

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The traditional goal of treating Crohn's disease (CD) in the past was to improve symptoms and to obtain clinical remission. However, inflammation can still persist despite the absence of symptoms, and many patients experience complications such as intestinal stricture and perforation.1 Moreover, clinical symptoms do not always correlate with the disease activity observed on endoscopy.2 Therefore, mucosal healing (MH) has emerged as a major therapeutic goal, and is expected to modify the natural course of CD.23 Achieving MH in CD is now well known to prevent bowel damage and improve the long-term outcome of the disease.456
Adalimumab (ADL) is a human monoclonal antibody that inhibits tumor necrosis factor (TNF). ADL has shown efficacy in inducing and maintaining clinical remission in a broad population of CD patients including naïve patients, as well as those who have failed to respond to other anti-TNF drugs.78910 Recent studies suggest that therapeutic drug monitoring (TDM) of anti-TNF agents is associated with improved clinical outcomes.1112 High trough levels (TLs) of anti-TNF inhibitors and low levels of anti-TNF antibodies are associated with superior clinical and endoscopic outcomes.1314 Some studies have identified an association between TLs of infliximab (IFX) and MH in CD.15161718 In contrast, there are limited data regarding MH and TDM in pediatric CD patients on ADL treatment. Moreover, the association between TDM of ADL and histologic remission (HR) has not yet been investigated in pediatric CD patients.
Therefore, we aimed to investigate the associations between ADL TLs and MH and between ADL TLs and HR after 16 weeks of consistent ADL treatment in pediatric CD patients.
Go to : 
METHODS
Patients and study design
This study was a prospective cohort conducted at the Department of Pediatrics, Samsung Medical Center, between January 2016 and December 2017. Subjects included in this study were pediatric patients diagnosed with moderate-to-severe luminal CD under the age of 19 who were naïve to biologics. Patients who required treatment with biologics after treatment failure with conventional drugs (‘step-up’ treatment) or those requiring biologics upfront at diagnosis due to the presence of high-risk factors of poor outcomes (‘top-down’ treatment) were the indications for treatment with ADL.319
Patients were excluded from the study based on the diagnoses of inflammatory bowel disease (IBD) unclassified, mild disease activity at diagnosis, coexisting perianal fistulizing disease requiring surgery, and age 19 years or above at ADL. CD was diagnosed in accordance with the European Society for Pediatric Gastroenterology, Hepatology, and Nutrition-revised Porto criteria.20 In accordance with the Pediatric Crohn's disease Activity Index (PCDAI), patients were classified as moderate-to-severe CD based on a score of 30 points or more at diagnosis.21 Disease classification and behavior were based on the Paris classification.22
At the time of diagnosis, baseline clinicodemographic data including sex, birth date, disease classification, growth indicators, prior history of surgery of the gastrointestinal tract or anal fistulas, and family history of IBD were recorded. Then, after initiation of ADL and 16 weeks later, a physical examination, PCDAI scores, growth indicators, and laboratory exams including complete blood cell counts with differential counts, chemistry profiles, erythrocyte sedimentation rate, and C-reactive protein (CRP) levels were conducted. Clinical activity assessments and laboratory examinations including analyses for ADL TLs and antibody to adalimumab (ATA) levels were also performed simultaneously. Quantitation of serum ADL TLs and qualification of ATA positivity were measured at 16 weeks using commercial enzyme-linked immunosorbent assay kits from Matriks Biotek Laboratories (Ankara, Turkey).
Ileocolonoscopy was performed at 16 weeks after ADL initiation, and the Simple Endoscopic Score for Crohn's disease (SES-CD) was assessed to evaluate the degree of mucosal involvement.23 Ileocolonoscopic biopsies were taken from sites where ulcers or lesions were present prior to ADL treatment at each ileocolonic segment; terminal ileum, cecum, ascending colon, transverse colon, descending colon, sigmoid colon, and rectum.
ADL was administered subcutaneously based on a scheduled induction regimen that was determined based on the weight of the patients 160/80 for patients ≥ 40 kg, and 80/40 mg for patients < 40 kg in the first two weeks. Thereafter, patients ≥ 40 kg received 40 mg, and patients < 40 kg received 20 mg every two weeks. Interval shortening to one week was allowed when a loss of response occurred. The decision of concomitant azathioprine (AZA) during ADL treatment was based on each patient's previous treatment prior to ADL initiation. AZA was continued concomitantly with ADL in those who had been receiving AZA prior to ADL, while those who were not on AZA prior to ADL initiation did not receive AZA further on during the study period.
Outcome measures and definition
The primary outcome of this study was MH at 16 weeks from baseline ADL initiation. The secondary outcome was HR at 16 weeks from ADL initiation. MH was defined as an SES-CD = 0, which corresponds to complete healing of the mucosa to normal, clear of any ulcers or other mucosal lesions such as erosion and inflammation. HR was defined as the complete absence of microscopic inflammation in biopsy specimens. Clinical remission was defined as a PCDAI < 10 points and laboratory remission was defined as a CRP < 0.5 mg/dL.
Statistical analysis
For statistical comparison between groups, a Student's t-test or Wilcoxon rank-sum test was used for continuous variables, and a χ2 test or Fisher's exact test was used for categorical variables. Comparative data for continuous variables were reported as medians (interquartile range [IQR]) or means ± standard deviation. Receiver operating characteristic (ROC) curve analysis was performed to derive the best cut-off point for ADL TL, stratifying patients with and without MH. All analyses were performed using the R software (version 3.2.3; R Foundation. Vienna, Austria).
Ethics statement
This study was approved by the Institutional Review Board of Samsung Medical Center and was conducted in accordance with the Declaration of Helsinki (approval No. 2015-10-068-002). Informed consent was obtained from the patients and guardians.
Go to :
RESULTS
Baseline characteristics
A total of 17 patients met the inclusion and exclusion criteria and were included in this study. The baseline clinicodemographic characteristics of all patients are reported in Table 1. The mean diagnosis age of the patients was 14.1 ± 2.0 years. The mean age at ADL initiation was 14.5 ± 2.2 years, and the median duration from diagnosis to ADL treatment was 0.16 years (IQR, 0.08–0.18 years). Fifteen patients (88.2%) started ADL treatment within three months of diagnosis. Twelve patients (70.6%) had been receiving concomitant AZA treatment.
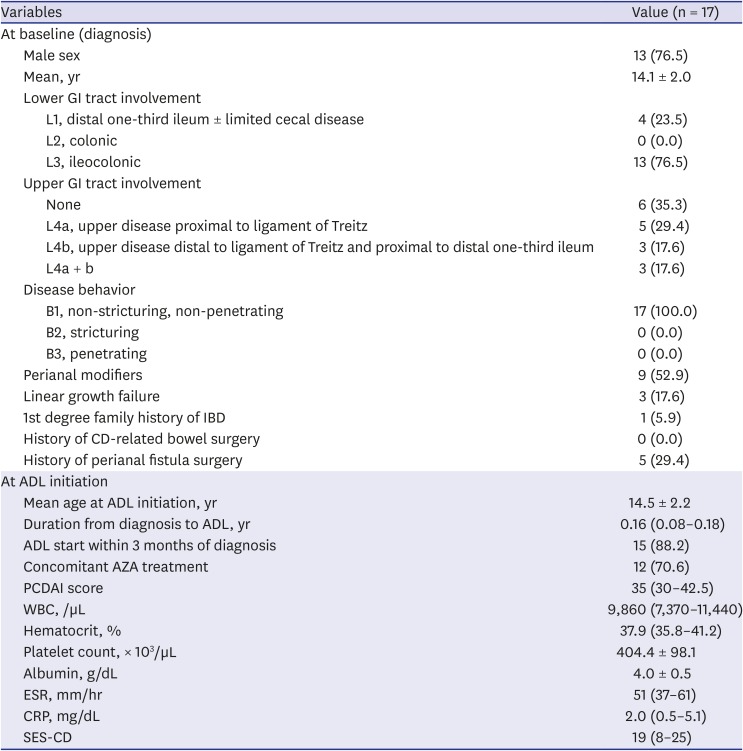
Table 1
Baseline clinicodemographic characteristics
Data are presented as mean ± standard deviation, median (interquartile range) or number (%).
ADL = adalimumab, AZA = azathioprine, CD = Crohn's disease, CRP = C-reactive protein, ESR = erythrocyte sedimentation rate, GI = gastrointestinal, IBD = inflammatory bowel disease, PCDAI = Pediatric Crohn's disease Activity Index, SES-CD = Simple Endoscopic Score for Crohn's disease, WBC = white blood cell.
![]()
ADL TLs according to MH and HR status
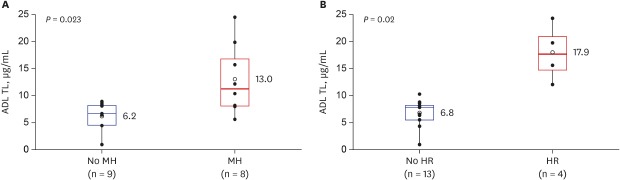
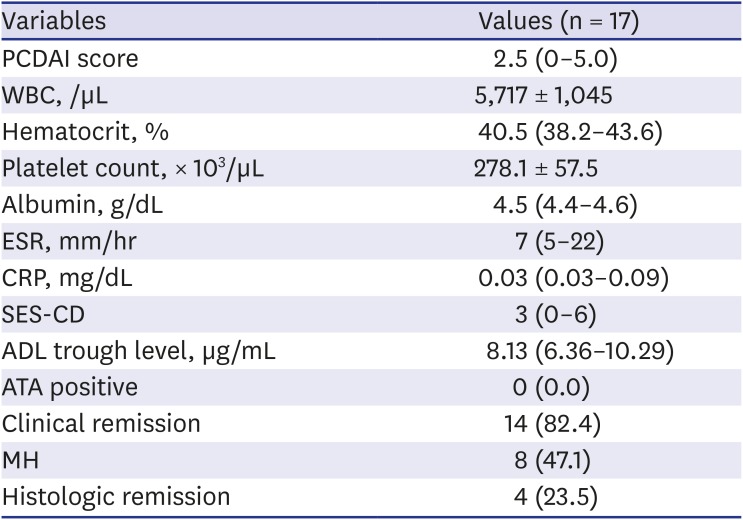
At 16 weeks from ADL initiation, 14 (82.4%), 8 (47.1%), and 4 (23.5%) patients achieved clinical remission, MH, and HR, respectively. All results from the 16-week follow-up visits are summarized in Table 2. ADL TLs were compared between patients with endoscopic MH and patients without MH. ADL TLs were significantly higher in patients who achieved MH than in those who did not (13.0 ± 6.5 vs. 6.2 ± 2.6 μg/mL, P = 0.023) (Fig. 1A). Higher ADL TLs were also associated with HR. ADL TLs were significantly higher in patients who achieved HR than in those who did not (17.9 ± 5.3 vs. 6.8 ± 2.5 μg/mL, P = 0.02) (Fig. 1B).
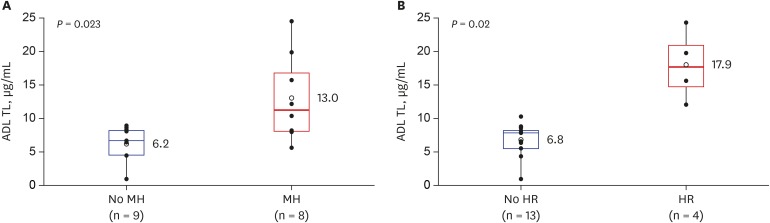 | Fig. 1ADL TLs according to MH and HR status. (A) Comparison for ADL TLs between CD patients with MH and those without MH (P = 0.023). (B) Comparison for ADL TLs between CD patients with HR and those without HR (P = 0.02).ADL TL = adalimumab trough level, CD = Crohn's disease, MH = mucosal healing, HR = histologic remission.
|
Table 2
Outcomes and results at 16 weeks follow-up
Data are presented as median (interquartle range), mean ± standard deviation or number (%).
ADL = adalimumab, ATA = antibody to adalimumab, CRP = C-reactive protein, ESR = erythrocyte sedimentation rate, PCDAI = Pediatric Crohn's disease Activity Index, SES-CD = Simple Endoscopic Score for Crohn's disease, WBC = white blood cell, MH = mucosal healing.
![]()
Relationship between concomitant AZA, ADL TL, and outcomes
ADL TLs did not significantly differ between patients receiving combination treatment with AZA and those receiving ADL monotherapy (median, 8.52 [IQR, 8.01–8.76] vs. 8.00 [IQR, 5.96–11.19] μg/mL; P = 0.799). MH was observed in 50% (6/12) and 40% (2/5) of patients who had and had not received concomitant AZA, respectively (P = 1.000), and HR was observed in 25% (3/12) and 20% (1/5) of patients who had and had not received concomitant AZA, respectively (P = 1.000).
ROC curve of ADL TL in predicting MH
We sought to determine the optimal ADL TL associated with MH. The ROC curve was used to identify the optimal cut-off value for ADL TLs for predicting MH (area under the curve [AUC], 0.819; P < 0.001). According to the ROC analysis, the optimal cut-off value for predicting MH was 8.76 μg/mL (sensitivity, 62.5%; specificity, 100%; positive predictive value, 75%; negative predictive value, 100%) (Fig. 2).

Go to :
DISCUSSION
This study is the first to investigate the associations between ADL TLs and MH, and between ADL TLs and HR at 16 weeks from ADL treatment in the pediatric CD patient population. We showed that ADL TLs were significantly higher in patients who achieved MH compared to those who did not (P = 0.023). This suggests that higher ADL TLs increases the likelihood of achieving MH. We were also capable of observing an association between ADL TLs and HR at week 16.
There is growing evidence that TDM of anti-TNF agents is associated with improved clinical outcomes. A post hoc analysis of the CLASSIC I trial showed that median ADL TLs were significantly higher in patients who achieved clinical remission than those who did not at week 4 (8.10 vs. 5.05 μg/mL, respectively; P < 0.05).24 Another study reported a cut-off ADL level of 5.85 μg/mL yielded optimal sensitivity, specificity and positive likelihood ratio for the prediction of remission (68%, 70.6% and 2.3, respectively).25 A recent analysis from the IMAgINE-1 study in pediatric patients with CD also identified a positive association between serum ADL concentration and remission/response.26 There is also evidence in literature that higher ADL TLs are associated with an increasing rate of MH. Roblin et al.27 demonstrated MH in a cohort of 40 IBD patients receiving maintenance treatment with ADL when ADL TLs were greater than 4.9 μg/mL. Ungar et al.11 showed that ADL TLs higher than 7.1 μg/mL predicted MH in IBD patients with 85% specificity during maintenance treatment. Similarly, Zittan et al.14 demonstrated that higher ADL drug levels during maintenance-ADL treatment were significantly associated with MH when compared with the non-MH group. While most studies investigated the association between ADL TL and MH during maintenance ADL treatment, a recent study revealed that short-term MH at week 4 from ADL initiation was also significantly higher in ulcerative colitis patients who had ADL TLs ≥ 9.4 μg/mL.28 Similarly, our study found that ADL TL of 8.76 μg/mL was the best cut-off point to stratify patients with or without MH. The difference of cut-off levels between studies may differ due to the heterogeneity in the study population, the point of investigation, and other factors. However, a consistent conclusion is that higher TLs of ADL are required in order to achieve MH at any treatment point. Therefore, TDM may guide in optimizing drug levels proactively in order to better achieve the goal of MH in the treat-to-target era.293031
Although there is debate regarding the application of proactive dosing of biologics in real-life practice, a recently published randomized clinical trial by Assa et al.32 revealed that proactive dosing of ADL resulted in significantly higher rates of corticosteroid-free clinical remission than reactive dosing in children with CD. However, limitations of that study are that the therapeutic TL was targeted at a rather low level 5 μg/mL, and MH was not investigated as an endpoint. Meanwhile, the results of our study suggest that in order to achieve MH, higher TLs are required in children with CD receiving ADL. Moreover, considering that MH was investigated 16 weeks after ADL initiation, the results of our study may potentially guide in proactively optimizing dosing in the early stages of ADL therapy.
Histological signs of inflammation still exist in many patients whose endoscopic appearances are normal. There is also limited evidence in literature on the association between TDM and HR. In our study, higher ADL TLs were also associated with HR (P = 0.02). These results are consistent with findings of Yarur et al.13 who showed that mean serum ADL TLs were lower in IBD patients with histological and endoscopic inflammation (9.2 vs. 14.1 μg/mL, P = 0.03, and 8.5 vs. 13.3 μg/mL, P = 0.02, respectively). In addition, attaining HR required higher ADL TLs compared to that of MH (7.8 μg/mL [AUC, 0.76; sensitivity, 61%; specificity, 95%; P = 0.04] vs. 7.5 μg/mL [ROC, 0.73; sensitivity, 62%; specificity, 83%; P = 0.02]). Based on these findings, a higher ADL TL seems to be required to achieve HR than that required for MH.
There is controversy whether concomitant immunomodulators should be continued in CD patients who start treatment with ADL after failed immunomodulator therapy. A recent meta-analysis concluded that the continued use of immunomodulators after starting anti-TNF treatment is no more effective than anti-TNF monotherapy in the aspects of inducing or maintaining response or remission in patients with CD.33 Meanwhile, in another recently published meta-analysis combination treatment with immunomodulators were associated with the reduced risk of antibody formation against anti-TNF agents in patients with IBD.34 Recently, a randomized controlled trial in patients with CD receiving treatment with ADL reported that the clinical efficacy of concomitant AZA during treatment with ADL at week 26 did not differ from that of ADL monotherapy, while those who had received combination therapy showed a significantly higher rate of endoscopic improvement.35 Furthermore, in a post hoc analysis of that study ADL in combination with AZA was shown to increase ADL TLs which was associated with endoscopic response and MH at weeks 26 and 52.36 However, findings in our study were inconsistent with the results of that study, possibly due to the small number of patients in ours.
Likewise, there are several limitations to our study, such as the small number of patients and short term period of the study. Further large-scale studies with long term outcomes may better elucidate the results of our current study. Another limitation is that selection bias may have been introduced. Because the effect of ADL on perianal fistulizing CD in children has been elucidated only recently, some patients with coexisting perianal fistula may have been not enrolled in this study but to receive IFX instead based on the decision of the investigator.37 Although patients with perianal fistulizing disease requiring surgery were excluded, 52.9% of patients with moderate-to-severe luminal CD with perianal fistulizing disease were included in our study as coexisting perianal fistulizing disease at diagnosis is a distinct feature of pediatric CD in Korean children when compared to their European counterparts.38 However, this is still lower than our previous study in pediatric CD patients receiving IFX in which 61.8% of patients had coexisting perianal fistulizing disease.39 Therefore, selection bias may have been introduced during patient enrollment.
In conclusion, serum ADL TLs at 16 weeks after ADL initiation were significantly higher in pediatric patients with CD who achieved MH or HR compared to those who failed to achieve each outcome. Future relevant large-scale studies may guide in predicting short-term MH and HR in the era of treat-to-target.
Go to :
 XML Download
XML Download