

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
In mechanically ventilated critically ill patients, opioids are often required to manage pain and agitation.1 When opioid therapy is abruptly discontinued, opioid withdrawal syndrome (OWS) can develop, indicated by the presence of symptoms such as anxiety, irritability, tachycardia, and tachypnea.2 The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) defines OWS as the occurrence of three or more characteristic symptoms (such as dysphoric mood, nausea, vomiting, diarrhea, or fever) within minutes to several days after cessation or reduction of high dose or prolonged opioid therapy.3 However, it is difficult to apply these criteria in mechanically ventilated patients as symptom evaluation can be challenging.
Some OWS assessment tools have been validated for use in pediatric patients,45 and the incidence of OWS in critically ill children has been reported to range between 10% and 57%.67 Several risk factors (such as cumulative dose, duration of analgesia, and the administration of sedative drugs) are known to increase the risk of OWS.891011 However, few studies have evaluated the incidence, symptoms, and risk factors for OWS in critically ill adult patients.1213 In addition, an assessment tool has not been established to evaluate the symptoms and diagnosis of OWS in this patient group. Although a prospective study recently reported an OWS incidence of 16.7% in adults, the study was limited by the use of the DSM-5 criteria to assess OWS and a lack of information on symptoms or type of opioid used.13
The objective of the current study was to determine the incidence of OWS using our own tool developed for the assessment of adult patients treated in a medical intensive care unit (ICU). The clinical features, risk factors and incidence of OWS according to the type of opioid were also analyzed as secondary objectives.
Go to : 
METHODS
Study design and population
This retrospective cohort study was conducted in the Asan Medical Center, Korea. Data from critically ill patients aged ≥ 18 years who were admitted to the medical ICU between November 2015 and October 2016 were evaluated. As of November 2016, the Health Insurance Review & Assessment Service of the Korea national government has prohibited the administration of remifentanil for more than 3 days; therefore, the period of enrollment was set to 1 year prior to this date.1415 Patients were required to be supported on mechanical ventilation for > 3 days and to have received only one type of opioid.41316 Patients were excluded if they suffered from central nervous system (CNS) diseases that disturbed the assessment of OWS (such as status epilepticus, brain hemorrhage, and meningitis) or if they were discharged or died without reducing the opioid dose. The inclusion period for patients receiving fentanyl or morphine was amended from November 31, 2011 to October 31, 2017 due to the limited number of eligible patients. This was because there was a preference for remifentanil in our institution, with few patients receiving fentanyl or morphine only.
OWS
As there are no validated assessment tools for OWS in mechanically ventilated adult ICU patients, OWS assessment was based on several pediatric assessment tools and the DSM-5 criteria.417 The OWS assessment period was from the cessation of opioid therapy to a maximum of 24 hours because the continuous infusion of opioids has a longer context-sensitive half-life than the general half-life.181920 For patients whose opioids were maintained at a reduced dose throughout the ICU stay, the OWS assessment period was 24 hours from the point where the opioid dose was 50% of the maximal dose. If patients died or were transferred to the general ward, the evaluation could be terminated earlier than 24 hours. If opioids were re-introduced or the dose increased 2-fold, OWS was evaluated from the initiation of assessment to the time of adjusted dosing. Also, in patients receiving a reduced opioid dose, if cessation occurred within 24 hours during the evaluation of OWS, the period of evaluation was prolonged to 24 hours from opioid cessation. Because OWS is known to occur more frequently as the cumulative duration of opioid administration increases in pediatric ICU patients, we only evaluated the last period in case of having many periods of assessment.72122
During the assessment period, five CNS symptoms were evaluated: 1) a change in the Confusion Assessment Method (CAM) scoring to a positive signal; 2) increased pupil size by one plus signal; 3) Glasgow Coma Scale score increase of ≥ 2; 4) increased Richmond Agitation-Sedation Scale (RASS) score of ≥ 2; 5) new onset of seizures. In addition, six autonomic nervous system (ANS) symptoms were assessed: 1) new onset of fever or temperature increase of ≥ 1°C; 2) and 3) increased respiratory or pulse rate by 20% of the mean observed during the previous 4 hours; 4) and 5) increased frequency of suction at the endotracheal or oral secretion by more than twice the mean observed during the previous 4 hours; 6) new onset of loose stools or diarrhea. The starting time and duration of symptoms were also recorded. OWS was determined if ≥ 3 of the total 11 symptoms persisted for more than 2 hours simultaneously during the period of evaluation. Patients were excluded if other events occurred, such as extubation, arrhythmia or the requirement for invasive procedures, such as central venous line insertion, percutaneous pigtail insertion or bronchoscopy.
Data collection and clinical outcomes
The following demographic and clinical outcomes data were collected for each patient from the electronic medical records: age, gender, reason for ICU admission, comorbidities, history of opioid drugs used for more than 3 days prior to administration to the ICU, chronic alcoholism, septic shock or dialysis within 24 hours of admission to the ICU, Sequential Organ Failure Assessment (SOFA) score at admission, and use of sedatives at the time of OWS evaluation. The reason for admission to the ICU was classified as infection, bleeding event, respiratory failure, heart failure, post-operative management, and others. Comorbidities comprised diabetes mellitus, hypertension, respiratory disease, liver disease, renal disease, heart disease, solid cancer, hematologic malignancy, immunosuppression, and others. Clinical data included the duration and cumulative dose of opioid received from ICU admission to evaluation. All opioid doses were converted into morphine equivalents.23 For all enrolled patients, data on the occurrence of any of the 11 symptoms included in the assessment criteria, time of symptom onset, and the duration of symptoms were collected up to 24 hours after initiating the evaluation by the electronic medical records where the nurse recorded the patient's status.
The primary outcome was the overall incidence of OWS. The clinical features of OWS and the incidence of OWS according to the type of opioid were also analyzed as secondary objectives. Covariates were analyzed to evaluate risk factors for the development of OWS.
Statistical analysis
Descriptive data are expressed as proportions, and continuous variables as a median with interquartile range or mean plus standard deviation. The χ2 test or Fisher's exact test was used to compare categorical variables, while one-way analysis of variance or the Kruskal-Wallis test was used for comparing continuous variables with normal or non-normal distribution, which were corrected in post hoc analysis using Bonferroni's method. The incidence of OWS is defined as the proportion of patients with a positive OWS diagnosis. The sensitivity of the symptoms of OWS was calculated as patients with the symptom/patients with OWS; and specificity was patients without symptoms/patients without OWS. The sample size was calculated to compare the incidence of each opioid as well as entire patients in the setting of type 1 error as 0.05 and power 80%, based on the incidence reported in a recent study (16.7%) along with our internal incidence data (35%) obtained from 30 patients in our hospital.13 The multivariable Cox-proportional hazards model was used to identify independent predictors of OWS development. The time used in the Cox-proportional hazards model was from the initiation of opioids in the ICU to the occurrence of OWS. A final model was constructed using a stepwise method; a P value of ≤ 0.15 in the univariate analysis was set for entry of variables. A two-sided P value < 0.05 was considered statistically significant. All statistical analyses were performed using IBM SPSS Statistics for Windows/Macintosh, version 24.0 (IBM Corp., Armonk, NY, USA).
Ethics statement
The study protocol was approved by the Institutional Review Board (IRB) of Asan Medical Center (IRB No. 2017-1248) and performed in accordance with the amended Declaration of Helsinki. Because this study was the retrospective analysis, IRB confirmed the requirement for informed consent was waived.
Go to :
RESULTS
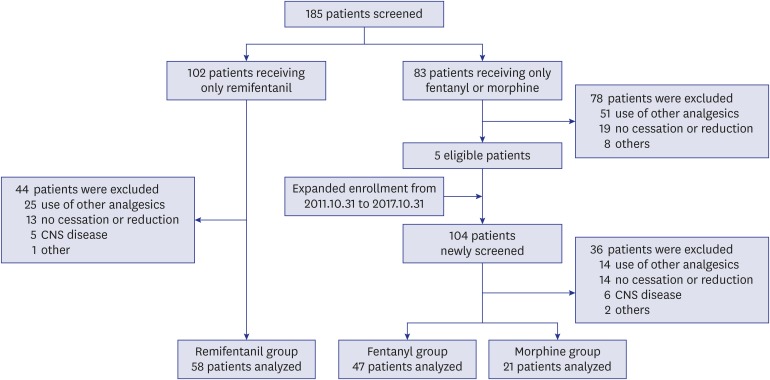
During the study period, 185 adult patients admitted to the medical ICU were screened; of these, 102 patients (55.1%) received remifentanil and 83 (44.9%) received other opioids (Fig. 1). Of the 102 patients in the remifentanil group, 58 patients (56.9%) met the inclusion criteria. Ultimately, 47 patients who had received fentanyl and 21 patients who had received morphine were included in the analysis. The main reasons for exclusion were administration of other opioids, no cessation or reduction of opioids, and the presence of a CNS comorbidity.
Characteristics
The baseline characteristics of the 126 patients included in the analysis are shown in Table 1. The mean patient age was 68.3 years (± 14.1 years), and 85.0% were men. The most common reason for mechanical ventilator application was infection (48.4%). The study patients had high severity of illness with mean SOFA scores of 9. Comparison of the demographic variables according to type of opioid showed no significant differences in age, gender, reason for mechanical ventilator application, comorbidity, chronic alcoholism, septic shock, and dialysis. Statistically significant differences in the history of opioid exposure and SOFA score were seen between the groups; the remifentanil group had a slightly lower proportion of patients with a history of opioid exposure than other groups (P = 0.007), and patients in the fentanyl group had a higher level of disease severity than those in the morphine group (P = 0.004). There was a tendency for a higher use of sedatives in the remifentanil group than in other groups (P = 0.011); most of the remifentanil group (62.1%) had received a sedative in the assessment period, because there were a higher proportion of patients in this group undergoing de-escalation than in the other groups. Propofol was the most commonly used sedative in all three groups.
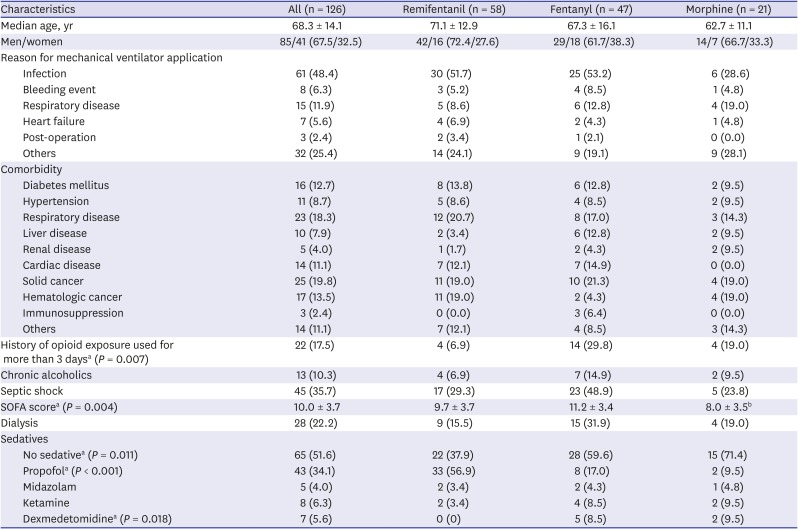
Table 1
Patient characteristics
Results are reported as mean ± standard deviation or number (%).
SOFA = Sequential Organ Failure Assessment.
aStatistical significance when comparing the variables of the three groups; bvs. the fentanyl group.
![]()
Incidence of OWS
The overall incidence of OWS was 29.4% (37 of 126 patients), with 18 patients (31.0%) in the remifentanil group, 17 (36.2%) in the fentanyl group, and two (9.5%) in the morphine group (Table 2). Although there was no statistically significant difference between the three groups (P = 0.078), patients in the morphine group tended to develop OWS less frequently. The type of withdrawal differed significantly between the remifentanil group and the other groups (P = 0.001). However, there was no difference in the incidence of OWS according to the type of withdrawal among the three groups. The total cumulative opioid dose (adjusted into the corresponding morphine dose) was highest in the remifentanil group (median, 5,023.8 mg), compared with the fentanyl (median, 2,090.4 mg) and morphine (median, 216.0 mg) groups. The total duration of opioid infusion did not differ between the three groups. There were no differences in total observation time between the three groups (P = 0.209). Of the 126 patients included in the study, only 33 were evaluated for less than 24 hours due to transfer to the general ward, re-infusion of opioids or death.
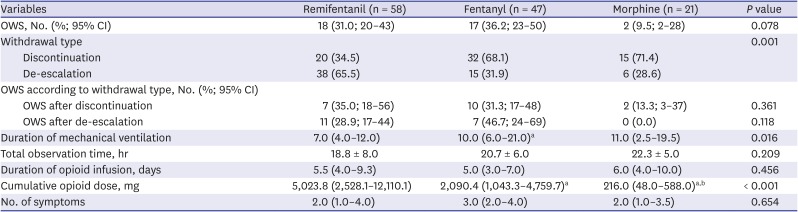
Table 2
OWS according to the type of opioid analgesic
Results are reported as number (%), mean ± standard deviation, or median (interquartile range).
OWS = opioid withdrawal syndrome, CI = confidence interval.
avs. the remifentanil group; bvs. the fentanyl group.
![]()
Symptoms of OWS according to type of opioid
The most common symptoms in all patients was a change in respiratory or pulse rate (Table 3). Of the ANS symptoms, the onset of new fever was the least frequent. Of the CNS symptoms, a change in CAM, RASS, and pupil size occurred with similar frequency, but a change of Glasgow Coma Score or new onset seizure was less common. In the remifentanil group, a change in respiratory rate (RR) had the highest sensitivity for OWS (94.4%; 95% confidence interval [CI], 74.2−99.0) of the 11 symptoms, but specificity was low (52.6%; 95% CI, 39.9−65.0). By contrast, a change of RASS score (90.0%; 95% CI, 77.0−96.0), increased oral secretion (95.0%; 95% CI, 83.5−98.6), sputum (95.0%; 95% CI, 83.5−98.6), and new onset loose stool or diarrhea (72.7%; 95% CI, 51.9−86.9) showed high levels of specificity. Although the sensitivity of both a change of RR and pulse rate was lower, almost all patients with increased oral secretion (95.0%; 95% CI, 83.5−98.6) or sputum (100.0%; 95% CI, 90.8−100.0) satisfied the criteria for OWS in the fentanyl group. In the morphine group, there were too few patients to perform this analysis.
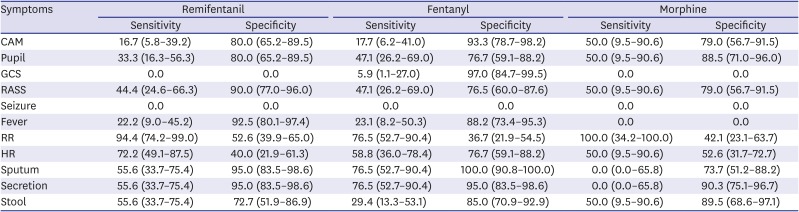
Table 3
Sensitivity and specificity of opioid withdrawal symptoms according to the type of opioid analgesic
Results are reported as % (95% confidence interval).
CAM = Confusion Assessment Method, GCS = Glasgow Coma Scale, RASS = Richmond Agitation-Sedation Scale, RR = respiratory rate, HR = heart rate.
![]()
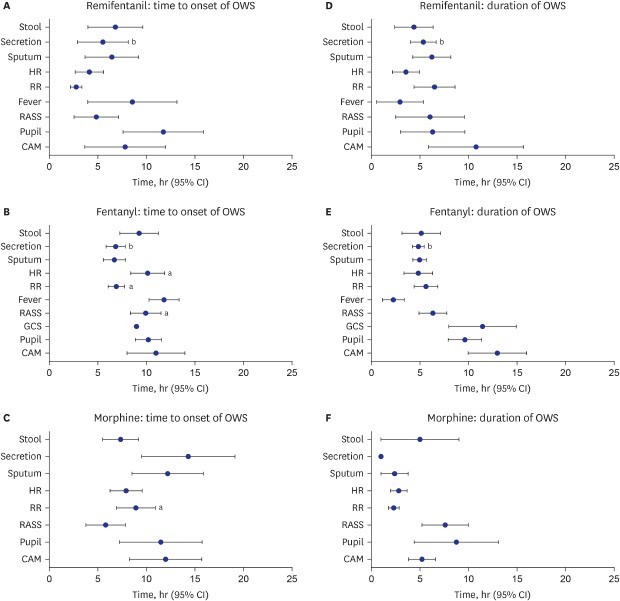
The onset and duration of the 11 symptoms in all patients are shown in Fig. 2. The onset of CNS symptoms did not differ among the three groups. The median onset time of changes in CAM and pupil size ranged from 7 to 12 hours. However, the onset time of change in RASS in the remifentanil group (4.5 ± 3.8 hours) was significantly earlier than that in the fentanyl group (9.9 ± 1.5 hours). There were many differences in onset time among the ANS symptoms between the three groups. The remifentanil group showed a faster onset time for both a change in RR (2.7 ± 1.9 hours) and pulse rate (4.1 ± 3.5 hours) than those in the fentanyl group. In addition, the morphine group showed a later onset time for increased oral secretion (14.3 ± 8.3 hours) than the other groups. Most of the ANS symptoms had similar durations of approximately 2–6 hours. The only difference was that the morphine group had a shorter duration of increased oral secretion than the other groups (1 hour). The duration of CNS symptoms was generally longer than that of the ANS symptoms, although there was no variation in the duration according to the type of opioid.
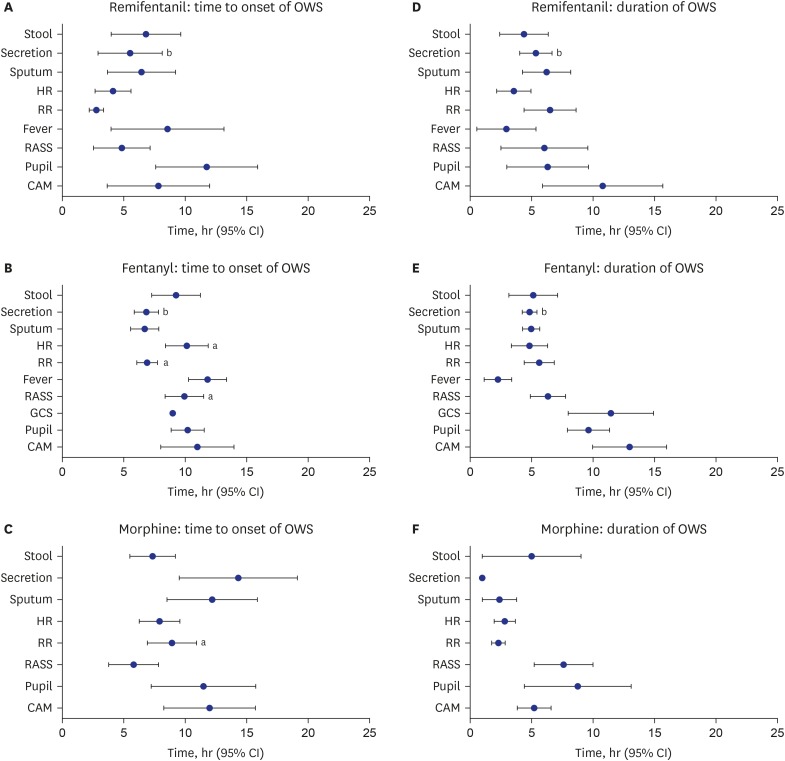 | Fig. 2Onset time and duration time of symptoms during 24 hours after discontinuation or de-escalation of opioid infusion. (A) Onset time of remifentanil group. (B) Onset time of fentanyl group. (C) Onset time of morphine group. (D) Duration time of remifentanil group. (E) Duration time of fentanyl group. (F) Duration time of morphine group.OWS = opioid withdrawal syndrome, CAM = Confusion Assessment Method, CI = confidence interval, GCS = Glasgow Coma Scale, RASS = Richmond Agitation-Sedation Scale, RR = respiratory rate, HR = heart rate.
avs. the remifentanil group; bvs. the morphine group.
|
Risk factors of OWS
To investigate risk factors, we conducted a multivariate analysis for covariables associated with OWS (Table 4). Although there were differences in history of opioid exposure, SOFA score, cumulative opioid dose, and use of sedatives among the three groups, univariate analysis showed a statistically significant association between OWS and septic shock, duration of opioid infusion, and total cumulative opioid dose. These variables, along with type of opioid and SOFA score, were included in the multivariable analysis. The stepwise Cox-proportional hazard model for multivariable analysis yielded two main predictors of OWS: the use of morphine as an analgesic (hazard ratio [HR], 0.17; 95% CI, 0.04–0.74) and the duration of opioid infusion (HR, 0.57; 95% CI, 0.45–0.71). The final model was statistically significant (χ2 [3] = 10.10, P = 0.018).
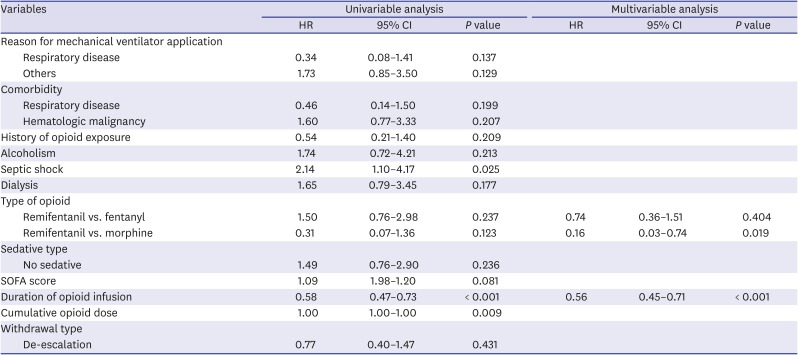
Table 4
Univariable and multivariable analyses of covariables associated with OWS
OWS = opioid withdrawal syndrome, SOFA = Sequential Organ Failure Assessment, HR = hazard ratio, CI = confidence interval.
![]()
Go to :
DISCUSSION
In the current study, a high frequency of OWS was observed in mechanically ventilated adult medical ICU patients. A change of RR was the most common symptom of OWS, and increased oral secretion or sputum was the most specific symptom. In addition, a longer duration of opioid infusion and use of morphine showed a significant association with a decreased risk of OWS. These results could help to improve understanding of OWS in ICU physicians underestimating OWS. As a result, this may have an effect of increasing awareness about OWS in adult ICU.
The data presented here are similar to those reported in previous studies over the past two decades.1213 One retrospective study evaluated 28 critically ill adult patients supported on mechanical ventilation for more than 7 days in the trauma and surgical ICU. Of these, nine patients were diagnosed with opioid or sedative withdrawal syndrome, although the study did not distinguish between the two syndromes.12 Another recent study showed the incidence of OWS to be 16.7% in patients receiving mechanical ventilation for > 72 hours.13 Despite the differences between the three studies in terms of study design, reason for admission and assessment tool used, it is evident that OWS is highly prevalent in adult ICU patients.
Few studies have reported the symptoms of OWS in critically ill adult patients. The only previous study is a small series of nine patients with opioid or benzodiazepine withdrawal syndrome.12 The common symptoms were irritability (100%), hypertension (88.9%), tachycardia (77.8%) and tachypnea (44.4%). A case series of three patients with remifentanil withdrawal syndrome showed that anxiety, hypertension, and tachycardia occurred in all three patients; tachypnea, dilated pupils, and sweating were observed in two of the three patients.24 Although there are some differences in the frequency of symptom reporting between previous studies and the current study, the occurrence of symptoms such as tachycardia, tachypnea, and anxiety was similar. However, a key difference is the occurrence of increased oral secretion and sputum in the current study, which showed a high specificity for OWS. In this study, the increase in RR was not specific to OWS irrespective of the characteristics of opioid analgesics. ICU patients are prone to many other causes of tachypnea, such as fever, pain and fluctuations in hemodynamic and respiratory conditions. Therefore, tachypnea would have shown a high sensitivity, but low specificity for OWS.
The current study showed a significantly lower incidence of OWS in patients who received morphine than in those receiving remifentanil or fentanyl, which is consistent with previous studies of pediatric patients.482526 Animal studies have shown differences between the mechanisms involved in the antinociceptive effects of compounds such as fentanyl and its analogs and morphine. Morphine interacts differently with the mu receptor than fentanyl analogs, which may explain its lack of mu receptor desensitization.272829 These data may explain the difference in the incidence of OWS seen in patients receiving morphine versus those receiving remifentanil or fentanyl. In addition, the half-life is an important factor associated with the incidence of OWS. The ultra-short half-life of remifentanil may be disadvantageous and the relative concentration of opioids in the brain may play a central role in the risk of OWS.8 P-glycoprotein, the efflux receptors at the Blood-Brain Barrier, are involved in the concentration of morphine and fentanyl derivatives in the CNS.30 Because morphine-6-glucuronide, the metabolite with a higher analgesic potency than the parent compound, is not a substrate of P-glycoprotein, the concentration of this derivative in the brain would remain higher than those of other drugs after discontinuation. Therefore, a decrease in the concentration of opioid in the brain would be less precipitous in patients receiving morphine than in patients receiving other types of opioid. In addition, the large difference in mean cumulative opioid dose between the three groups may have contributed to the incidence of OWS.11 Because the potency of remifentanil and fentanyl is approximately 100 fold greater than that of morphine, significant differences in the cumulative dose occurred after conversion of opioids into an equianalgesic dose of morphine. Although the cumulative dose per se showed no association with the incidence of OWS in the multivariable analysis, the larger differences in equianalgesic dose means that different opioids could have resulted in varying degrees of withdrawal effects. It is therefore important for physicians to consider the pharmacological aspects of different opioids when selecting an agent for their critically-ill patients.
This study has some limitations, in addition to the small sample size. First, differences in demographic characteristics were seen between the treatment groups. Fewer patients in the remifentanil group had a history of past opioid exposure than those in the other groups, and patients in the fentanyl group had higher SOFA scores than those in the morphine group. These differences could have affected the occurrence of OWS. Owing to the retrospective nature of the present study, it is not feasible to know the relative impact of these differences. Therefore, randomized, controlled trials are required to exclude factors that may influence the rate of OWS. Secondly, OWS was diagnosed using assessment tools that have not yet been validated, as a validated assessment tool has not yet been developed for use in critically ill adult patients. The application of the new assessment tool, which was not fully validated, could have over-estimated the incidence of OWS by misclassifying symptoms arising from other causes. Thirdly, changes in the inclusion criteria of the fentanyl and morphine groups may have affected the outcome of this study. In our hospital, morphine was the oldest opioid used and remifentanil was the most recent. Nevertheless, it was notable that OWS tended to occur least frequently in patients treated with the oldest opioid, considering the general improvement in ICU care over time. In addition, the time window for OWS detection was limited to 24 hours. It is known that OWS may occur some days after cessation of opioid therapy, based on the criteria of DSM-5. The context-sensitive concentration of fentanyl is more than 5 hours and the context-sensitive half-life of morphine is not known.31 The assessment period was selected as it is four times that of the longest known context-sensitive half and it is possible that patients who exhibited withdrawal symptoms after the evaluation period may have been missed. Finally, OWS in our subjects was shown to occur less frequently with a longer duration of opioid use and there is no obvious explanation for this observation. Previous studies have reported conflicting results regarding the relationship between the incidence of OWS and duration of opioid use.41316 In two pediatric studies, adjusted models showed that a longer duration of opioid treatment was a risk factor for the development of OWS. However, a study of adult patients did not show an association between the duration of opioid use and withdrawal syndrome. Further studies are required to clarify this issue.
In conclusion, this study suggests that OWS is not uncommon in mechanically ventilated adult patients who received continuous infusion of opioids for > 3 days. The most common symptoms were a change in respiratory or pulse rate in all patients. The use of morphine may be associated with a decreased risk of OWS. Further prospective studies are required to confirm these preliminary results.
Go to :
 XML Download
XML Download