weekday group and 1 in the full-time group. Thirty patients (12.6%) in the full-time group were transferred to local hospitals. In contrast, only sixteen patients (5.8%) in the weekday group were transferred to local hospitals (P = 0.007). Of 46 patients who were transferred to other hospitals, 31 patients (67.4%) had terminal cancer. There were no significant differences in unexpected readmission within 30 days and LOS between two groups (Table 2).
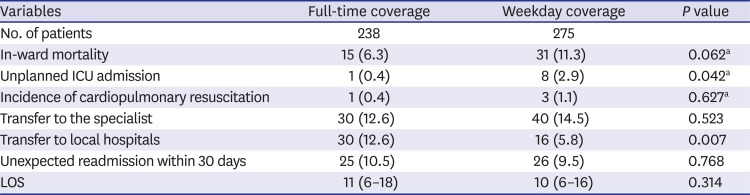
Table 2
Comparison of clinical outcomes according to the completeness of hospitalist coverage
Data are presented as median (interquartile range) or number (%).
ICU = intensive care unit, LOS = length of stay.
aFisher's exact test.
![]()
Predictive factors for in-ward mortality
By univariate logistic analyses for overall study patients, in-ward mortality was significantly associated with Hemato-oncological problem as a major cause of admission, CCI increment, incremental pulse and respiratory rate. Multivariate analysis showed that weekday coverage (odds ratio [OR], 2.00; 95% confidence interval [CI], 1.01–3.99), a one-point increment in CCI (OR, 1.32; 95% CI, 1.14–1.53), and a one-beat per minute increment in pulse rate at admission (OR, 1.03; 95% CI, 1.01–1.06) were independent predictors of in-ward mortality (Table 3).
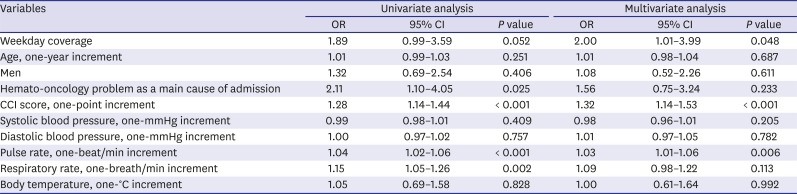
Table 3
Predictive factors for in-ward mortality
![]()
Go to :
DISCUSSION
In this retrospective study, we found that frequency of in-hospital clinical outcomes including mortality and unexpected ICU admission were significantly higher in acutely-ill medical patients admitted through emergency department with partial, weekday hospitalist coverage than with 24/7 hospitalist coverage. In further analysis for factors associated with mortality, comorbidity burden and initial pulse rate were significant after adjustment.
The current hospitalist pilot program provides a predefined fee for patients receiving hospitalist care.13 Although the current fee system includes an incremental subsidy according to the completeness of hospitalist coverage, many hospitals are struggling to recruit hospitalists, especially those who are willing to work on weekends.11 In our experience, a system in which five or more physicians provide full-time coverage for a single unit (35–45 patients) is less sustainable, frequently leading to team-member burn-out and quitting. Indeed, burn-outs leading to quitting without applicants for the empty hospitalist positions resulted in the weekday hospitalist system that we maintained throughout 2019.
In this study, the weekday coverage affected in-ward mortality. A recent large scaled study reported that high hospitalists schedule continuity was associated with lower 30-day mortality after discharge,14 but the literature on in-hospital mortality associated with 24/7 coverage was difficult to find. Most patients (87.0%) who died during their ward stay had terminal cancer as the key reason for mortality in the present study. In patients with serious underlying diseases with obvious grave outcomes, thorough care with frequent communication between attending physicians and patients and caregivers may help overcome barriers in care transition to palliative settings.151617 The results of this study also showed a significantly higher ICU admission in acutely-ill patients, weekday coverage by hospitalists when compared to that in patients with full-time coverage. In view of that most of patients admitted to the ICU had terminal cancer and died during ICU stay, the full-time hospitalist coverage may reduce unnecessary ICU admissions. Therefore, full-time coverage by dedicated hospitalists with seamless discussions and transitions might explain the lower incidence of the mortality during ward stay and unplanned ICU admission. The significantly higher number of transfers to local hospitals in the full-time group also supports this speculation. Systematically incentivizing the full-time coverage system might be beneficial for care-plan decisions and for better care transitions in terminally ill patients.
A number of studies have shown that weekend continuity or 24-hour in house staff coverage are associated with reduced LOS.18192021222324 It is not clear why LOS was not reduced in the full-time group in this study, but there are some reasons that may affect LOS during the weekday coverage period. The first possible reason is a decreases in the total beds of the hospitalist unit in the weekday coverage period. One hospitalist was responsible for 22.5 inpatients during the full-time coverage period and 17 during the weekday coverage period. There was an article on effect of density of hospitalist per occupied bed on LOS.25 Another reason is the fact that after the weekday coverage period began, hospitalists hold a ward meeting and reviewed LOS every month. These factors would have reduced LOS of the weekday coverage group and eventually offset the LOS difference between two groups. The full-time hospitalist coverage will be resumed at the hospitalist unit of the current study. Further research on the factors affecting LOS will be feasible in the near future.
This study has several limitations. As the study was based on retrospective data from patients admitted to a single unit of an academic tertiary hospital, a large proportion of the patients had underlying cancer, restricting the generalizability of the findings. Furthermore, the study was based on a before-and-after design rather than prospective randomization. However, since Korea's hospitalist system is still a pilot program, a prospective study comparing two different hospitalist systems26 would be difficult to perform reliably. After establishment of hospitalist programs in Korea, future studies using nationwide claims-based datasets or in randomized prospective manners might compare the characteristics of varying continuity of hospitalist models.
In conclusion, the completeness of hospitalist coverage was an independent predictive factor of in-ward mortality in acutely-ill patients. In addition, the full-time coverage hospitalist system helped timely care transitions and reduced unnecessary ICU admissions. These observations indicate that the uninterrupted weekend coverage hospitalist service might be helpful for timely care transition from tertiary hospitals that maintain appropriate medical delivery systems. Future studies and establishment of policies for hospitalist programs are warranted for the development of the Korean hospitalist care model.
Go to :
 XML Download
XML Download