

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Patients who received intensive care regardless of the reason for admission often experience various complications after hospital discharge, including physical, cognitive, and mental health impairments, which are collectively known as post-intensive care syndrome.1 Moreover, these complications have patients experience persistent physical disability for a long time resulting in poor prognosis and low quality of life.23
Studies show that rehabilitation is not only feasible456 but able to improve physical function of patients, reduce delirium, decrease the duration of mechanical ventilation, and reduce length of stay in the hospital and intensive care unit (ICU).578910 Early rehabilitation interventions such as mobilization, passive and active exercise, training of activities of daily living, and neuromuscular electrical stimulation (NMES) improved outcomes of critically ill patients.1112 Lack of early ICU mobility therapy in survivors of respiratory failure requiring mechanical ventilation was associated with increased rates of hospital readmission or death within 12 months of hospital discharge.13
However, there is limited evidence regarding the utilization of rehabilitation at ICU evaluating patients recovering from critical illness.1415161718 The study aims to evaluate the utilization of rehabilitation resources among critically ill patients during hospital admission and its impact on health outcomes.
METHODS
Study population
We conducted a retrospective cohort analysis of the Health Insurance and Review Assessment (HIRA) database from the Korean Ministry of Health. Because Korea has a single-payer national health system, the Korean government covers approximately 97% of Koreans, with the remaining 3% who cannot afford national insurance being covered by the Medical Aid Program (MAP).19 Claims submitted for reimbursement to the Korean National Health Insurance (KNHI) and MAP are reviewed by HIRA, a central office in the Korean Ministry of Health. Therefore, the HIRA database used in this study covered virtually all ICU admissions in Korea between January 1, 2008 and May 31, 2015.
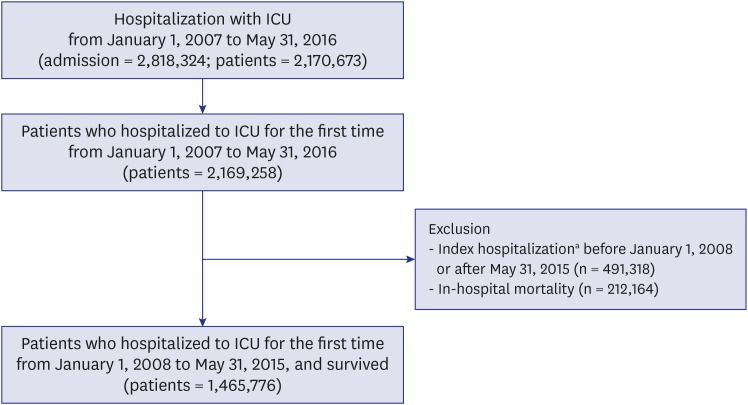
We selected patients > 18 years of age and who hospitalized to ICU for the first time from January 1, 2007 to May 31, 2016 (n = 2,169,258). We excluded patients whose hospitalization period including before January 1, 2008 or after May 31, 2015 (n = 491,318) and died during the initial hospitalization (n = 212,164). The final sample therefore included 1,465,776 patients: 836,584 men and 629,192 women (Fig. 1).
Data collection
We defined ICU admissions based on claim codes that hospitals in Korea are required to use when submitting cost claims to HIRA for ICU management during in-hospital stays (codes AJ100-AJ590900). These codes are based on the Korean Classification of Diseases 6th edition, which is a modified version of the International Classification of Diseases 10th revision, adapted for use in the Korean health system.20 All ICU stays during the same hospitalization were considered a single ICU admission. Similarly, hospital stays separated by < 2 days were considered the same hospital admission.
Rehabilitation therapies during ICU admission included NMES (KNHI procedure codes MM060, MM151), occupational (MM111–MM114), physical (MM101, MM102, MM105, MM301, MM302), respiratory (MM290, MM360, MM430), or swallowing (MX141, MZ008) therapies. In terms of outcomes, emergency room (ER) visit or readmission to the ICU after the initial hospital discharge was included.
Information on comorbidities, procedures, prescriptions, and demographic characteristics was based on claim codes. Comorbidities were defined using 10th revision of the International Statistical Classification of Diseases and Related Health Problems (ICD-10) codes,21 and summarized using the Charlson Comorbidity Index (CCI).2223 Patients with neurologic or neuromuscular disorders defined as patients with central nerve system disease (cerebrovascular disease [CVD], hemiplegia, and brain tumor; G45, G46, H34, I60-I69, G801, G802, G81, G830-834, C70, C71) or with spinal cord disease (paraplegia and spinal tumor; G82, G041, G114, G800, G839). Procedures of interest included mechanical ventilation (M5850, M5857, M5858, M5860), intermittent hemodialysis (O7020), peritoneal dialysis (O7062), continuous renal replacement therapy (CRRT; O7051–7054), and extracorporeal membrane oxygenation (ECMO; O1901–O1904). We identified the use of vasopressor drugs and antimicrobial agents using Korean Drug and Anatomical Therapeutic Chemical Codes.24
Hospitals were classified according to their capacity based on the number of hospital beds and a number of specialties, as defined by the Korean Health Law.25 A hospital was defined as a healthcare institution with more than 30 inpatient beds. Nursing care hospital was a hospital providing long-term inpatient stays. The general hospital was a hospital with more than 100 beds and more than seven specialty departments, including internal medicine, surgery, pediatrics, obstetrics and gynecology, anesthesiology, pathology, and laboratory medicine. The tertiary hospital was a general hospital with more than 20 specialty departments that serve as a teaching hospital for medical students and nurses. Departments were classified as medical and surgical. Medical departments included general medicine, internal medicine, neurology, psychiatry, pediatrics, dermatology, radiology, radiation oncology, clinical pathology, tuberculosis, rehabilitation medicine, family medicine, emergency medicine, industrial medicine, preventive medicine, and conservative dentistry. Surgical departments included general surgery, orthopedic surgery, neurosurgery, thoracic and cardiovascular surgery, plastic surgery, anesthesiology, obstetrics and gynecology, ophthalmology, otorhinolaryngology, urology, and oral surgery. The total cost of hospitalization, including ICU stay, was the amount of money reimbursed by KNHI to the hospitals and patients for medical services endorsed by HIRA.
Statistical analysis
Mean and standard deviation or median and interquartile range were used to describe the distribution of continuous variables. We used the χ2 test and Student's t-test to compare categorical and continuous variables, respectively. We calculated hazard ratios (HRs) with 95% confidence intervals (CIs) using a proportional hazards regression model for ER visits and ICU readmissions. In the model, we adjusted for age, gender, CCI, type of hospital, type of admission, and use of mechanical ventilation, ECMO, or vasopressor drugs to account for potential confounding factors between patients with and without rehabilitation. We examined the proportional hazards assumption using plots of the log (-log) survival function and Schoenfeld residuals. All statistical analyses were performed using SAS Visual Analytics (SAS Institute INC, Cary, NC, USA).
RESULTS
Among the 1,465,776 patients, 249,918 (17.1%) received rehabilitation therapy during their hospital stay that included an ICU admission (Table 1). Compared to patients without rehabilitation therapy, those who received rehabilitation therapy were older, had a higher CCI, were more likely to be admitted to a tertiary hospital and surgical department via the ER, and were more likely to receive major treatments (mechanical ventilation, intermittent hemodialysis, peritoneal dialysis, CRRT, or ECMO) during their hospital admission (Table 2). The mean ICU (median 8 vs. 2 days, P < 0.001) and hospital length of stay (median 33 vs. 11 days, P < 0.001) was longer in participants who received rehabilitation therapy than in patients without rehabilitation. In addition, the total hospitalization cost was higher in participants who underwent rehabilitation therapy than in those who did not (median 8,859 vs. 4,640 dollars, P < 0.001).
Table 1
Characteristics of surviving ICU patients according to rehabilitation therapy in Korea, January 2008 to May 2015
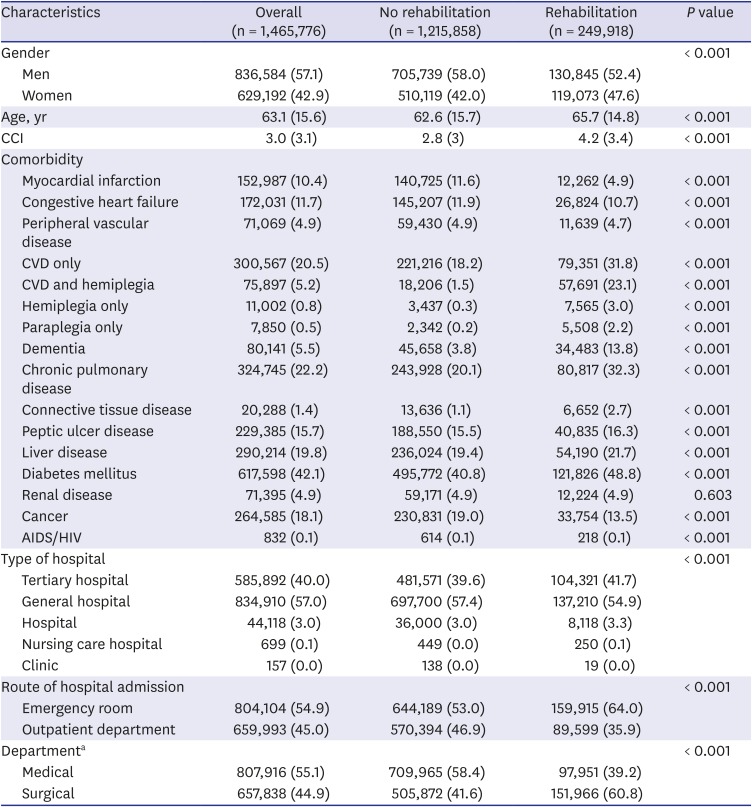
Values are presented as frequency (%), except for age and CCI (mean [standard deviation]).
ICU = intensive care unit, CCI = Charlson Comorbidity Index, CVD = cerebrovascular disease, AIDS = acquired immune deficiency syndrome, HIV human immunodeficiency virus.
aMedical includes general medicine, internal medicine, neurology, psychiatry, pediatrics, dermatology, radiology, radiation oncology, clinical pathology, tuberculosis, rehabilitation medicine, family medicine, emergency medicine, industrial medicine, preventive medicine, and conservative dentistry. Surgical includes general surgery, orthopedic surgery, neurosurgery, thoracic and cardiovascular surgery, plastic surgery, anesthesiology, obstetrics and gynecology, ophthalmology, otorhinolaryngology, urology, and oral surgery.
Table 2
Management procedures and outcomes of surviving ICU patients according to rehabilitation therapy in Korea, January 2008 to May 2015
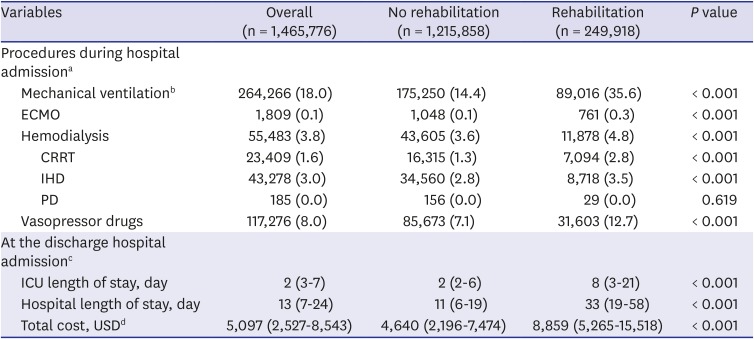
ICU = intensive care unit, ECMO = extracorporeal membrane oxygenation, CRRT = continuous renal replacement therapy, IHD = intermittent hemodialysis, PD = peritoneal dialysis.
aValues are presented as frequency (%); bMechanical ventilation was defined that using for more than 3 hours; cValues are presented as median (interquartile range); d1 USD=1,158 Korean won (exchange rate as of December 1, 2015).
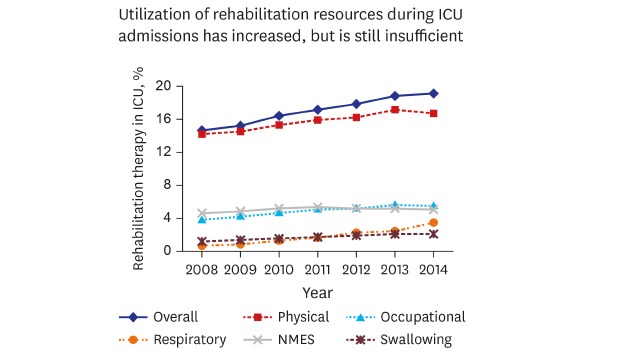
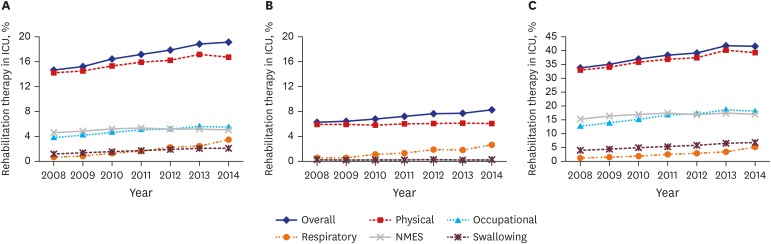
The percentage of patients receiving any rehabilitation therapy increased annually, from 14% in 2008 to 20% in 2014 (Fig. 2A). Physical therapy was received by 16% of all ICU patients, whereas other types of rehabilitation therapy were received by 5% or less of patients. Among patients receiving rehabilitation therapy, 41.5% underwent two or more different types of therapy (Supplementary Table 1). Physical therapy was received by 91.9% of patients who underwent rehabilitation therapy. A lower percentage of patients received occupational therapy (28.6%), but patients received more sessions of occupational therapy than respiratory therapy (32.1 vs. 24.8 treatments per patient) (Supplementary Table 2). Among the types of therapies, respiratory therapy was the lowest percentage in 2008, but increased during the study period. The percentage of patients receiving all other individual types of rehabilitation therapy also increased over time. In patients without neurologic or neuromuscular disorders, the percentage of patients receiving any form of rehabilitation therapy was < 10%, but the percentage of patients in this group receiving respiratory therapy increased during the study period (Fig. 2B). And, in patients with neurologic or neuromuscular disorders, the percentage of patients receiving any form of rehabilitation therapy was > 30%, indicating that rehabilitation therapy is concentrated in neurologic or neuromuscular patients (Fig. 2C). Detailed trends in rehabilitation therapy for central nerve system disease and spinal cord disease are shown in Supplementary Fig. 1.
Fig. 2
Trends in rehabilitation therapy in patients admitted to ICUs for the first time in Korea between January 2008 and May 2015. (A) Group 1 = all patients admitted to the ICU during the time period. (B) Group 2 = patients admitted to the ICU during the time period who had no neurologic or neuromuscular disorder during hospitalization or the first year after discharge. (C) Group 3 = patients admitted to the ICU during the time period who had cerebrovascular disease, paraplegia/hemiplegia, or brain/spinal cord tumor during hospitalization or the first year after discharge.
ICU = intensive care unit, NMES = neuromuscular electrical stimulation.
During the 30-day post-discharge follow-up period, 80,416 patients readmitted to the ICU and 138,766 patients revisited to the ER. Of patients who readmitted to the ICU, 13,250 (5.4%) had received rehabilitation therapy during their initial admission, whereas 67,166 (5.7%) had no rehabilitation therapy (Table 3). Of patients who revisited to the ER, 23,622 (9.6%) had received rehabilitation therapy during their initial admission, whereas 115,144 (9.7%) had no rehabilitation therapy. After adjusting for confounding variables, the risk of ICU readmission (adjusted HR, 0.70; 95% CI, 0.65–0.75) and revisit to the ER (adjusted HR, 0.83; 95% CI, 0.77–0.88) were significantly lower in patients who received rehabilitation therapy than in patients without rehabilitation. In addition, we analyzed readmission to the ICU and revisit to the ER in patients without neurologic or neuromuscular disorder. After adjusting for confounding variables, the risk of ICU readmission (adjusted HR, 0.86; 95% CI, 0.76–0.98) was significantly lower in patients who received rehabilitation therapy than in patients without rehabilitation.
Table 3
HRs (95% CIs) for post-discharge 30-day outcomes associated with rehabilitation among patients who survive in ICU (n =1,418,811)a

HR = hazard ratio, CI = confidence interval, ICU = intensive care unit.
aNo insurance claim records were available after discharge for 36,965 patients (32,180 in the no rehabilitation group and 4,785 in the rehabilitation group); bAdjusted for age, gender, comorbidities (myocardial infarction, congestive heart failure, peripheral vascular disease, cerebrovascular disease, dementia, chronic pulmonary disease, connective tissue disease, peptic ulcer disease, liver disease, diabetes, renal disease, and cancer), tertiary hospital, admission type, mechanical ventilation, extracorporeal membrane oxygenation, and vasopressor drugs.
DISCUSSION
This study showed that in-hospital rehabilitation for critically ill patients was associated with an 30% reduction in risk of ICU readmission, and 17% reduction in risk of ER visit within the 30-day following discharge. However, only approximately 17% of our ICU survivors received any type of rehabilitation therapy during their hospital stay, and they were more likely to be older and in poorer physiological condition than those who did not undergo rehabilitation therapy. From 2008 to 2014, the overall percentage of patients receiving rehabilitation therapy steadily increased, and the percentages for each rehabilitation therapy also increased over time.
In a prospective, cohort study (the Improving Care of Acute Lung Injury [ALI] Patients study) conducted between 2004 and 2007 in the United States, 36% of mechanically ventilated patients with ALI received physical therapy in the ICU.26 In recent multicenter studies, physical therapy services provided by dedicated staff were available to all ICU patients as part of standard ICU care.141827 By contrast, the percentage of critically ill patients who received any type of in-hospital rehabilitation in our current study was low (17%) and consisted primarily of physical therapy. Our results, therefore, demonstrated a paucity of rehabilitation resources or comprehensive rehabilitation management in critical care facilities in Korea. Indeed, the availability of physical and occupational therapists represented a major barrier to the delivery of therapy in earlier studies.1028 Previous implementing projects also considered the lack of staff, equipment, and physician referrals for physical therapy as barriers to ICU rehabilitation therapy.5929
After adjusting for confounding factors, we found that the percentage of ICU readmissions during 1-year follow-up was significantly lower in patients receiving rehabilitation therapy. In a recent meta-analysis, active mobilization and rehabilitation in the ICU were associated with more days alive and out-of-hospital up to day 180.30 Since patients admitted to an ICU are more likely than non-ICU patients to visit the ER and be readmitted to the hospital and ICU,31 these results suggest that ICU or overall in-hospital rehabilitation therapy can provide meaningful benefits to ICU survivors concerning healthcare utilization after discharge. However, the percentage of ER visits was similar in our two patient groups. Considering that our overall ER visit rate of 22.8% was much lower than that of previous reports (e.g., 46% within the first 6 months post-discharge, as per Hill et al.31), but our overall ICU readmission rate (13.9%) was similar to previously reported rates (e.g., 10% within the first year post-discharge, as per Garland et al.32), we assume that ER visits are more likely than ICU admissions to be influenced by various healthcare system factors or patient factors not directly related to health status.
Compared to patients without rehabilitation therapy, those who received rehabilitation therapy were older, had a higher CCI, were more likely to be admitted a tertiary hospital and surgical department via the ER, were more likely to receive major life-sustaining treatments, and stayed longer in the ICU and hospital. These results reflect the actual situation of ICU rehabilitation in Korea. Under the Korean health system, therefore, rehabilitation prescribed for patients who can charge medical insurance cost of rehabilitation therapy rather than medical needs for rehabilitation. Increased rehabilitation therapy in patients with CVD in this study might be related with the Korean insurance systems.
In the current study, marked differences in rates of neurologic comorbidities, including CVD, dementia and paraplegia/hemiplegia, existed between patients who did and did not receive rehabilitation therapy. Indeed, this preferential use of rehabilitation therapy in patients with neurologic disorders is not unusual. In a national survey of physical therapists in the United States using six different ICU patient scenarios, physical therapy was more likely to be routinely and intensively provided for the two neurologic patient scenarios than for three medical patient scenarios.16 In a nationwide cohort study in Taiwan, ICU survivors receiving post-discharge rehabilitation therapy were more likely to exhibit neurologic comorbidities than those without rehabilitation, despite only patients with sepsis being included in the study.33 Rehabilitation therapy may be more common in patients with neurologic disorders because many of these patients have a physical disability, which is one of the most common indications for rehabilitation. However, the preferential use of rehabilitation therapy in patients with neurologic conditions was more pronounced than in previous studies, like CVD, dementia, and paraplegia/hemiplegia was 2.8, 3.6, and 14.9 fold more common, respectively, in patients who received rehabilitation therapy compared with patients who did not undergo rehabilitation. In addition, utilization rates of rehabilitation therapy and each type of therapy when excluding patients with neurologic or neuromuscular disorders more clearly demonstrated the priority for neurorehabilitation (Fig. 2). In Korea, early rehabilitation in acute stroke patients is encouraged as a part of the Value Incentive Program of HIRA. In addition, KNHI guarantees a wider range of therapies and higher reimbursement costs for rehabilitation therapies for patients with neurologic disorders than for patients with other medical disorders. It is possible that these healthcare system factors influenced the preferential use of in-hospital rehabilitation in neurology patients.
This is the first Korean nationwide cohort study to investigate actual clinical practice related to the use of rehabilitation therapy in critical care, including 1,465,776 adult ICU survivors. In Korea, rehabilitation has not yet become standard practice in critical care because of its relatively recent implementation.34 In addition, most ICUs do not have dedicated therapists, and use of rehabilitation therapy depends on consultation because of its expense and restricted institutional prescription authority (related to the physician’s specialty). Most previous studies used a controlled design and thereby potentially deviated from usual clinical practice because of their focus on short-term, intensive administration of resources and early rehabilitation in the ICU.5710 Although some nationwide surveys of rehabilitation practice in other countries have been published, it is possible that only ICUs with sufficient resources or interest in early mobilization participated in these studies.1415161718 By contrast, our HIRA database is more likely to provide comprehensive, unbiased, and objective information regarding the epidemiology of rehabilitation. It did not restrict study participants to a specific disease group and did not rely on observations or responses of particular examiners for data acquisition. The large sample size and an extended follow-up period were additional strengths of our study.
This study has limitations. First, the amount and timing of rehabilitation therapies were not clearly determined. The HIRA only reviews claims for the entire hospital admission period and does not distinguish between time in the ICU or on the general ward. Second, the HIRA database consists of claims for reimbursement and, therefore, does not provide information regarding behavioral factors, psychosocial status, laboratory results, or mortality. Also, the effects of activities that do not incur direct costs, such as basic nursing care, were not excluded. Finally, although a single payer national health system with largely private provision of healthcare in Korea has made this comprehensive analysis possible, our results may not be generalizable to other countries with different healthcare systems.
In conclusion, this study identified increasing, but still insufficient, utilization of rehabilitation resources in critical care in Korea. Nonetheless, rehabilitation therapy during hospitalizations including an ICU admission appears to positively impact outcomes in ICU survivors—the rate of ICU readmission and ER visit. Despite the effectiveness of rehabilitation therapy for critically ill patients, there are practical limitations due to insufficient medical resources for ICU rehabilitation. To overcome practical limitations, sufficient medical insurance cost of rehabilitation for critically ill patients should be needed. Although future prospective studies will be needed to verify the effectiveness of rehabilitation therapy for critically ill patients, our results underline the potential importance of rehabilitation therapy for critically ill patients. To implement rehabilitation as routine practice, and thereby improvement outcomes, overall consideration should be given to various factors, including those related to physicians and specific healthcare systems.
 XML Download
XML Download