

 PDF
PDF Citation
Citation Print
Print



Introduction
Metastases from other organs to the thyroid are extremely rare, with cases mainly observed in autopsies.1) At autopsy, the breast and lung are the most common primary cancer sites that metastasize to the thyroid.2,3)
Anaplastic thyroid cancer, the most aggressive form of thyroid malignancies, exhibits a broad spectrum of morphological features and can be difficult to diagnose due to a high degree of reverse differentiation. Unlike papillary and follicular carcinomas, which have been well differentiated, anaplastic thyroid cancer shows rapid growth and a high local recurrence rate, with a 5-year survival rate of 1.0-7.1%. The average survival time is reported to be 4 to 12 months.4-6)
This report presents a case of thyroid anaplastic carcinoma diagnosed though fine needle aspiration (FNA) in a 76-year-old patient previously diagnosed with non-small cell lung carcinoma (NSCLC).
Case Report
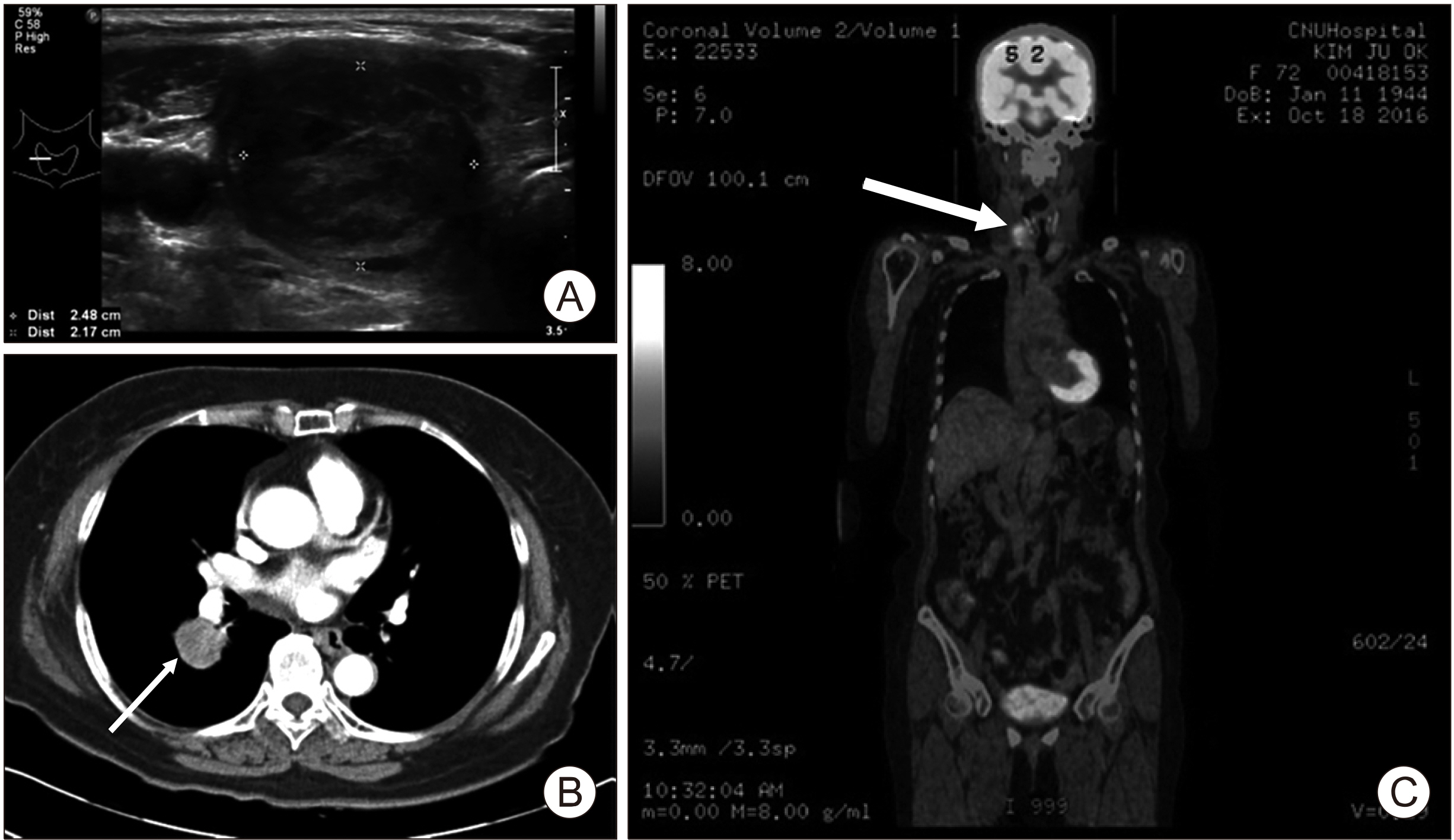
A 76-year-old woman with no respiratory symptoms or smoking history was admitted to the Department of Respiratory Medicine with a right lower lung mass found in chest PA detected on physical examination. Based on bronchoscopy performed for the evaluation of the lung mass, lung cancer was suspected and computed tomography (CT)-guided percutaneous core needle biopsy (PCNB) was performed. Positron emission tomography (PET)-CT imaging was performed before surgery to evaluate another metastasis (Fig. 1). The patient subsequently underwent a right lower lobectomy in the Department of Cardiothoracic Surgery, with the results of the postoperative histological examination indicating adenocarcinoma exhibiting acinar (40%), papillary (30%), and solid (30%) patterns (Fig. 2A).
In addition to the management of NSCLC, the patient was followed by thyroid ultrasound of two benign thyroid nodules since 2016. During the postoperative follow-up after thoracic surgery, 4-years later, the patient was referred to Department of General Surgery for elevated carcinoembryonic antigen (CEA) and increased size of the right thyroid nodule. FNA of the thyroid nodule indicated anaplastic carcinoma. Total thyroidectomy with central neck dissection was performed. The results of the histopathological examination indicated metastatic adenocarcinoma of lung origin with poor differentiation, which is clinically a very rare occurrence (Fig. 2B). Blood tests performed before surgery showed the following findings: tumor marker CEA 39.59 ng/mL, calcitonin 83 pg/mL, free thyroxine 1.14 μg/dL, free triiodothyronine 1.38 μg/dL, thyroid-stimulating hormone (TSH) 0.98 μIU/mL, anti-thyroglobulin antibodies 9.56 U/mL, parathyroid hormone 36.81 ng/L, and thyroglobulin 31.09 µg/L. No distinguishing biochemical features generally observed in anaplastic thyroid cancer were detected, such as the lack of thyroglobulin production, the inability to carry iodine, or the lack of TSH receptors.
The patient was subsequently seen in the Department of Respiratory Medicine for treatment of the cancer of pulmonary origin. The thyroid tissue was tested for epidermal growth factor receptor (EGFR) mutations, anaplastic lymphoma kinase (ALK), and programmed death-ligand 1 (PD-L1) in the primary lung tissue (Table 1). PET-CT imaging performed after thyroid surgery detected multiple lymph node metastases, with hypermetabolism in right level IIB, III, IV, and VI border zone lymph nodes. However, no significant lymphadenopathy was observed on neck CT performed before thyroid surgery, as mentioned earlier. Brain MRI showed no metastatic lesions or specific findings, and chest CT detected no abnormalities in either of the neck lymph nodes.
Based on the mutations detected through additional genetic testing performed following total thyroidectomy, we initiated treatment for NSCLC recurrence using gefitnib (an EGFR inhibitor) based on Exon21 L858R mutation.
Discussion
Despite the rich vascular supply to the gland, metastases to the thyroid are extremely rare,7) accounting for less than 4% of all malignant thyroid tumors.1,8)
Anaplastic thyroid cancer is a highly malignant disease. Due to its aggressive nature (which distinguishes it from other thyroid cancers), it is unlikely to be misdiagnosed as another disease. A cancer that has metastasized to the thyroid gland may be difficult to distinguish histologically from an undifferentiated cancer. This can be the case in situations in which the cancer transferred to the neck exhibits dedifferentiation, as in the reported case.
According to the National Comprehensive Cancer Network (NCCN) guidelines, lung cancer is classified into “small cell lung cancer” (15%) and NSCLC (85%) according to the histological features. NSCLC is further subclassified into adenocarcinoma (40% of NSCLC cases), squamous cell carcinoma (30%), or large cell carcinoma. Differentiation between squamous cells and the non-squamous epithelium has important connotations for the treatment of NSCLC. In many cases of non-squamous cell carcinoma, including adenocarcinoma, an induced mutation (driver mutation) is observed in EGFR, ALK, ROS1, or BRAF genes. It is important to test for these mutations, particularly EGFR and ALK, in all cases. When such mutations are found, drug treatment appropriate for the specific mutation should be selected. If mutations are not present, the PD-L1 test should be performed to determine whether single agent immunotherapy, combination immunotherapy, or a combination of immunotherapy with chemotherapy should be implemented, depending on the degree of expression.
Adenocarcinoma is the most common histological type found in patients with lung cancer, which has metastasized to the thyroid, with histological types associated with different life expectancies. While mutations in the EGFR and EML4-ALK genes are associated with thyroid metastases, the exact mechanism underlying this interaction has not yet been elucidated.
Diagnosis
Thyroid cancers can be qualitatively diagnosed through FNA and immunohistochemistry. FNA is a fast, minimally invasive, and affordable technique that can be used to differentiate between metastatic lung cancer and thyroid cancer. Patients with thyroid nodules should consider an FNA to rule out other disorders. However, in some cases, FNA alone is not sufficient, and it may be difficult to distinguish between undifferentiated thyroid cancer and metastatic malignant tumor.3,9,10)
Immunohistochemistry exhibits a high accuracy in diagnosing thyroid cancer, with the reported false negative rate of less than 1% and the false positive rate of approximately 2-3%.11,12) Additionally, immunohistochemistry can be used to distinguish between metastases and primary thyroid tumors.13) On immunohistochemistry examination, undifferentiated thyroid cancer is generally negative for thyroid globulin and calcitonin. Approximately half and one-third of cases are positive for pan-keratin and epithelial membrane antigen, respectively, while vimentin is found in 90% of cases. Thyroid transcription factor-1 is present in 0-50% of the cases. These markers can distinguish anaplastic thyroid cancer from other diseases with similar presentation (Table 2, Fig. 3).
Among findings of imaging modalities such as PET-CT, detection of a “cold” nodule on thyroid scan, a hyperechoic mass on ultrasound, and calcification of the thyroid parenchyma and nodules can be seen as features of thyroid metastases.12,14)
Biologically, thyroid hormone balance is unaffected by metastatic thyroid nodules.15) The thyroid hormone levels were found to be normal in the presented case.
Surgical Treatment
In the case of metastatic cancer of the thyroid, surgery is performed to address the potential morbidity related to tumor recurrence in the neck. However, the prognosis remains poor in most cases, and the surgery does not contribute to prolonging the life of patients.16,17)
For metastatic cancer, systemic treatment with chemotherapy or targeted therapy is the standard treatment. Radioiodine treatment is not indicated for thyroid metastases. A case report describing a patient with thyroid metastases from lung cancer with an EGFR mutation reported a marked response of the thyroid and lung masses after the patient was treated with erlotinib.18) Radiation therapy was described as an alternative approach for partial symptom relief in thyroid cancer.19)
We present a rare case of a patient with metastases to the thyroid gland following diagnosis of NSCLC. In this case, thyroidectomy did not appear to affect the patient’s disease progression, and neck lymph node metastases were detected immediately after thyroid surgery. Therefore, active systemic therapy for primary cancer is expected to affect the disease progression in patients.
Metastasis from the lungs to the thyroid is rare and may be confused with primary thyroid cancer if it does not clearly display the clinical features described above, making it difficult to accurately diagnose. Therefore, a close follow-up and diagnostic examination of thyroid nodules are required.


 XML Download
XML Download