

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Heart disease is one of the leading causes of death among children despite the fact that the mortality rate for pediatric patients with advanced heart disease has declined significantly owing to improvements in medical care and cardiac surgeries.123 In addition, heart disease is a major cause of pediatric death due to complex chronic conditions, which account for a significant proportion of pediatric patients who die during hospitalization.45 Children who died from advanced heart disease in hospitals usually received highly aggressive and technical treatment in intensive care units at their end-of-life.678
Pediatric end-of-life care, an important component of palliative care, aims to satisfy the physical, emotional, social, and spiritual needs of children with life-threating diseases at their end of life.9 Appropriate end-of-life care helps mitigate children's suffering, increases parents' preparedness for their child's death, facilitates advanced care planning, and helps the child die in a preferred location.1011 Thus, palliative care programs for pediatric patients with life-limiting disease and their families have been steadily evolving worldwide; however, children with heart disease have rarely received palliative care program.121314
Recent research has assessed the pattern of end-of-life care in pediatric patients with advanced heart disease; however, there remains a lack of studies of end-of-life care for patients with heart disease outside western countries.78 Therefore, the purpose of this study was to investigate the current situation of end-of-life care for hospitalized patients with advanced heart disease in a tertiary referral center in Korea.
METHODS
Study population
We conducted a retrospective chart review of patients who died in the pediatrics department of our hospital between January 2006 and December 2013. Pediatric patients who were diagnosed with advanced heart disease were included in the study. Young adults between the ages of 18 and 35 years were also included to consider end-of-life care for young adults with complex congenital heart disease. To investigate the characteristics of patients with advanced heart disease with sufficient medical records and to minimize the confounding factors, patients who met the following criteria were excluded from the study: 1) patients who died outside the hospital or in the emergency department, 2) patients who died within 1 month after cardiac surgery, and 3) patients who had an extremely low birth weight, congenital diaphragmatic hernia, persistent pulmonary hypertension of the neonate, malignancy, or an immunodeficiency disorder.
Data collection
The following patient characteristics at the final hospitalization were recorded: age, sex, diagnosis of primary heart disease, comorbid genetic disease, length of intensive care unit treatment, and duration of hospitalization. Furthermore, we collected data on parent' education level, residence type, and national health insurance status to identify the socioeconomic status of each patient's family.
The mode of death was categorized as follows: 1) death after withdrawal or withholding of life-sustaining support, 2) death during cardiopulmonary resuscitation, and 3) brain death. The location at the time of death and the cause of death were also recorded. Furthermore, we investigated whether cardiopulmonary resuscitation had previously been performed during the final admission. The total length of the final cardiopulmonary resuscitation was analyzed in the group of patients who died during resuscitation.
We also reviewed the interventions performed within the 24 hours prior to death. These data included the presence and type of mechanical ventilation and the use of inhaled nitrogen oxide, dialysis, and parenteral nutrition support. The use of extracorporeal membrane oxygenation support, left ventricular assist device, pacemaker, implantable cardioverter-defibrillator, and cardiac resynchronization therapy device were also recorded. The presence of central and arterial lines and tracheostomy and gastrostomy tubes was evaluated, as well as the administration of inotropes, antibiotics, analgesics, sedatives, and neuromuscular blockers.
End-of-life care discussion between physician and patients/guardians were identified by searching for documented end-of-life discussions in medical records and the presence of written consent regarding a do-not-resuscitate order. End-of-life care discussions included explanations regarding life expectancy, withdrawal or withholding of certain life-sustaining support, and preferences regarding resuscitation or palliative care. Written consent regarding a do-not-resuscitate order that had been signed by the parents during the final cardiopulmonary resuscitation was not included. We analyzed the relationship between documented end-of-life care discussions and patients' characteristics and the socioeconomic status of their family. Finally, we determined the time interval between the end-of-life care discussion and death for the patients who had been hospitalized for 7 days or more and had documented end-of-life care discussions.
Statistical analysis
Descriptive data are presented as medians and ranges or means and standard deviations, whereas categorical variables are presented as numbers and percentages. The Mann-Whitney U test and Pearson's χ2 test/Fisher's exact test were performed for continuous and categorical variables, respectively. A P value less than 0.05 was considered statistically significant. Data manipulation and statistical analyses were performed using SPSS 23.0 for Windows (IBM SPSS, Inc., Chicago, IL, USA) and Microsoft Office Excel 2013 (Microsoft Inc., Redmond, WA, USA).
RESULTS
Patient characteristics
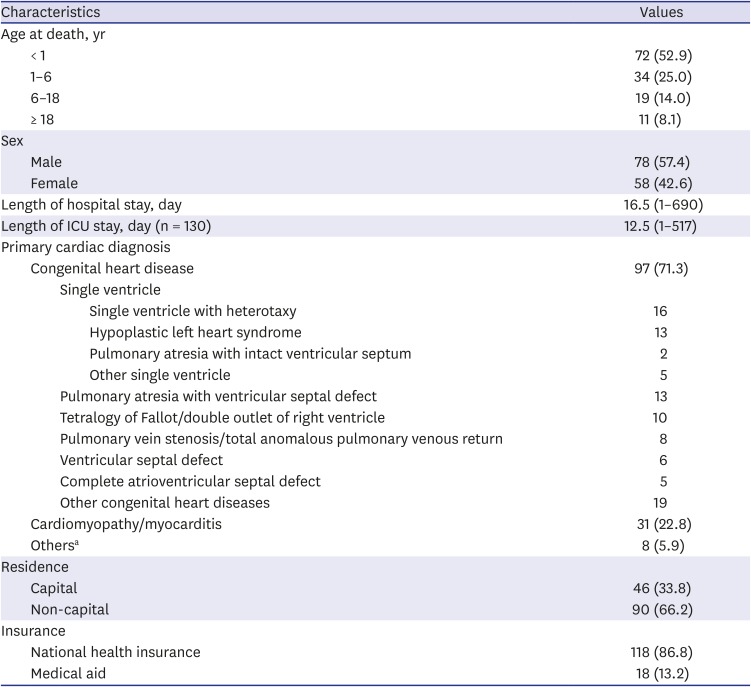
Of the 652 patients who had died in the pediatric department from all causes of death during the study period, 136 patients with primary heart diseases were included in the current study. Their median age at death was 10.0 months (range, 1 day–28.3 years) (Table 1). More than half of the patients (72, 52.9%) died within a year after their birth, and 24 patients of them died during the neonatal period. The median duration of the final hospitalization was 16.5 days (range, 1–690 days), and 90 patients (66.2%) were hospitalized for 7 days or more. One-quarter of the patients (33, 24.3%) were confirmed or suspected of having comorbid genetic disease. The majority of patients (130, 95.6%) received treatment in an intensive care unit at least once during the final hospitalization, and 74 patients (54.4%) received treatment in an intensive care unit for 7 days or more. Three-fourths of the patients (97, 71.3%) had congenital heart disease, and 36 patients of them had a single ventricle physiology. Most parents (118, 86.8%) had Korean national health insurance. One-third of the patients (46, 33.8%) lived in the capital where the hospital was situated.
Table 1
Patient characteristics
Circumstances of in-hospital death of children with advanced heart disease
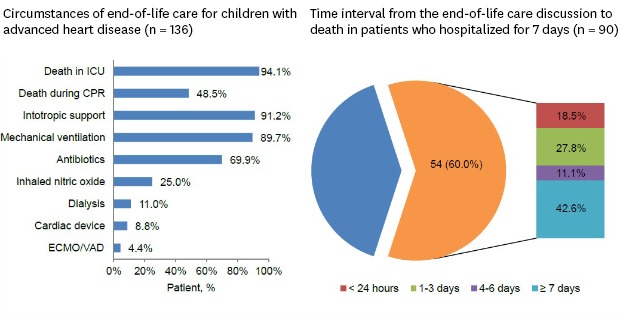
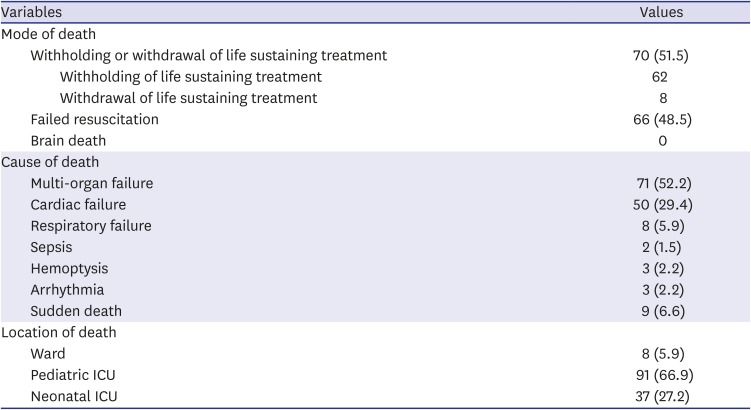
Seventy patients (51.5%) died following the withholding or withdrawal of life-sustaining treatment, whereas 66 patients (48.5%) died during cardiopulmonary resuscitation (Table 2). Among the patients who died during cardiopulmonary resuscitation, the median duration of the cardiopulmonary resuscitation was 51.5 minutes (range, 4–257 minutes), and 25 of 66 patients received cardiopulmonary resuscitation for 1 hour or more. More than half of the patients (71, 52.2%) died from multi-organ failure. Most patients (128, 94.1%) died during care in the intensive care unit, and only 6 patients died in the general ward.
Table 2
Circumstances of in-hospital deaths of pediatric patients with heart disease
Interventions performed within 24 hours of death
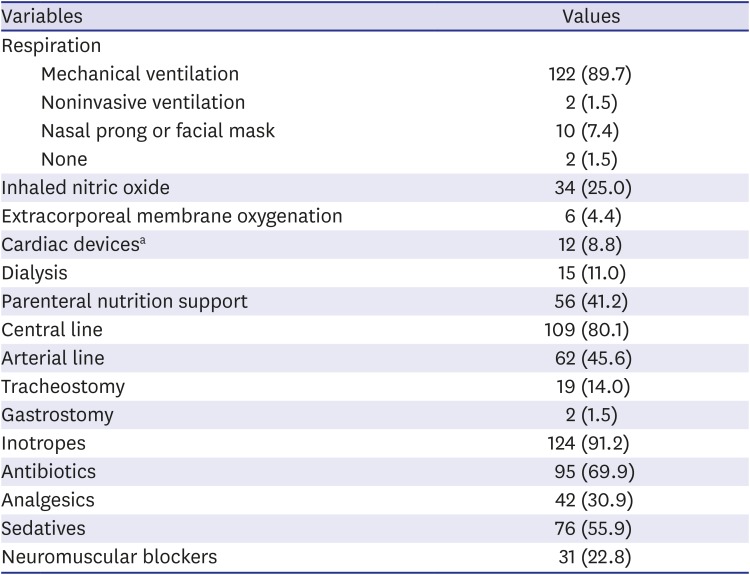
Most patients (122, 89.7%) had received mechanical ventilation, and 14 patients (10.3%) had received high-frequency oscillatory ventilation within 24 hours of death (Table 3). Extracorporeal membrane oxygenation was applied to 6 patients (4.4%). Of the 12 patients (8.8%) with cardiac devices, 10 patients had a pacemaker, 1 had an implantable cardioverter defibrillator, and 1 had a cardiac resynchronization therapy device. Of the 15 patients (11.0%) who had received renal replacement therapy for acute renal failure, 12 patients received continuous renal replacement therapy and 3 received peritoneal dialysis. Fifty-six patients (41.2%) had received parenteral nutrition support prior to death. Most patients (124, 91.2%) had required inotropic support. More than half of the patients (76, 55.9%) received sedatives, and one-third of the patients (42, 30.9%) received analgesics.
Table 3
Interventions performed within 24 hours of death
End-of-life care discussions for children with advanced heart disease
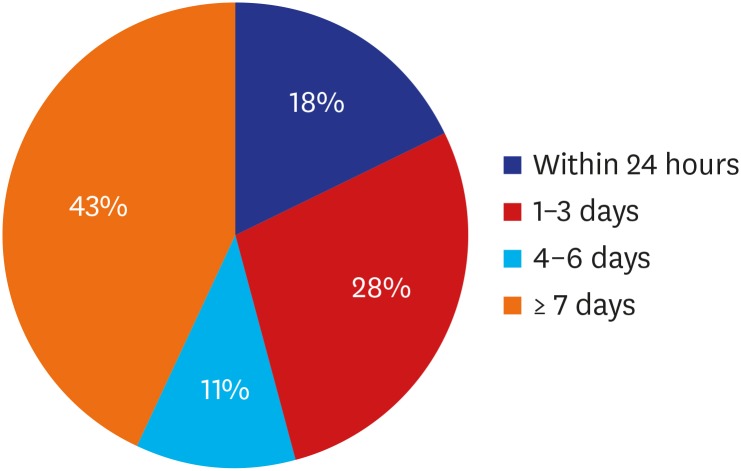
Seventy-four patients (54.4%) had documented end-of-life care discussions; of these, the discussions of 19 patients (19/74, 25.7%) occurred on the date of the patient's death. Seventy patients (70/74, 94.6%) died following the withholding or withdrawal of life-sustaining treatment and consent to a do-not-resuscitate order was written in 59 patients (59/74, 79.7%). The patient's age, sex, and comorbid genetic disease were irrelevant to the documented end-of-life care discussion (Table 4). The patients who had documented end-of-life care discussions were hospitalized longer than those who did not (23 days [range, 1–366] vs. 12 days [range, 1–690]; P = 0.042). The former patients had also remained for longer in the intensive care unit (15.5 days [range, 1–300] vs. 6 days [range, 1–517]; P = 0.020). Parents' education level, residence type, and national health insurance status were not related to the discussion regarding patients' end-of-life care. All discussions regarding end-of-life care occurred between the physicians and patients' parents or guardians; thus, no patients participated in the discussion of their end-of-life care. Of the 90 patients who were hospitalized for 7 days or more, the parents or guardians of 54 patients (54/90, 60%) had end-of-life care discussions. The time interval from the end-of-life care discussion to death was 3 days or less for 25 patients (25/54, 46.3%) (Fig. 1).
Table 4
Demographic and clinical characteristics according to the presence of end-of-life care discussion
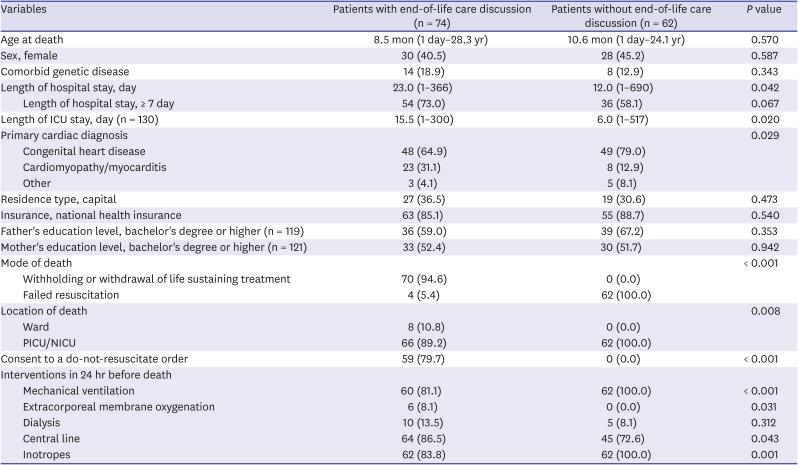
Fig. 1
Time interval from the end-of-life care discussion to death in patients who hospitalized for ≥ 7 days (n = 90). Fifty-four patients (54/90, 60%) had end-of-life care discussions, and the time interval from the end-of-life care discussion to death was three days or less for 25 patients (25/54, 46.3%).
DISCUSSION
This study explored the recent trends in the end-of-life care for pediatric patients with advanced heart disease in a tertiary center in Korea. First, most patients (128, 94.1%) received highly intensive treatment and died in the intensive care unit. Second, half of the patients (66, 48.5%) died following an unsuccessful cardiopulmonary resuscitation, and the duration of some cardiopulmonary resuscitations was prolonged. Third, discussions regarding end-of-life care were often deferred until the day of the patient's death, despite the patient being hospitalized for 7 days or more. Finally, all discussions regarding end-of-life care occurred between the physicians and parents or guardians; the patients did not have the opportunity to confer with physicians about their end-of-life care and might not have been prepared for their death.
Most patients with heart disease were intubated, received highly advanced treatment, or died in the intensive care unit in our study. These findings are consistent with previous studies.678 Some patients (25/66, 37.9%) died after prolonged cardiopulmonary resuscitation, despite the fact that survival rates are lower and neurological outcomes are poorer with longer cardiopulmonary resuscitation duration.15 The frequencies of sedative drug and analgesic use at the end-of-life were lower than those reported in previous studies, including studies of general pediatric patients. This finding may reflect the invasiveness of the treatment for pediatric patients with heart disease in the current study.616
There were 3 possible reasons for this reported high invasiveness of treatment. First, with the advancement of technology for surgery and medical treatment, pediatric cardiologists can use advanced medical equipment, such as extracorporeal membrane oxygenation and ventricular assist devices, to save the lives of pediatric patients. In some cases, cardiac transplantation is an option for pediatric patients with heart disease that is intractable to medical treatment or surgery.17 Therefore, pediatric cardiologists are likely to be unfamiliar with the decision-making process of shifting from attempting to cure patients to performing palliative care.18 Second, parents are more likely to prolong the lives of their children via invasive treatments, even when there is no chance that the child's life will be extended. They may believe that there are remaining treatment options or that their child will survive, or they may have a more positive view regarding the quality of life of their child despite physician opinions.19 Third, parents might not have known that their child had little possibility of survival until death was near.7
For more than half of the patients with documented discussions regarding end-of-life care, this discussion occurred immediately prior to death. This finding is consistent with that of a previous study.7 Several studies have demonstrated that early integration of palliative care including end-of-life issues into the treatment plan is necessary to improve patients' quality of life and help patients prepare for their deaths.2021 However, there are several obstacles to early discussions regarding end-of-life care. First, some patients exhibit unpredictable courses and variable progression, which make it difficult for the physician to know when these patients will die and therefore, when the physician should start discussing the poor prognosis with the patient's family.22 Second, a lack of in-depth conversation regarding the prognosis of heart disease can result in different understandings of the prognosis between patients or parents and physicians. Parents who care for pediatric patients with heart disease are likely to have more optimistic expectations regarding the prognosis of their children than physicians.818 Third, physicians may worry that some patients or parents misunderstand the concept of palliative and end-of-life care and believe palliative care is akin to abandonment of their children.23 Finally, insufficient education regarding palliative care among pediatricians can make it difficult for them to understand when to initiate discussions regarding end-of-life care.24
None of the patients in the present study had the chance to participate in a discussion regarding end-of-life care with their doctors, although some patients were adolescents and young adults. Most discussions regarding end-of-life care occurred between physicians and parents. Patients may have been too sick to participate in discussions regarding their end-of-life care at this point. Physicians or parents may not have wanted to disclose the terminal illness to patients. In Asia, a child is considered a family member for whom the parents are responsible, and parents want to protect their child from highly negative information rather than considering the patient's autonomy.2526 However, adolescents and young adults can understand the concept of death, and some of these patients may be competent to make decisions regarding their lives.27 More than half of adolescents with life threatening disease were reported being comfortable talking about their end-of-life issues. Indeed, not all decisions made by parents and physicians completely accord with the decisions of adolescent and young adult patients.28 Adolescents and young adult patients should be given opportunities to participate in discussions of end-of-life care and express their wishes via early involvement of palliative care. To ensure optimal communication with adolescents and young adults regarding end-of-life care, physicians should take a gradual approach along with family support, considering the spiritual and cultural factors of the patient.29 Educational programs, such as communication skills training, have been helpful for physicians to learn the skills required to deal with a challenging situation, including transitioning to palliative care and end of life.30
Pediatric palliative care programs must be established to provide appropriate end-of-life care for pediatric patients with advanced heart disease.9 Pediatric palliative care has evolved over the previous 2 decades such that more than half of the hospitals in the United States have pediatric palliative care programs; historically, pediatric patients with heart disease infrequently used palliative programs.1214 Pediatric palliative care teams can assist patients with complex congenital heart disease and their families by providing help with medical decision-making, advance care planning, and bereavement management.31 A recent single-center study reported that pediatric palliative care teams are primarily involved in the goals of care, psychosocial support, symptom management, and advance care planning for patients with advanced heart disease and their families.32
The present study had several limitations. First, as a retrospective study, only documented discussions regarding end-of-life care were collected; thus, discussions that had not been documented could not be identified. Second, this study included a small number of patients who died at a single tertiary referral hospital; thus, we could not identify patterns of end-of-life care among patients who died at home. Third, the subjective symptoms of the patients and the parents' preparedness for end-of-life were not explored; such factors could provide different perspectives of the death process in pediatric patients.
In conclusion, the present study is the first to explore the current status of end-of-life care pediatric patients with advanced heart disease outside of western countries. Our findings demonstrate that among most pediatric patients with advanced heart disease who died in our hospital, discussions with these patients regarding end-of-life care were postponed until immediately prior to death. Pediatric palliative care programs must be implemented to improve the quality of death of pediatric patients with heart disease.
 XML Download
XML Download