

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Chronic hepatitis B virus (HBV) infection is a public health problem affecting more than 400 million people worldwide.1 If untreated, chronic hepatitis B (CHB) is likely to progress to advanced liver diseases, such as liver cirrhosis, hepatic decompensation and hepatocellular carcinoma (HCC), resulting in more than 600,000 deaths every year.2 Indeed, patients with HBV-related cirrhosis have a high risk of developing HCC, and its incidence rate is approximately up to 8% per year.3 Therefore, the primary therapeutic goal of CHB is to improve the long-term prognosis by preventing disease progression through potent viral suppression.
Accordingly, in the current international guidelines,456 nucleos(t)ide analogues with a high genetic barrier to resistance, such as entecavir (ETV), tenofovir disoproxil fumarate (TDF), and tenofovir alafenamide (TAF), are recommended as the first-line antiviral therapy (AVT).1 Especially in Korea, in addition to ETV, TDF, and TAF, besifovir dipivoxil maleate (BSV) with L-carnitine supplementation is also recommended as a first-line agent.4 BSV is a potent acyclic nucleoside phosphonate, which is converted into an active metabolite, a nucleos(t)ide analogue of guanosine monophosphate that inhibits HBV replication.7 Recent clinical trials have shown that BSV with L-carnitine supplementation effectively suppresses HBV replication,8910 and that the antiviral efficacy and safety of BSV are comparable to those of TDF.11
Approximately, 14%–70% of cases, hepatic steatosis (HS) was noted among patients with CHB.12 Controversial interaction between HS and CHB has been reported.13 Some studies have shown that CHB is not a protective factor against fatty liver.14 Another Asian study has demonstrated that the level of hepatitis B surface antigen (HBsAg) in the liver decreased as the severity of HS worsened.15 In contrast, an unfavorable impact of HS in patients with CHB includes the facilitation of progression to advanced liver disease.1617 Moreover, a recent study has shown that the presence of metabolic syndrome is closely associated with HS, and is an independent risk factor for cirrhosis and HCC among patients with CHB.1819 All these signify that assessment and management of co-existing HS in patients with CHB are important.
L-carnitine (L-beta-hydroxy-g-N-trimethylaminobutyric acid), used in combination with BSV, is an essential nutrient that promotes the migration of long-chain fatty acids and converts fat into mitochondrial energy. Administration of L-carnitine improves or prevents hepatic damage with various causes.20 Carnitine reduces intrahepatic lipid accumulation, increases the expression of metabolic products associated with β-oxidation, and significantly reduces fatty acid levels in the liver.21 Carnitine also ameliorates the inflammation caused by non-alcoholic fatty liver disease (NAFLD). Furthermore, carnitine and vitamin complex supplementation reduce the serum levels of aspartate aminotransferase (AST), alanine aminotransferase (ALT), and total bilirubin in patients with NAFLD.22 In a clinical study, BSV reduced the serum L-carnitine level in 94.1% of 114 patients, and the level normalized after taking L-carnitine supplements.7
Thus, we investigated whether BSV combined with L-carnitine could improve HS when compared to ETV and TDF, and identified the independent predictors of improvement of HS in patients with CHB.
METHODS
Study participants
Between November 2017 and October 2018, 617 treatment-naïve patients with CHB who were initiated on AVT at Severance Hospital, Yonsei University College of Medicine (Seoul, Korea) were considered eligible for this retrospective cohort study. CHB was defined as the persistent presence of serum HBV surface antigen (HBsAg) for at least 6 months. The exclusion criteria were as follows; 1) patients who were initiated on AVT except BSV, ETV, and TDF, 2) HCC at enrollment or any such previous history, 3) decompensated liver disease at enrollment or any such previous history, 4) liver transplanted status at enrollment or any such past medical history, 5) insufficient laboratory information, 6) treatment duration ≤ 6 months, 7) use of medication potentially associated with fatty liver, 8) history of any other malignancy.
Enrollment and follow-up
AVT was administered according to the treatment guidelines of the Korean Association for the Study of the Liver and the reimbursement guidelines of the National Health Insurance Service of Korea.4 After AVT initiation, each patient was followed up after 3–6 months and underwent laboratory tests and ultrasonographic evaluation.
Estimation of HS and liver fibrosis
In addition to ultrasonographic assessment, the magnitude of HS was assessed using hepatic steatosis index (HSI). The equation used for the calculation of HSI is as follows: HSI = 8 × ALT /AST + BMI + 2, if diabetes mellitus is present; + 2, if the patient is female; values ≥ 36 suggest fatty liver.23 In this study, the HS improvement was defined as ≥ 10% reduction in HSI from the baseline. The HSI formula was developed based on a logistic regression model, in a retrospective cohort study that excluded patients with chronic liver diseases including CHB infection.23 However, HSI has acceptable diagnostic accuracy for both patients with CHB and the general population (area under the receiver operating characteristic curve, 0.65–0.79). These findings support the use of HSI to assess the degree of fatty liver in patients with CHB.2425 Besides, the degree of hepatic fibrosis was identified using the fibrosis-4 index (FIB-4 index). The equation used for the calculation of FIB-4 index is as follows: FIB-4 index = (Age × AST) / (PLT × √ALT).26
Statistical analyses
All statistical analyses were conducted using IMB SPSS software, version 25.0 (SPSS Inc. Chicago, IL, USA) for Windows. The continuous variables were expressed as the mean ± standard deviation (SD), and the categorical variables were presented as frequencies with percentages. To examine the differences between the two groups, the continuous variables were compared using Student's t-test or Mann-Whitney U test and the categorical variables were compared using χ2 test or Fisher's exact test. Changes in variables between baseline and follow-up were analyzed by paired t-test. The variables that were statistically significant in the univariate analysis were added to a multiple logistic regression model to identify the independent predictors of HS improvement from the baseline. Statistical significance was considered for comparisons with a two-tailed P value of < 0.05.
A sample size of 275 (24 in the BSV group and 251 in the ETV or TDF group) achieved 93% power to detect a between group-difference of 0.25, at a significance level of 0.05. In the initial analysis, we assumed the rate of significant reduction in HSI in the control group (ETV or TDF) would be around 0%, so we set the proportion of reduction in HSI in the control group as 0.05. The proportion of reduction in HSI in BSV group was assumed to be 0.05 under the null hypothesis and 0.30 under the alternative hypothesis.
Ethics statement
The study was approved by the Institutional Review Board (IRB) of Severance Hospital, Yonsei University Health System (IRB 4-2020-0034) and was performed according to the ethical guidelines of the 1975 Helsinki declaration. The requirement of informed consent was waived due to the retrospective nature of this study.
RESULTS
Baseline characteristics
Among the 617 treatment-naïve patients with CHB who started AVT between November 2017 and October 2018, 588 patients who started AVT consisting of BSV, ETV, or TDF were considered. After excluding 313 patients according to the exclusion criteria, 275 patients were finally selected for the statistical analysis (Fig. 1). The baseline characteristics of the study population are described in Table 1. The mean age was 56 years, with a male predominance (n = 178, 64.7%). Diabetes, hypertension, and liver cirrhosis were identified in 31 (11.3%), 57 (20.7%), and 82 (29.8%) patients, respectively. The mean BMI, AST, ALT, and platelet count were 23.5 kg/m2, 49.6 IU/L, 49.0 IU/L, and 191.3 × 109/L, respectively. The mean HSI and FIB-4 index were 32.6 and 0.5, respectively. While fatty liver was identified in 14 (5.1%) patients based on the ultrasonographic evaluation, it was diagnosed in 66 (23.6%) patients by HSI.

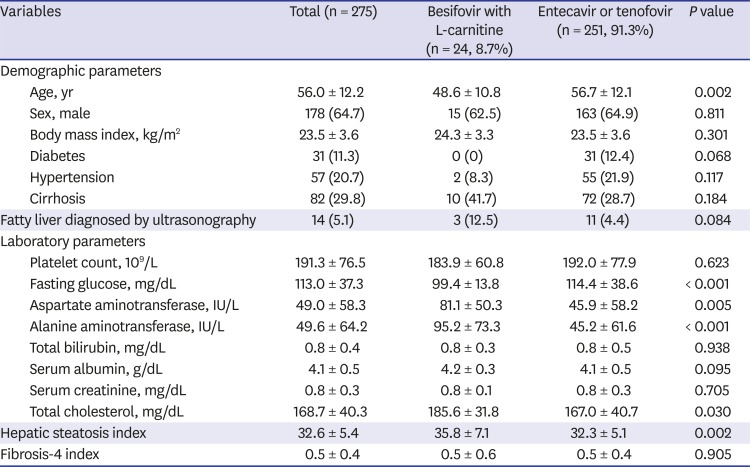
Fig. 1
Recruitment and follow-up algorithm. A total of 617 treatment-naive patients with CHB who started antiviral therapy between November 2017 and October 2018. However, 29 patients who started antiviral therapy except BSV, ETV, and TDF were excluded. Moreover, 313 patients were excluded according to our exclusion criteria. Finally, 275 patients were finally selected for the statistical analysis.
CHB = chronic hepatitis B, BSV = besifovir, ETV = entecavir, TDF = tenofovir, HCC = hepatocellular carcinoma.
![]()
Table 1
Baseline characteristics of the study population (n = 275)
![]()
Comparison between patients with BSV and those with ETV or TDF
Of the study population, only 24 (8.7%) patients started AVT consisting of BSV with L-carnitine, whereas the other 251 (91.3%) started with ETV (n = 154, 56.0%) or TDF (n = 97, 35.3%). The patients in the BSV group were significantly younger (mean, 48.6 vs. 56.7 years), and had lower fasting glucose level (mean, 99.4 vs. 114.4 mg/dL), higher AST level (mean, 95.2 vs. 45.2 IU/L), higher ALT level (mean, 81.1 vs. 45.9 IU/L), and higher total cholesterol level (mean, 185.6 vs. 167.0 mg/dL) (all P < 0.05) than those in the ETV/TDF group (Table 1). The proportion of patients with fatty liver diagnosed by ultrasonography was higher in the BSV group than those in the ETV/TDF group (12.5% vs. 4.4%, P = 0.084). When HSI was used to define HS, the proportion of patients with fatty liver was higher in the BSV group than those in the ETV/TDF group (n = 11 [45.8%] vs. n = 55 [21.9%]; P = 0.998) (Table 1).
When patients in the BSV group were compared to those in the ETV or TDF group, respectively, similar findings were observed, except similar fasting glucose level (Supplementary Table 1).
Changes in the laboratory variables, HSI, and FIB-4 index after 6 months of AVT
After 6 months of AVT, platelet count (mean, 191.3 → 167.0 × 109/L), fasting glucose (mean, 113.1 → 105.9 mg/dL), AST (mean, 49.6 → 28.0 IU/L), ALT (mean, 49.0 → 33.9 IU/L), and total cholesterol (mean, 170.0 → 162.1 mg/dL) levels were significantly decreased (all P < 0.05) (Table 2). The HSI significantly decreased (mean, 32.6 → 31.4; P < 0.001), whereas the FIB-4 index significantly increased (mean, 0.5 → 0.6; P < 0.001) after 6 months of AVT.
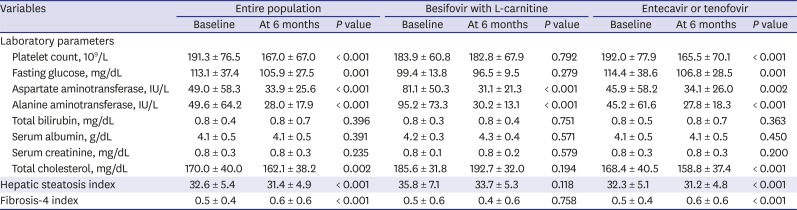
Table 2
Changes in laboratory parameters, hepatic steatosis index, and fibrosis-4 index after 6 months of antiviral therapy
![]()
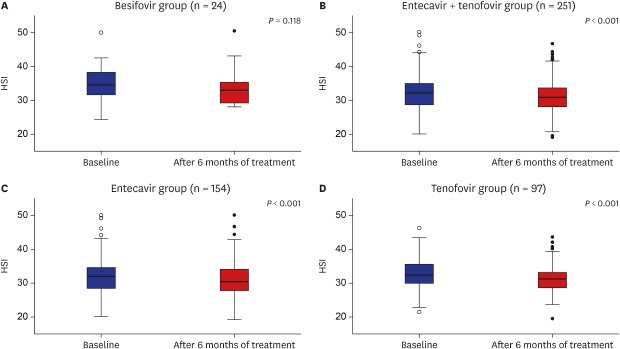
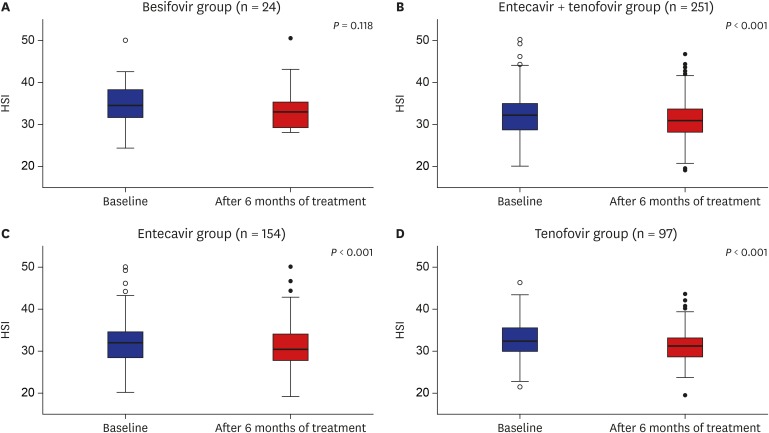
Among the patients in the BSV group, AST (mean, 95.2 → 30.2 IU/L), and ALT (mean, 81.1 → 31.1 IU/L) levels significantly decreased (all P < 0.05), whereas HSI and FIB-4 index were maintained (all P > 0.05) (Table 2). Among patients in the ETV/ TDF group, platelet count, fasting glucose, AST and ALT levels, total cholesterol, HSI, and FIB-4 index were significantly changed (all P < 0.05) (Table 2). The respective changes in the laboratory parameters, HSI, and FIB-4 index according to ETV and TDF are enumerated in Supplementary Table 2. The changes in HSI according to the antiviral agents are depicted in Fig. 2.
Independent predictors of treatment outcomes
Univariate and subsequent multivariate analyses were performed to identify the independent predictors of improvement of HS (Table 3). In the univariate analysis, age, BMI, diabetes, cirrhosis, fasting glucose level, and ALT level were significantly associated with improvement of HS (all P < 0.05). In the subsequent multivariate analysis, lower BMI (odds ratio [OR], 0.816; 95% confidence interval [CI], 0.727–0.917; P = 0.001), diabetes (OR, 3.272; 95% CI, 1.089–9.825; P = 0.035), absence of cirrhosis (OR, 0.351; 95% CI, 0.135–0.909; P = 0.031), higher fasting glucose level (OR, 1.013; 95% CI, 1.002–1.025; P = 0.019), higher ALT level (OR, 1.040; 95% CI, 1.023–1.064; P < 0.001) were significantly associated with the higher probability of HS improvement after 6 months of AVT. However, BSV with L-carnitine supplementation as compared to ETV or TDF was not associated with the probability of HS improvement (P = 0.415).
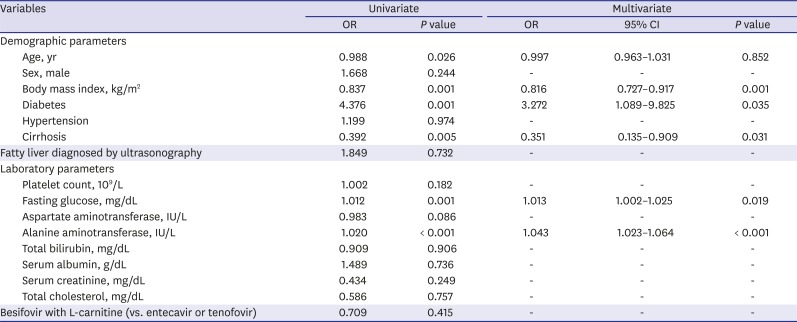
Table 3
Binary logistic regression to identify predictors of improvement of hepatic steatosis (≥ 10% reduction in hepatic steatosis index from the baseline) after 6 months of antiviral therapy
![]()
When 66 (23.6%) patients with fatty liver based on HSI > 36 at baseline, who might benefit from HS improvement, were selected for a subgroup analysis, only higher ALT level (OR, 1.214; 95% CI, 1.017–1.449; P = 0.032) was independently associated with the higher probability of HS improvement (Table 4). When 8 patients with fatty liver diagnosed by ultrasonography were further added (n = 74, 26.9% in total), only higher ALT level (OR, 1.228; 95% CI, 1.025–1.470; P = 0.026) was independently associated with the higher probability of HS improvement (Supplementary Table 3).
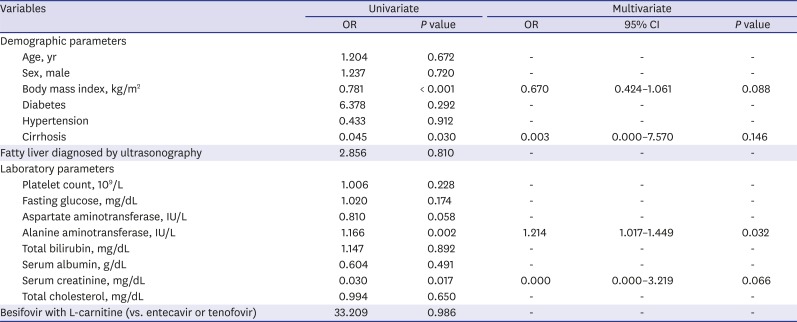
Table 4
Binary logistic regression to identify predictors of the improvement of hepatic steatosis after 6 months of antiviral therapy among the patients with fatty liver based on HSI > 36
Improvement of hepatic steatosis was defined as a ≥ 10% reduction in the HSI score from the baseline.
HSI = hepatic steatosis index, OR = odds ratio, CI = confidence interval.
![]()
DISCUSSION
Current Korean guidelines for the treatment of CHB recommend BSV as a first-line AVT agent, together with ETV, TDF, and TAF.4 However, a recent clinical study showed that BSV reduced the serum L-carnitine level in 94.1% of 114 patients, although the level normalized after taking L-carnitine supplements.7 Thus, carnitine supplementation was routinely applied to all patients taking BSV. In living cells, L-carnitine transports fatty acids from the cytosol into the mitochondria during the breakdown of lipids, for the generation of energy.21 Moreover, carnitine administration prevents hepatic damage by reducing intrahepatic fat accumulation and inflammation.202122 Because L-carnitine is an essential nutrient involved in fatty-acid metabolism that protects the liver, we hypothesized that L-carnitine plus BSV would affect the hepatic fat burden in patients with CHB.
During the 6 months follow-up period, univariate and subsequent multivariate analyses found that BSV with L-carnitine supplementation did not show a significant reduction in the amount of hepatic fat estimated by HSI as compared to that with ETV or TDF. In the subgroup of patients with fatty liver (HSI > 36) or those with fatty liver diagnosed by ultrasonography or HSI > 36, BSV with L-carnitine supplementation was not significantly associated with an improvement in HS.
Our study has several strengths. First, to the best of our knowledge, despite the negative results, this is the first study to investigate the potential effects of BSV and L-carnitine on fatty liver. To date, L-carnitine has been known to be effective for improving fatty liver.21 However, because the primary aim of L-carnitine supplementation is to compensate for L-carnitine deficit caused by BSV, our clinical setting was different from those of the other previous studies,21 which supports the clinical implication of our current study.
Second, we investigated the effects of BSV and L-carnitine on fatty liver using the control group of patients treated with ETV and TDF, which were previously administered as the first line agents. In contrast to the BSV group, ETV and TDF group showed a decline in the platelet count and an increment in FIB-4 index, which is an unexpected phenomenon with AVT using high-potent antiviral agents. In addition, baseline AST and ALT levels, which are the key factors for calculating HSI and FIB-4 index, were significantly different between the BSV and ETV/TDF groups. This might be a reason for the potential false negative results in the BSV group. Therefore, well-designed prospective randomized trials with a large sample size are required.
Third, we tried to find independent predictors for HS improvement. Higher BMI and presence of cirrhosis were independently associated with the lower probability of HS improvement. The exact reason for this phenomenon is not clear. Among the various mechanisms associated with HS development, obesity is a major associated risk factor.27 Thus, the result of this study can be partly explained by the fact that L-carnitine supplementation might not be sufficient to improve HS when the fat burden outside the liver is high. In addition, cirrhosis with structural and functional abnormality might be associated with poor response to L-carnitine and poor mobilization of hepatic fat. However, further validation studies are required to elucidate these assumptions. In another study, patients with non-alcoholic steatohepatitis (NASH) were found to be at increased risk for liver fibrosis, cirrhosis, and HCC.28 Patients with lower BMI and without diabetes or cirrhosis showed improvement in HS. Because fasting glucose or ALT levels are associated with diabetes or cirrhosis, an improvement in HS is found with low glucose or ALT levels.
This study had several limitations. First, the size of the BSV and ETV/TDF groups differed significantly (n = 24 vs. 251). This may have hampered detection of a beneficial effect, as indicated by the non-significantly higher mean reduction in HSI in the BSV group (35.8 to 33.7) versus the ETV/TDF group (32.3 to 31.2). Moreover, the follow-up treatment period (6 months) may have been insufficient to fully determine the effect of L-carnitine on fatty liver. Therefore, larger-scale long-term clinical studies are needed to confirm the effects of BSV with L-carnitine on fatty liver in patients with CHB. Second, although recent studies partially support the use of HSI to assess the degree of fatty liver in patients with CHB,2930 no evidence is available on whether HSI is appropriate for patients with CHB, especially those with elevated liver enzyme levels who require antiviral therapy. In addition, the clinical implications of a reduction in the HSI score of > 10% from the baseline are unclear. Furthermore, because only 10 patients underwent paired transient elastography, our results could not be reproduced with controlled attenuation parameters. Also, because this was a retrospective study, we were unable to analyze the serum L-carnitine level. Thus, unfortunately, we cannot confirm that our findings are due to the effect of L-carnitine. In further studies, changes in histological status should be assessed, or more reliable noninvasive surrogates and assessment of the serum carnitine level during BSV treatment should be implemented. Third, as this was a retrospective study performed in a single tertiary academic institute, the results might not be applicable to the general population. Indeed, the proportion of patients diagnosed with fatty liver was only 5.1%, lower than the prevalence rate of fatty liver in Korea (26%–40%).3132 Similarly, the proportion of patients with HSI-based fatty liver was 23.6%, lower than the prevalence rate of HSI-based fatty liver in Korea (64.3%).33 Finally, the frequency of a significant improvement in HSI was unexpectedly high in the control group (ETV or TDF treatment), which may explain the potential false-negative results in the BSV group. The reduction in total cholesterol level in patients on ETV or TDF (mean, 168.4 → 158.8 mg/dL) was greater than that in those on BSV (mean, 185.6 → 192.7 mg/dL), which might explain the significant reduction in HSI in the ETV and TDF groups. However, further randomized prospective studies including large populations are needed to confirm this finding.34
In conclusion, BSV and L-carnitine did not show improvement of HS in patients with CHB receiving BSV combined with L-carnitine supplementation. However, further prospective randomized controlled trials are required to elucidate the potential beneficial effects of BSV with L-carnitine supplementation in patients with CHB.
 XML Download
XML Download