

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Neuromyelitis optica spectrum disorder (NMOSD) is a type of demyelinating disorder of the central nervous system (CNS) characterized by optic neuritis, transverse myelitis, or both. Approximately 75%–90% of patients with NMOSD have antibodies against aquaporin-4 (AQP4 Ab), a type of water channel, which is believed to be pathognomonic.1 In general, NMOSD is considered to be a rare inflammatory CNS disease. There have been a few epidemiological studies that have investigated NMOSD worldwide.234567 Several studies have estimated the prevalence of NMOSD in Caucasians, with variations among the studies. The prevalence of NMOSD was reported to be 1.96 per 100,000 persons in Southeast Wales, 0.52 per 100,000 persons in Cuba, and 4.44 per 100,000 persons in Denmark.89 However, there may be differences in the prevalence in Asians due to racial differences.10 In a recent study from New Zealand and Australia, NMOSD was reported to be approximately three times more common in Asians than in other ethnicities (1.57 vs. 0.57 per 100,000 persons).11
Korean studies investigating the prevalence and incidence of NMOSD have not been conducted. Therefore, we investigated the prevalence and incidence of NMOSD in Korea using data from the National Health Insurance (NHI) claims database between 2014 and 2017. Because the NHI database reflects the nationwide real-world medical record, it is very helpful in determining the national prevalence and incidence of certain diseases in Korea. Additionally, we evaluated the relative risk (RR) for age by sex and compared these results with an older age group.
Go to : 
METHODS
Data from the NHI and Health Insurance Review and Assessment Service (HIRA)
The Korea has a mandatory public medical insurance program known as the “NHI,” and each hospital provides patient medical usage lists to the HIRA, which is one of the central government organizations linked to the NHI. HIRA assesses the appropriateness of medical fees and the adequacy of medical services through a medical claims review of each hospital. The patients can select their desired hospital from a range of primary care clinics to tertiary hospitals. The hospital provides an individual medical record to NHI. NHI collects data for each patient, including demographic information, the diagnosis which is represented by a diagnostic code entered by the physician, drug management, and procedures performed by public health in Korea. Therefore, the NHI claims database can provide representative, nationwide healthcare information on specific diagnoses and track patients longitudinally over multiple years.
Identification of NMOSD
Data from the NHI claims database, from 2014 to 2017, were used to select patients with NMOSD. Patients with NMOSD of any age who appeared in the databases between January 2014 and December 2017 were identified and selected. More specifically, patients with NMOSD were defined as those with a primary or secondary diagnostic code of G36.0 according to the Korean Standard Classification of Disease 2015, which is the Korean version of the International Classification of Diseases, 10th Revision, in the departments of neurology, ophthalmology, and pediatrics.
To improve the accuracy of the diagnosis, we combined data regarding prescriptions for immunosuppressants, except oral steroids, after the registration of the NMOSD diagnosis. Data from 2014 to 2017 were obtained. However, the washout period was set from 2014 to 2015 to survey an accurate incidence rate. The incident case was defined as the first entry of the diagnostic code G36.0 (de novo) on admission or from the outpatient medical records for 2016 and 2017, that is, the people who had no previous history of the diagnostic code G36.0.
Population data
Population data for the Korea for 2016–2017 were obtained from the Korean Statistical Information Service (http://kosis.kr/). The total population in Korea in 2016 and 2017 was approximately 50 million. The population was stratified according to sex and grouped into 15-year age intervals. The prevalence and incidence of NMOSD were calculated based on these data.
Estimation of prevalence and incidence
Prevalence is defined as the total number of cases of a disease existing in a specified population at a designated time. The prevalence rate is the total number of cases of a disease existing in a population divided by the total population. Incidence is defined as the number of newly diagnosed cases of a given disease during a given period in a specified population. The crude prevalence for each year (2016 and 2017) was calculated, and patients with NMOSD were analyzed according to sex and age at which the diagnostic code of NMOSD was entered. Furthermore, the annual crude incidences in 2016 and 2017 were calculated. The washout period was set from 2014 to 2015. Incident case was defined as the first entry of the diagnostic code NMOSD in the medical records in 2016 and 2017. Finally, standardized incidence and prevalence rates, adjusted for sex and age, were calculated using population census data for 2016 and 2017, which were obtained from the Korean Statistical Information Service in the Korea National Statistical Office. Depending on the age at which the diagnostic code was entered, the included patients were divided into 5 groups according to the following intervals: < 15; 15–29; 30–44; 45–59; and ≥ 60 years.
The prescribed immunosuppressive agents were described from the NHI database. We analyzed the prescribed data of the immunosuppressive agents, which included azathioprine, cyclosporine, mycofenolate mofetil, rituximab, methotrexate, and mitoxantrone. Oral steroids were not included.
Statistical analysis
The χ2 test was used to compare the prevalence and incidence according to sex and the diagnostic code entered age group. The RR of each age group was assessed and compared with the older (≥ 60 years) group. The group under 15 years of age was not included in the RR statistical analysis because of the small number of patients in this group. Data with 95% confidence intervals (CIs) that did not contain 1 in RR and differences with a P value < 0.05 were considered statistically significant in all analyses. All statistical analyses were performed using SAS Enterprise Guide 7.1 (SAS Institute Inc., Cary, NC, USA) and SPSS version 20.0 (IBM Corporation, Armonk, NY, USA).
Data availability statement
Data can be shared on request by directly contacting the corresponding author.
Ethics statement
This study was approved by the Institutional Review Board (IRB) of Korea University Guro Hospital (IRB No. 2017GR0166). Given the retrospective nature of the study and the use of anonymized patient data, the requirement for informed consent was waived.
Go to :
RESULTS
Prevalence and incidence
A total of 2,390 NMOSD cases in 2016 and 2,410 cases in 2017 were identified according to the diagnostic code (G36.0). Data for 2014 and 2015 were excluded for accuracy to identify incident cases. Patients with a documented prescription for immunosuppressants, except oral steroids, and who had a diagnosis of NMOSD were selected. Ultimately, data of 1,676 cases in 2016 and 1,776 in 2017 were extracted and used to calculate the prevalence of NMOSD in Korea.
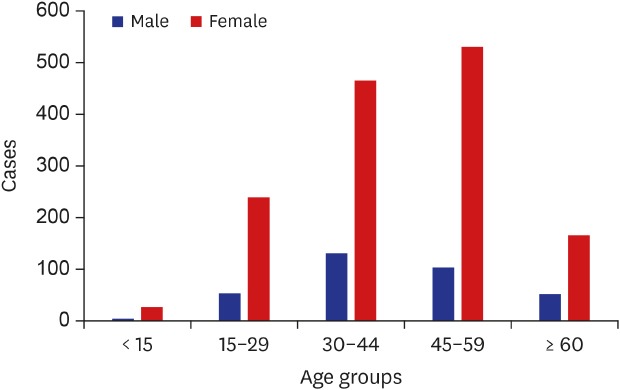
The prevalence and incidence rates for NMOSD in Korea for 2016 and 2017 were calculated. In 2016, the overall prevalence rate was 3.36 per 100,000 persons, and the incidence rate was 0.65 per 100,000 person-years. In 2017, the overall prevalence rate was 3.56 per 100,000 persons, and the incidence rate was 0.41 per 100,000 person-years. The data from 2016 and 2017 were analyzed according to age and sex considering the recent criteria revision for diagnosing NMOSD. Prevalence and incidence rates according to age and sex are summarized in Table 1. The prevalence and incidence of NMOSD were higher in female individuals than in male individuals (male:female ratio, 1:4.69 in incident cases; 1:4.11 in prevalent cases). In prevalent cases for 2017, the mean ages were 43.7 (standard deviation [SD], 14.3) years for the male group and 43.1 (SD, 14.1) years for the female group, and there was no significant difference relating to sex (P = 0.53). Age-specific prevalences in 2017 are shown in Fig. 1. The prevalence and incident rates in individuals aged between 30 and 59 years when the diagnostic code was entered were higher than the overall prevalence and incidence rates. Additionally, they were extremely low in individuals aged < 15 years. Both male and female individuals exhibited similar tendencies. However, these tendencies were more pronounced in female individuals.

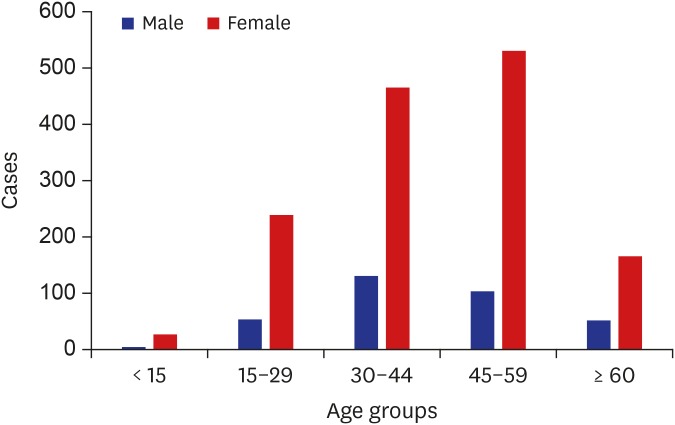 | Fig. 1Age-specific prevalence in Korea in 2017. The prevalence in individuals aged between 30 and 59 years was higher than the overall prevalence.
|
Table 1
Prevalence and incidence of NMOSD in Korea in 2016 and 2017
NMOSD = neuromyelitis optica spectrum disorder.
aAge means the age at which the diagnostic code for NMOSD was entered.
![]()
Treatment state of immunosuppressive agents
We analyzed the prescription status of immunosuppressive agents from claim data in 2017. The most commonly used drugs were azathioprine (38%) and mycophenolate mofetil (19%). Nine percent of the extracted patients were treated with rituximab, and about 5% of the patients were prescribed other immunosuppressants such as tacrolimus, mitoxantrone, and methotrexate.
RR compared with the older diagnostic code entered age group
The incidence of NMOSD was higher in female individuals aged between 30 and 59 years than in female individuals in the older diagnostic code entered age group (≥ 60 years): RR, 2.82 (95% CI, 1.70–4.69) for those aged 30–44 years; RR, 3.05 (95% CI, 1.86–4.99) for those aged 45–59 years. However, such differences were not found among the male diagnostic code entered age groups (Table 2 and Fig. 2).

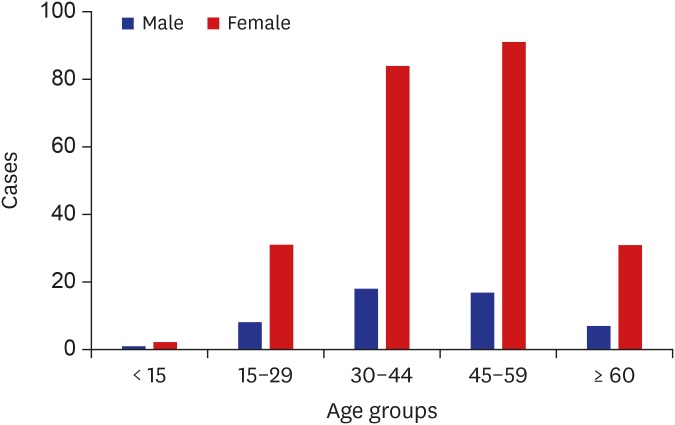 | Fig. 2Age-specific incidence in Korea in 2017. The incidence of NMOSD was higher in females aged between 30 and 59 years compared with females in the older age group (≥ 60 years). However, such differences were not found among males.NMOSD = neuromyelitis optica spectrum disorder.
|
Table 2
NMOSD incidence in younger age groups compared with older age group in 2017
NMOSD = neuromyelitis optica spectrum disorder, RR = relative risk, CI = confidence interval.
aAge means the age at which the diagnostic code for NMOSD was entered.
![]()
Go to :
DISCUSSION
This population-based study was the first to investigate the prevalence and incidence of NMOSD in Korea using data from the NHI database. We estimated the prevalence of NMOSD to be 3.36 and 3.56 per 100,000 persons and the incidence of NMOSD to be 0.41 and 0.65 per 100,000 person-years in 2016 and 2017, respectively.
The prevalence reported in the current study was higher than that reported in previous studies from New Zealand and Australia in Asian individuals (prevalence, 1.50 per 100,000 persons), Southeast Wales (United Kingdom) (prevalence, 2 per 100,000 persons), and Isfahan, Iran (1.9 per 100,000 population). However, the prevalence was consistent with that reported in recent studies from the United States, India, and Cuba.8111213 Although these differences were concordant with ethnic variations, these estimates were lower than those published in several previous population-based studies for Caucasian or Afro-Caribbean individuals (prevalence, 4.4 per 100,000 incidence; 0.4 per 100,000).121415 Additionally, this prevalence was higher than that in a study from southern Japan (1.64 per 100,000) and equivalent to the prevalence of NMOSD in northern Japan (4.1 per 100,000).1617 Our incidence was consistent with that reported in previous results from other countries with similar prevalence rates.2345671218 This result should be confirmed in further follow-up studies, considering that the diagnostic criteria for NMOSD has recently been revised. The results of several studies to date regarding the worldwide prevalence and incidence of NMOSD are summarized in Table 3.
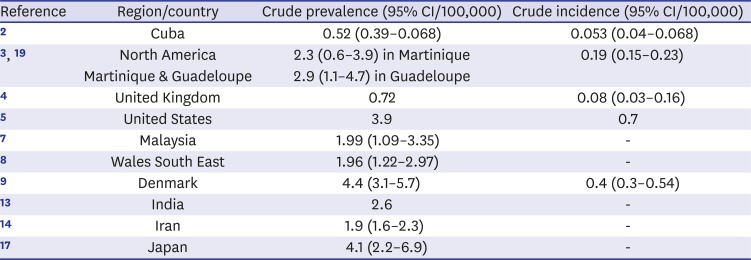
Table 3
Prevalence and incidence studies investigating neuromyelitis optica spectrum disorder
| Reference | Region/country | Crude prevalence (95% CI/100,000) | Crude incidence (95% CI/100,000) |
|---|---|---|---|
| 2 | Cuba | 0.52 (0.39–0.068) | 0.053 (0.04–0.068) |
| 319 | North America | 2.3 (0.6–3.9) in Martinique | 0.19 (0.15–0.23) |
| Martinique & Guadeloupe | 2.9 (1.1–4.7) in Guadeloupe | ||
| 4 | United Kingdom | 0.72 | 0.08 (0.03–0.16) |
| 5 | United States | 3.9 | 0.7 |
| 7 | Malaysia | 1.99 (1.09–3.35) | - |
| 8 | Wales South East | 1.96 (1.22–2.97) | - |
| 9 | Denmark | 4.4 (3.1–5.7) | 0.4 (0.3–0.54) |
| 13 | India | 2.6 | - |
| 14 | Iran | 1.9 (1.6–2.3) | - |
| 17 | Japan | 4.1 (2.2–6.9) | - |
![]()
The prevalence of multiple sclerosis (MS) was estimated to be 3.5 per 100,000 individuals in a previous study from Korea.19 In the United States, the prevalence of NMOSD is estimated to be approximately 1%–2% of that of MS.12 These data are not concordant with the results of the present study. However, it is important to consider racial differences. According to the results of a recent study, non-white patients with NMOSD tended to have a younger onset, more likelihood of a cerebral syndrome, and more severe disability than white patients.10 These racial differences may be influenced by the ratio of NMOSD to MS in Korea. Additionally, it is important to be aware that the previous Korean study was not only based on data from 2000 to 2005 and verified cases from major referral hospitals, but the differential diagnosis of NMOSD was unclear at that time owing to uncertainties with testing for AQP4 antibodies. Therefore, it was estimated that the prevalence was calculated without a clear distinction between MS and other demyelinating diseases such as NMOSD. A further follow-up study on MS may be needed to more clearly establish the ratio of MS and NMOSD in Korea. In recent published study, the prevalence of NMOSD patient was estimated 2.56 in 2016. We included the patients enrolled in secondary diagnosis, which may be overestimated, although we have used the history of drug. However, other study also may have been underestimated because they excluded people who once visited the clinic with NMOSD.20
In this study, higher prevalence and incidence were observed in individuals aged between 30 and 59 years when the diagnostic code was entered than in those aged > 60 years. NMOSD was extremely rare in individuals aged < 15 years. The rarity of childhood incidence of NMOSD was also observed in previous studies on the incidence of CNS demyelinating diseases in a multiethnic cohort of children.20 Our incidence result was reasonable in the group aged < 15 years when the diagnostic was entered. In the sub-analysis according to age, the incidence rates were higher in female individuals aged between 30 and 59 years than in those from the older age group (RR, 2.82 [95% CI, 1.940–4.340) for those aged 30–44 years; RR, 3.05 [95% CI, 1.845–4.170] for those aged 45–59 years). This was not observed in male individuals. These differences may be because of the effects of female hormones. We evaluated the risk of incidence in the groups of fertile female individuals compared with non-fertile postmenopausal elderly patients. Although the fertile women groups showed a higher risk of incidence, there was a possibility of other causes, besides female hormone exposure, considering the mean age of menarche was 12.7 years and that menopause developed at 49.3 years of age in Korean.1213141516171819202122232425
About 60% of NMOSD patients used azathioprine and mycophenolate mofetil, although there are overlapping patients owing to drug changes. According to the medical fee standard of HIRA in Korea, patients could be treated with secondary line therapy such as rituximab in refractory cases for first-line therapy. Therefore, most patients had no choice but to use azathioprine or mycofenolate mofetil. The efficacy of both drugs was not different in NMOSD.26
Our study had several limitations owing to the use of the NHI claims data. First, it was possible that the primary or secondary diagnosis of NMOSD was miscoded (i.e., other than G36.0). We could not access any clinical information, including the results of laboratory tests, such as that for the AQP4 antibody, or imaging studies such as magnetic resonance imaging. Therefore, we used a prescription for immunosuppressant(s) as an additional inclusion criterion to increase the validity of NMOSD diagnosis. Nevertheless, we may have underestimated the prevalence and incidence of NMOSD. In our study, NMOSD patients without a drug prescription may have been excluded because of our operational definition considering the use of immunosuppressant prescriptions except for oral steroid agents. However, approximately 96%–98% of patients with NMOSD were treated with immunosuppressive agents in a recent study involving several ethnicities.10 Third, the incidence may have been overestimated owing to revisions of the NMOSD criteria in 2015.27 However, we have found it more beneficial to use up-to-date data to identify recent trends in the prevalence and incidence of NMOSD in Korea. Furthermore, because the government has recently expanded coverage for NMOSD patients in Korea, there is a risk that the prevalence and incidence will be overestimated. Further follow-up longitudinal studies are needed to overcome these limitations. Finally, data from the NHI claims database do not specify the age at onset, but rather the age at diagnosis and do not include mortality-related information. However, the NHI claims database has merits in that it completely covers the entire population of Korea despite the limitations mentioned above.
This study was the first population-based investigation of the prevalence and incidence of NMOSD in the Korea using data from the NHI claims database. Nationwide prevalence of NMOSD in Korea was 3.36 and 3.56/100,000 and its incidence was 0.41 and 0.65/100,000-year in 2016 and 2017 respectively. We demonstrated that NMOSD is a rare disease in Korea and hope to perform further studies, including other epidemiologic features, in the future.
Go to :
 XML Download
XML Download