

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Total hip arthroplasty (THA) is generally considered to be one of the most successful and frequently performed orthopedic surgical procedures.12 Although many previous studies have reported good results of THA, various studies are still being conducted to improve its clinical outcomes.2 According to national joint registry data in Europe, the approach used is posterior in 59% of cases, lateral/anterior/anterolateral in about 36% of cases, and others in 5% of cases.3 Although there are various surgical approaches in THA, currently there is no consensus regarding which approach is the most suitable one.3
It has been reported that fast-track protocols for THA can reduce hospital stay and complications and result in good clinical outcome.45 Because traditionally large surgical exposure needs a lengthy rehabilitation time, minimally invasive surgery for THA is essential to improve its cost-effectiveness.4 However, there is a disagreement as to whether clinical results for minimally invasive surgery of THA are guaranteed.67
The direct anterior approach (DAA) through the inter-muscular interval between tensor fascia latae and sartorius was introduced by Hueter in 1870.14 Because there is no direct muscular injury in DAA, it has been reported that the increase of biomechanical markers indicating muscular damage is low and muscular damage on the magnetic resonance image is less compared with other approaches.89 In addition, clinically, DAA has been shown to be capable of promoting early ambulation. It has also been demonstrated by gait analysis that DAA can lead to a shorter hospital stay and a lower dislocation rate.31011 However, there are some problems when performing the DAA.312 Because it is usually performed in the supine position, special tables and retractors are required to perform this procedure. In addition, if the surgeon is unfamiliar with this procedure, the operation time is rather long. In addition, damage to surrounding muscle or fracture of greater trochanter, soft tissue release for preparing femur, and capsulectomy could cause more bleeding compared to other approaches. Most surgeons need a learning period for DAA.13
Several reviews have been published regarding surgical approaches of THA.31014 Most studies have described the advantage of early postoperative period that DAA can provide early ambulation and shorten the length of hospital stay because it causes minimum soft tissue damage, although its long-term advantages are less pronounced compared to other approaches.8 However, most studies did not adequately describe perioperative problems or complications of DAA.
Thus, the purpose of this study was to analyze complications through systematic review and network meta-analysis of comparative studies of DAA, anterolateral approach (LA), and posterolateral approach (PA).
METHODS
Our current review and meta-analysis were performed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines, extension of network meta-analysis.15
Study eligibility criteria
Prospective randomized controlled trials (RCTs) or quasi-experimental designs evaluating clinical outcomes of DAA, LA, and PA for complete hip arthroplasty are valid if they meet the following criteria: 1) Comparison of clinical outcomes between the three methods for main complete hip arthroplasty (THA); 2) Compared at least one of the following outcomes: blood loss, operating time, and transfusion volume.; 3) Sufficient data were available to extract and pool, i.e., mean reported, standard deviation and number of subjects.
Search methods for identification of studies
A comprehensive search of all relevant RCTs and comparative studies was conducted through PubMed Central, OVID Medline, Cochrane Collaboration Library, EMBASE, and hand search up to October 2019. We used the following search term: “total hip approach.” A manual search of possibly related references was also conducted (Supplementary Table 1). Two investigators independently reviewed titles, abstracts, and full texts of all potentially relevant studies as recommended by the Cochrane Collaboration.16 Any disagreement was resolved by a third reviewer. Full-text articles of remaining studies were assessed according to previously defined inclusion and exclusion criteria. Eligible articles were then selected. Review authors were not blinded to authors, institutions, or publication.
Data extraction
Two reviewers independently performed data extraction using standardized data extraction forms. The following data were extracted from included articles: authors, publication date, study design, participant number and characteristics (age, gender), type of approach, and outcomes. Outcomes pooled in this analysis included blood loss, transfusion, and operation time. Any disagreement was resolved by discussion and consensus with a third party.
Methodological quality assessment
Two authors independently assessed the methodological quality of included studies using the same criteria for RCTs and as described in the Cochrane Handbook for Systematic Reviews of Interventions 5.2. Ten criteria were: 1) allocation concealment; 2) clearly defined inclusion and exclusion criteria; 3) outcomes of patients who withdrew or were excluded after allocation described and included in an intention-to-treat analysis; 4) groups well matched, or with appropriate covariate adjustment; 5) surgeons' experience; 6) identical care programs other than trial options; 7) clearly defined outcome measures in the text with a definition of any ambiguous terms encountered; 8) blinding of outcome assessors to assignment status; 9) appropriate timing of outcome measures; and 10) reported loss to follow-up less than five percent of participants.
Data analysis
For continuous outcomes, standardized mean difference (SMD) and 95% confidence interval (CI) were calculated. The size of heterogeneity across studies was estimated with I2 statistic and χ2 test. A P value of > 0.10 and an I2 ≤ 50% were considered to be lacking statistical heterogeneity.17 For the test of heterogeneity, we used Higgins I2 statistics. Low heterogeneity was observed in these studies. Therefore, fixed effect models were used for network meta-analysis. Sensitivity analysis was conducted by omitting a single study each time and pooling data of remaining studies to explore possible high heterogeneity and determine the stability of outcomes.
A network meta-analysis was used to assess the effects of treatment between different surgical approaches. Indirect associations between two surgical approaches were performed by borrowing information from the common comparator (i.e., the posterior approach). Contribution plots were made to show the contributions of each direct comparison in the network meta-analysis estimates. A two-stage meta-analysis was used to estimate the relative effects of surgical approaches on THA as follows. The relative treatment effect and variance-covariance were estimated for each study using binary log-link function regression in dichotomous outcomes. The differences in treatment effects (i.e., coefficients and mean difference [MD]) between means were further assessed using the results of the regression model in continuous outcomes. These relative treatment effects were then pooled across studies using a multivariate meta-analysis with maximum probability function. Relative treatment results between surgical methods were measured using a linear combination of a multivariate meta-analysis model. Finally, inconsistency and heterogeneity were assessed using the generalized Cochran's Q statistic for multivariate meta-analysis.1819 Network meta-analysis was conducted using statistical software R (version 3.2.3; R Foundation for Statistical Computing, Vienna, Austria) with GeMTC package (version 0.7-1; van Valkenhoef and Kuiper). Additionally, rank probability analysis was performed using the “rank.probability” function of the GeMTC package. P values < 0.05 were considered as statistically significant unless otherwise specified.
RESULTS
Search results
We identified 9,260 reports through database search (Fig. 1). After removing duplication through the first screen of titles and abstracts where we excluded studies clearly not relevant, 35 articles were considered potentially relevant for review. By full paper review, 27 articles were excluded because they did not meet the inclusion criteria. Finally, eight prospective RCTs were included in the network meta-analysis (Table 1).48132021222324
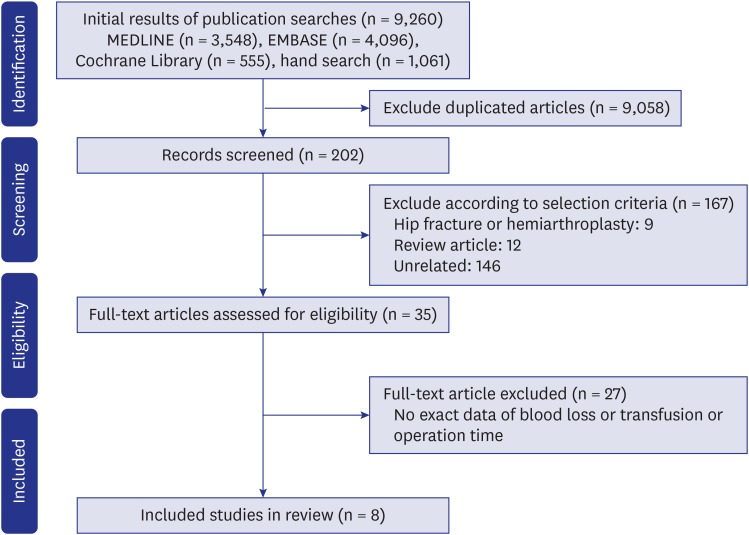
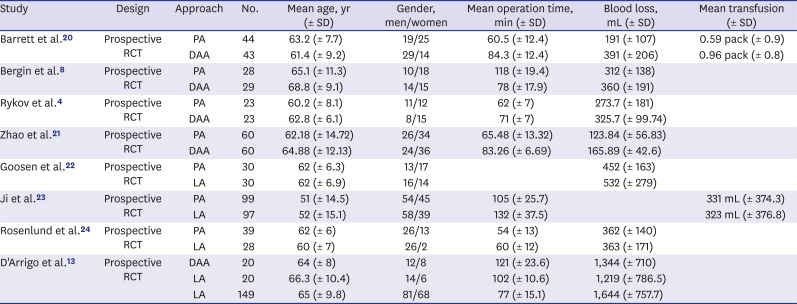
Fig. 1
Preferred reporting items for systematic reviews flow diagram representing details of the process of relevant clinical study selection.
![]()
Table 1
Included studies in network meta-analysis
| Study | Design | Approach | No. | Mean age, yr (± SD) | Gender, men/women | Mean operation time, min (± SD) | Blood loss, mL (± SD) | Mean transfusion (± SD) |
|---|---|---|---|---|---|---|---|---|
| Barrett et al.20 | Prospective RCT | PA | 44 | 63.2 (± 7.7) | 19/25 | 60.5 (± 12.4) | 191 (± 107) | 0.59 pack (± 0.9) |
| DAA | 43 | 61.4 (± 9.2) | 29/14 | 84.3 (± 12.4) | 391 (± 206) | 0.96 pack (± 0.8) | ||
| Bergin et al.8 | Prospective RCT | PA | 28 | 65.1 (± 11.3) | 10/18 | 118 (± 19.4) | 312 (± 138) | |
| DAA | 29 | 68.8 (± 9.1) | 14/15 | 78 (± 17.9) | 360 (± 191) | |||
| Rykov et al.4 | Prospective RCT | PA | 23 | 60.2 (± 8.1) | 11/12 | 62 (± 7) | 273.7 (± 181) | |
| DAA | 23 | 62.8 (± 6.1) | 8/15 | 71 (± 7) | 325.7 (± 99.74) | |||
| Zhao et al.21 | Prospective RCT | PA | 60 | 62.18 (± 14.72) | 26/34 | 65.48 (± 13.32) | 123.84 (± 56.83) | |
| DAA | 60 | 64.88 (± 12.13) | 24/36 | 83.26 (± 6.69) | 165.89 (± 42.6) | |||
| Goosen et al.22 | Prospective RCT | PA | 30 | 62 (± 6.3) | 13/17 | 452 (± 163) | ||
| LA | 30 | 62 (± 6.9) | 16/14 | 532 (± 279) | ||||
| Ji et al.23 | Prospective RCT | PA | 99 | 51 (± 14.5) | 54/45 | 105 (± 25.7) | 331 mL (± 374.3) | |
| LA | 97 | 52 (± 15.1) | 58/39 | 132 (± 37.5) | 323 mL (± 376.8) | |||
| Rosenlund et al.24 | Prospective RCT | PA | 39 | 62 (± 6) | 26/13 | 54 (± 13) | 362 (± 140) | |
| LA | 28 | 60 (± 7) | 26/2 | 60 (± 12) | 363 (± 171) | |||
| D'Arrigo et al.13 | Prospective RCT | DAA | 20 | 64 (± 8) | 12/8 | 121 (± 23.6) | 1,344 (± 710) | |
| LA | 20 | 66.3 (± 10.4) | 14/6 | 102 (± 10.6) | 1,219 (± 786.5) | |||
| LA | 149 | 65 (± 9.8) | 81/68 | 77 (± 15.1) | 1,644 (± 757.7) |
SD = standard deviation, RCT = randomized controlled study, PA = posterolateral approach, DAA = direct anterior approach, LA = anterolateral approach.
![]()
Operation time
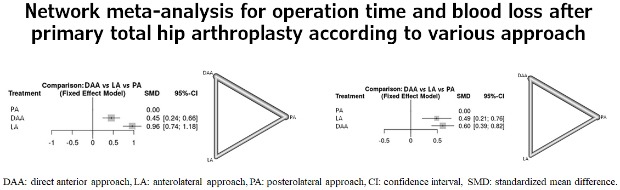
Seven of these eight studies provided pairwise comparisons of operation time (Tables 1, 2 and Fig. 2).481320–24 There was low evidence of heterogeneity across studies (I2 = 97.3%). Thus, the fixed effect model was used. There were statistically significant differences in operation time among the three approaches. The operation time of the LA was longer than that of PA (SMD, 0.96; 95% CI, 0.74–1.18; P < 0.001). DAA also had significantly longer operation time than PA (SMD, 0.45; 95% CI, 0.24–0.66; P < 0.001).
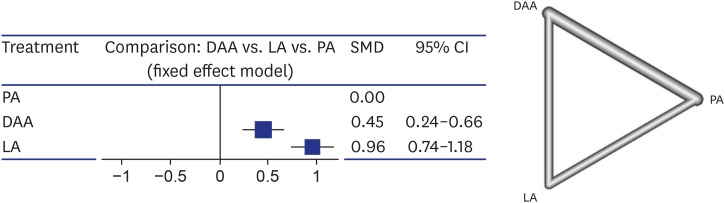
Fig. 2
Network meta-analysis and plots for operation time after primary total hip arthroplasty.
DAA = direct anterior approach, LA = anterolateral approach, PA = posterolateral approach, SMD = standardized mean difference, CI = confidence interval.
![]()
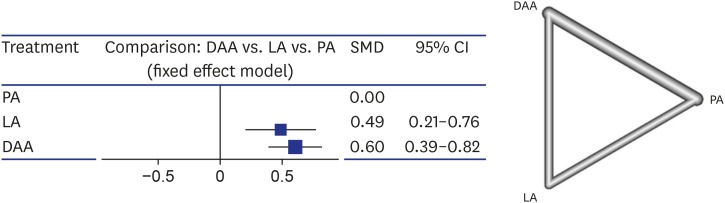
Blood loss
Seven of these eight studies provided pairwise comparisons of blood loss (Tables 1, 2 and Fig. 3).48132021222324 There was low evidence of heterogeneity across studies (I2 = 74%). Thus, the fixed effect model was used. There were statistically significant differences in blood loss among the three approaches. Blood loss with DAA was the highest among the three approaches (SMD, 0.60; 95% CI, 0.39–0.82; P = 0.002).
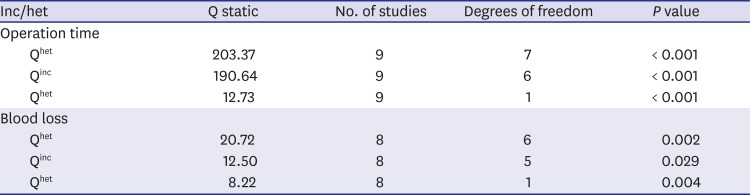
Heterogeneity and inconsistency within designs
Q statistic results for the whole network, for inconsistency, and for heterogeneity within designs are shown. In addition, the number of studies on which they are based, degrees of freedom, corresponding χ2 distributions, and corresponding P values are displayed (Table 2).
DISCUSSION
The main findings of this study are as follows. First, operation time was the longest in LA, followed by that in DAA. It was the shortest in PA. Second, blood loss was the highest in DAA, which was significantly higher than that in LA or PA. Although the longest operating time was observed in THA using LA, DAA did not always show superior results compared to the other two approaches in operation time or blood loss.
The main cause of this result is the steep learning curve for DAA. Most surgeons have a learning curve with this new approach. The faster one breaks away from established methods in general, the greater the risk of unexpected complications.13 A steep learning curve for DAA has been described in a previous study.25 In addition, operation time is relatively long in THA using DAA because it needs a large number of cases to identify operation with PA. One unique characteristic of DAA is that it has a different femoral preparation. Although neither LA nor PA needs a special procedure for femoral preparation, DAA needs enough release of deep structures such as posterior capsule and piriformis, especially during elevation of the femur.20 Sequential release of deep structure takes time for femoral canal preparation in DAA. If surgeons do not release the deep structure enough, DAA has a risk of greater trochanter fracture which takes considerable time for wiring. Although there are specifically designed tables and retractors for DAA, they can also lead to trochanter fracture if the deep structure does not have enough release.26
The steep learning curve can be represented as two phenomena as a result of this study in the perioperative period. The first is the increase in operation time. The second is the increase in blood loss. Although DAA is known as a muscle sparing approach, muscle damage has also been observed in cadaver studies. Tensor fascia latae has been observed to be damaged during surgery in several studies.27282930 Inadequate exposure due to improper release can result in excessive stretching and unintentionally detaching of surrounding soft tissue, leading to an increase in creatine kinase.4 Therefore, the steep learning curve for DAA could decrease the advantage of the approach for reducing blood loss and muscular damage. An increase in operating time necessarily leads to an increase in blood loss. Most surgeons prefer a huge anterior capsulectomy to access the femur than capsulotomy. Capsulectomy can lead to bleeding and a space where hematoma is located continuously. In addition, bleeding from the femoral side causes difficult visualization of the posterior capsule and makes it difficult to control the bleeding when it occurs during posterior soft tissue release.4 It can contribute to prolonged operative time. If femoral fracture and perforation as major complications of DAA occur, they can contribute to blood loss.213132
Although many articles have reported the steep learning curve of DAA, good results have been achieved in some studies with DAA for THA.3334 However, few studies have reported how much DAA should be done to achieve clinical results similar to other approaches.35 Spaans et al.35 have compared DAA and PA (46 THAs in each case). They found that the DAA group in which THAs were performed first had twice the operation time and blood loss. The authors also noted that the operation time tended to decrease with repeated cases, although there was no change in blood loss or hospital stay until after performing the operation for 46 patients. Additionally, there were more complications in the DAA group. Woolson et al.36 and D'Arrigo et al.13 have also reported higher complication rates of 13%–25% as well as longer operation time and more blood loss in the DAA group. Woolson et al.36 have reported that complications are decreased after 30–50 operations. Thus, surgeons should be very careful in changing their daily routine and performing THA through a technique whose benefit has not been proven in the long term because any change might increase complications, especially during the learning-curve phase.35
This network meta-analysis has some limitations. First, we could not evaluate surgeons' familiarity with DAA in each study. Second, data of included studies have heterogeneity. Third, we did not compare other clinical results such as functional scores or complication rates. This is a limit of a meta-analysis. Further studies are needed in the future to overcome these limitations. Finally, we could not analyze the factors such as special table, retractor, and patient position that could affect the surgical outcome of DAA. A network meta-analysis study based on comparative studies of DAA, DL, and PA did not describe all the factors, and statistical analysis could not be performed. In the near future, prospective comparative studies should be conducted based on the covariates such as special table, retractor, and patient position.
In conclusion, we should pay attention to increased operation time and blood loss when performing THA with DAA.
 XML Download
XML Download