

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Cavotricuspid isthmus (CTI) is the critical part of the circuit of typical atrial flutter (AFL), and catheter ablation for the bidirectional block has been an easy and safe treatment option.1)2)3) Atrial fibrillation (AF) and AFL commonly occur in combination.4)5)6) In current ablation guidelines, both atrial ablations were recommended in cases of combined AF and documented typical AFL.7) However, documentation of paroxysmal AFL is difficult, and some patients can have asymptomatic or undocumented episodes of AFL. These patients would benefit from additional ablation for CTI. Some patients with AF and AFL did benefit from CTI ablation alone and not from pulmonary vein isolation.8) This finding suggested that typical AFL could trigger AF, and ablation for CTI could reduce AF. A small randomized study reported that additional ablation for CTI has no impact on the one-year recurrence rate of AF or AFL.9) The present study is a large, long-term follow-up randomized trial to investigate the effect of prophylactic CTI ablation in patients without previous or induced AFL.
Go to : 
METHODS
Study population
The prophylactic CTI trial was a prospective, multicentre, randomized, single-blind, controlled trial to assess the role of preemptive CTI block during radiofrequency catheter ablation (RFCA) for paroxysmal atrial fibrillation (PAF). From January 2013 to June 2017, patients with AF referred for RFCA at tertiary hospitals (Seoul St. Mary's Hospital, Severance Hospital, and Asan Medical Center) had been screened. All enrolled patients provided written informed consent. Inclusion criteria were ≥18 years of age and patients undergoing RFCA for PAF. The exclusion criteria were a history of AFL, previous RFCA for AF, previous MAZE surgery, induced typical AFL during an electrophysiologic study, the presence of mechanical tricuspid valve, and refusal to participate. If no typical AFL was induced, patients were randomized in a 1:1 manner to the PVI alone or the PVI plus CTI block group; using a computer-generated randomization sequence at each centre. In the case of inducible AFL after randomization, the patients were dropped. The study protocol was approved by the Institutional Review Board (Severance Hospital [2013-0666-024]) and registered at ClinicalTrials.gov (NCT02031705).
Ablation procedure
Intracardiac electrograms were recorded using the Prucka Cardio Lab electrophysiology system (General Electric Medical Systems, Milwaukee, WI, USA). Diagnostic catheters were positioned into the coronary sinus, right ventricle, and His bundle at the operator's discretion. The detailed electrophysiologic study protocol was left to the operator's decision. A double transseptal puncture approach was used to access the left atrium. Subsequently, an ablation catheter and a circumferential PV mapping catheter were inserted into the left atrium. A three-dimensional (3D) electroanatomical map was generated by NavX or Carto system. Antral ablation lines for the PVI were created with radiofrequency energy of 25–35W for 20–30 seconds. An electrophysiologic study was tried to induce AFL. Overdrive atrial pacing rate was to 200 ms. Single atrial extrastimuli were delivered. Patients allocated to the PVI plus CTI block group underwent an additional ablation at the CTI, for which the radiofrequency energy was increased to 40 W during CTI ablation. The ablation procedure was performed using radiofrequency energy with an open irrigated catheter (Coolflex, Abbott, or Thermocool, Biosense Webster). The procedure time was from femoral vein puncture to sheath out. The endpoint of ablation was a bidirectional block at the CTI by differential pacing.10)
Follow-up and outcomes
The medical treatment including anticoagulation was administered in accordance with the guidelines available at the time of the trial.11) Recurrence was defined as any episode of atrial arrhythmia that lasted longer than 30 seconds.11) The first three months after ablation were considered a blanking period in accordance with the guidelines.11) During follow-up, we performed 12-lead ECG at every visit, and 24-hour Holter tests were performed at 3, 6, and 12 months after RFCA and every 6 to 12 months thereafter. Anti-arrhythmic drugs were prescribed after RFCA at the duty physician's discretion. The primary endpoint was a recurrence of atrial arrhythmia, including AF or any AFL. The secondary endpoint was a recurrence of any AFL and typical AFL. We defined typical AFL when ECG showed saw-tooth appearance in lead II and discrete positive P wave in V1. Any AFL was defined as a constant regular and very fast flutter wave on ECG.
Statistical analysis
The assumptions for the sample size calculation was proven to be inappropriate in the previous study.9) The effect of prophylactic CTI was much lower than expected, so a larger study should be needed. We accepted a type 1 error of 5% and the statistical power was 80%. Based on the previous study, the hazard ratio of AF or AFL was expected to 0.8 for 36 months follow-up. With an expected loss of patients during follow-up, we chose to enroll 180 patients in each group. For baseline characteristics, continuous variables are presented as mean±standard deviation and compared using Student's t-tests. Categorical variables are presented as the frequency with percentages (%) and compared by the χ2 test or Fisher's exact test. Cumulative incidences of primary outcomes were estimated by Kaplan-Meier survival curves and compared with the results of log-rank tests. The p values <0.05 were considered statistically significant. All statistical analyses were performed using R version 3.3.2.
Go to :
RESULTS
Patients characteristics
Patients with PAF referred for RFCA from November 2012 to May 2017 were screened. Among these patients, 42 were excluded (refused enrollment, ten patients, and experienced typical AFL during the procedure, 32 patients). The 366 remaining patients were randomly assigned to the PVI (n=183) or the PVI plus CTI block (n=183) group. Baseline characteristics are shown in Table 1. There was no significant difference between the PVI group and the PVI plus CTI block group.
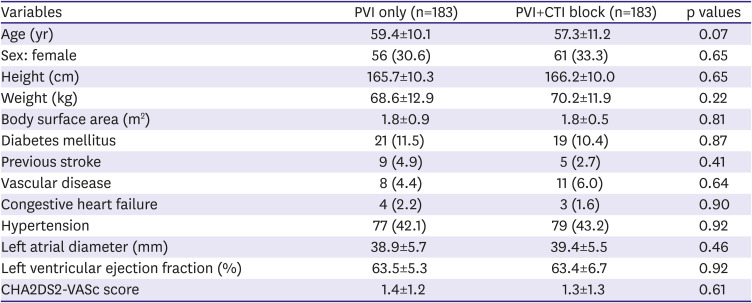
Table 1
Baseline patient demographic characteristics
Values are presented as mean±standard deviation or as number (%).
CHA2DS2-VASc = congestive heart failure, hypertension, age ≥75 yr, diabetes, stroke/transient ischemic attack, vascular disease, age 65–74 yr, and sex category; CTI = cavotricuspid isthmus; PVI = pulmonary vein isolation.
*Vascular disease included myocardial infarction, peripheral artery disease, and aortic plaque.
![]()
Procedures
Successful PVI was achieved in all patients. In the PVI plus CTI block group, CTI block with a bidirectional block was made in all patients. There was no significant difference in procedure time in both groups because most CTI block was performed during the waiting time after completion of PVI (176.8±72.6 minutes in the PVI group vs. 174.2±76.5 minutes in the PVI+CTI block group, p=0.75). Procedural complications occurred; 1 cardiac tamponade (the PVI group), 1 pseudoaneurysm in the femoral puncture site (the PVI group), 2 hematomas in the femoral puncture site (1 in the PVI group, 1 in the PVI+CTI block group).
Outcomes
All patients were followed up for at least 18 months, and the median follow-up was 3.4 years. Rates of the primary endpoint, recurrence of AF or AFL, were not significantly different in the two groups (25.7% in the PVI group vs. 27.3% in the PVI+CTI group, p=0.92). Figure 1A shows the cumulative AF- or AFL-free rate during follow-up after the 3-month blanking period. AFL occurred in 9 (2.4%) patients during follow-up. Rates of the secondary endpoint, recurrence of any AFL, were not significantly different in the two groups (3.3% [6/183] in the PVI group vs. 1.6% [3/183] in the PVI+CTI group, p=0.31). Figure 1B shows the cumulative any AFL-free rate during follow-up after the 3-month blanking period. The recurrence rate of typical AFL was not different between groups (0.5% [1/183] in the PVI group vs. 0.5% [1/183] in the PVI+CTI group, p=0.99). Subgroup analyses were performed. No significant interactions were identified (Figure 2).
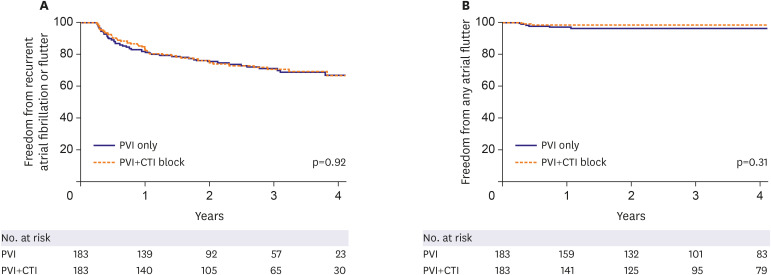 | Figure 1Kaplan-Meier curves for recurrence rates of atrial fibrillation or flutter (A) and any atrial flutter (B).CTI = cavotricuspid isthmus; PVI = pulmonary vein isolation.
|
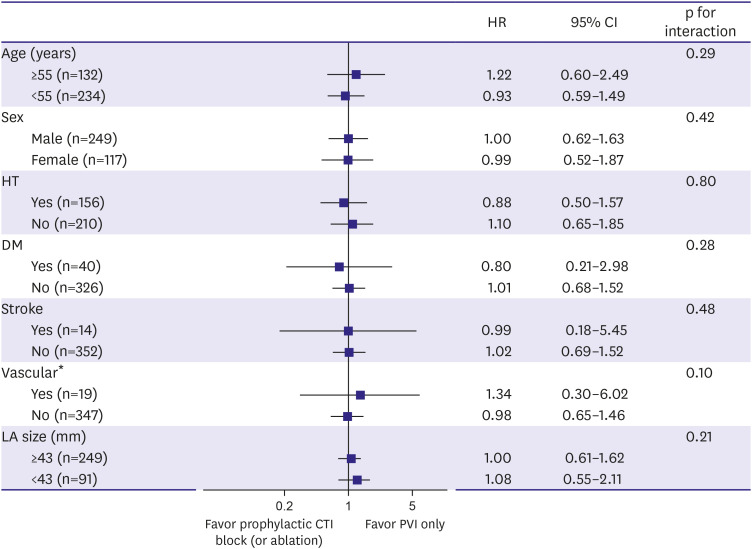 | Figure 2Interactions and hazard ratios for recurrence rates of atrial fibrillation or flutter.CI = confidence interval; CTI = cavotricuspid isthmus; DM = diabetes mellitus; HR = hazard ratio; HT = hypertension; LA = left atrial; PVI = pulmonary vein isolation.
*Vascular disease included myocardial infarction, peripheral artery disease, and aortic plaque.
|
Go to :
DISCUSSION
In this randomized trial, we found no reduction in the rate of recurrent AF or AFL when prophylactic CTI ablation and ablation with PVI were performed in patients with paroxysmal AF. These results, which were observed during a long-term follow-up period (at least 18 months and the median of 3.4 years), were consistent across the primary and all secondary endpoints. Although the negative result like the present study was already reported, the assumptions for the sample size calculation were inappropriate in the previous study.9) Therefore, a larger study should be needed to clarify the effect of prophylactic CTI ablation.
According to the well-defined anatomic substrate and pharmacologic resistance, CTI ablation is an effective and safe first-line treatment for typical AFL.12) For patients undergoing AF ablation, CTI ablation can be easily performed without significant prolongation in procedure time due to performance during the waiting time for the 3D geometry or waiting phase of PVI. Current guidelines recommend that CTI ablation be performed in patients with a history of typical AFL or induced typical AFL at the time of AF ablation (Class I indication).7),13) However, there is no current recommendation in patients with no history of AFL.
A small randomized trial reported that CTI ablation in addition to PVI had no benefit on AF or AFL recurrence at one year.9) Ablation technique, experience, and results have been improved over time; previous high complication rate (cardiac tamponade, 4%), low success rate (recurrence rate of typical AFL in 1 year, 4%; recurrence rate of AF in 1 year, 45%), and heterogenous AF type (paroxysmal, 54%) would not be acceptable in current practice. The previous study was too small and the follow-up period too short to demonstrate the additional benefit of prophylactic CTI ablation.14)
The ablation strategy and outcomes usually differed with the type of AF. Poor outcomes were expected in patients with persistent AF, even though additional ablation was performed. Therefore, we limited our study population to paroxysmal AF, and the same ablation strategy, PVI, was applied in all patients. We found no benefit of prophylactic CTI ablation for AF or AFL recurrence rate. These findings are consistent with data from a previous study by Pontoppidan et al.9) Recurrence rate of AF or AFL in our study seemed to be low, which could be caused by under-detection of the event, the inclusion of paroxysmal AF type and adjunctive anti-arrhythmic drug therapy. In addition, relatively young age, advanced mapping technology, antral ablation, and accumulated experience could be another explanation.15)
The occurrence of typical AFL in the PVI group (0.5%) was much lower than that in the previous study (5%)9) because some patients with intraprocedural documentation of typical AFL were excluded. Most studies where the creation of additional lines in the absence of documented tachycardias did not show any additional effect. The best-known study is the STAR-AF 2 study, and our study was compatible with these findings.16) Performing unnecessary ablation could increase risk without benefit. Although there is no additional risk and time in the PVI+CTI ablation group, the operator should not ablate without evidence. Typical AFL could be induced during the procedure while there was no history of documentation (32/408, 7.8%). It is unclear whether induced typical AFL should be ablated because the patients were excluded from our study. However, considering the prevalence (7.8%), it would be acceptable that a typical AFL induction study should be performed in every AF ablation procedure, and induced typical AFL should be ablated.
Our study has some limitations. First, the use of anti-arrhythmic drugs was at the physician's discretion. Second, all procedure was performed at the tertiary hospitals, so the results were interpreted with caution. Third, only 24-hour Holter was used for monitoring. After 1-year, Holter monitoring was performed every 6 months. Thus, the recurrence rate of AF or AFL could be underestimated.
In this long-term and large study, additional CTI ablation had no benefit for patients with paroxysmal AF but no previous or induced AFL.
Go to :
 XML Download
XML Download