

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Diabetes mellitus (DM) has become increasingly more prevalent over the past several decades, with an estimated outbreak over 366 million by 2030 [1]. The long-term DM complications, induced by prolonged hyperglycemia, have been the major causes of premature mortality and morbidity [234]. Therefore, tight glycemic control may reduce the risk of progression to complications over time. Hypoglycemia is frequently accompanied by tight glycemic control with intensive antidiabetic therapy. However, several studies failed to investigate the conclusion that strict glycemic control targeting a glycosylated hemoglobin (HbA1c) level of <6.5% reduced the incidence of complications [567]. Additionally, hypoglycemia and all-cause mortality rates reportedly increased in the intensively controlled groups of some trials [678]. While hyperglycemia is the main cause of microvascular and macrovascular complications, hypoglycemia can cause a series of sequelae that can alter the patient's cardiovascular risk profile and increase mortality. Particularly, hypoglycemia in the intensive care unit (ICU) increases the risk of mortality, seizures, and coma; thus, careful monitoring for tight glycemic control is crucial [9]. However, studies performed in ICU patients may show overestimated results compared with those of analysis on general glycemic control. Most patients experiencing hypoglycemia encounter the condition in real life, not in the ICU. Furthermore, hypoglycemia outcomes in patients hospitalized only for glycemic control is less known.
Therefore, this study analyzed risk factors of hypoglycemia among patients who experienced and those who did not during hospitalization and the effect of hypoglycemia on clinical outcomes.
METHODS
Study design and selection of participants
This was a retrospective study of electronic medical records (EMRs) of patients admitted for only glycemic control at the Department of Endocrinology and Metabolism of Seoul St. Mary's Hospital from January 2009 to July 2018. Patients diagnosed with DM and treated with oral hypoglycemic agents (OHAs) or insulins were selected. Patients with DM admitted for other reasons, such as frequent hypoglycemia due to DM-complications or gastrointestinal symptoms, were excluded. All OHAs and insulin orders were documented and reviewed during hospitalization. No other exclusion criteria were considered except for the cause of hospitalization. DM was defined using the International Classification of Diseases-10th Revision (ICD-10), as follows: E10 (type 1 DM [T1DM]), E11-E14 (type 2 DM [T2DM]), and O24 (DM in pregnancy).
Interventions
Patients admitted for glycemic control underwent blood glucose measurement seven times a day: fasting glucose after overnight fasting (6:00 to 6:30 AM), preprandial glucose (before a meal), and postprandial glucose after 2 hours following meal initiation (10:00 to 10:30 AM, 2:30 to 3:00 PM, and 8:00 to 8:30 PM); additional glucose measurements were performed when patients felt hypoglycemic or at 3:00 AM when patients had a fasting glucose level <70 mg/dL. The hypoglycemia during hospitalization (HYPO group) comprised patients experiencing at least one hypoglycemia episode during hospitalization, whereas the control group comprised patients treated without experiencing hypoglycemia during hospitalization. Hypoglycemia was defined as blood glucose level <70 mg/dL based on the value checked after admission [10]. After admission, insulin dose was increased or decreased appropriately according to the guidelines [11].
Outcome measures
On admission, data on basic characteristics, including age, sex, height, weight, and body mass index (BMI), were extracted. Blood chemistry results were reviewed based on EMRs. HbA1c, C-peptide, insulin, blood urea nitrogen (BUN), creatinine, glomerular filtration rate (GFR), sodium, potassium, aspartate aminotransferase (AST), alanine aminotransferase (ALT), creatine phosphokinase, lactate dehydrogenase, amylase, lipase, erythrocyte sedimentation rate (ESR), high-sensitivity C-reactive protein (hsCRP), alkaline phosphatase, gamma-glutamyl transpeptidase (γ-GTP), total cholesterol (TC), triglycerides, high density lipoprotein cholesterol (HDL-C), low density lipoprotein cholesterol (LDL-C), and osmolality values were evaluated. All measurements were performed with an automated blood chemistry analyzer (Hitachi 747; Hitachi, Tokyo, Japan). HbA1c was measured by high-performance liquid chromatography using Diabetes Control and Complications Trial-aligned methods (Tosoh-G8; Tosoh, Tokyo, Japan). Homeostatic model assessment of insulin resistance (HOMA-IR) and homeostatic model assessment of beta-cell function (HOMA-β) as insulin resistance markers were calculated as follows [12]:
HOMA-IR=[fasting insulin (IU/mL)×fasting plasma glucose (mmol/L)]/22.5
HOMA-β=[20×fasting plasma insulin (IU/mL)]/[fasting plasma glucose (mmol/L)−3.5]
We extracted data on all OHAs and insulin types that were prescribed during the patient's hospitalization. Insulin was categorized into basal insulin (glargine, detemir, and degludec), bolus insulin (aspart, lispro, and glulisine), and premixed insulin. OHAs were divided into metformin, dipeptidyl peptidase-4 inhibitors (DPP4i), and sodium-glucose cotransporter-2 inhibitors (SGLT2i), while treatment modalities were classified according to the combination of insulin and OHAs. The ICD-10 was used to confirm the presence of current comorbidities, as follows: I10-I15 (hypertensive disease); I20 (angina pectoris); I21 (acute myocardial infarction [AMI]); I20-I25 (ischemic heart disease [IHD]); I60-I69 (cerebrovascular disease [CVD]); C (cancer); I50, I11.0, I13.0, and I24.8 (heart failure); and I12, I13, and N17-N19 (renal failure). The initial diagnosis date of these diagnoses was examined to determine whether the diagnosis was a current coexisting disease or a disease occurring after discharge.
Direct chart review and data quality management
A direct chart review was conducted to determine if patients were hospitalized for glycemic control. We excluded patients admitted for perioperative glycemic control and admitted due to other diseases but had high blood glucose levels. To confirm the extracted data, one researcher modified the data through direct chart review. The modified data were stored separately and processed using the same protocol.
Privacy protection
All identifiable information, including patient's name and social security number were made anonymous. The patient's hospital registration number was assigned a temporary number by a responsible investigator, and after the analysis, the registration number was deleted. The comparison of the hospital registration number with the temporary number was accessible only to the responsible investigator. If a chart review was required after statistical processing, the responsible investigator could access the hospital information. All data were stored in an encrypted computer in the form of encrypted files, which were accessible only to the responsible investigator. This study used EMRs of patients whose treatments were terminated, and thus, there was no physical or mental risk to the patients. Therefore, informed consent was not required. This study was approved by the Clinical Research Ethics Committee of the Catholic University of Korea (IRB no. KC18RNSI0379).
Primary data analysis
Baseline variables were presented as means and standard deviations or medians and interquartile ranges for continuous variables based on normality, and numbers and percentages for categorical variables. Hypoglycemia status was compared using the independent t-test or Wilcoxon rank-sum test for continuous variables and the chi-square or exact test for categorical variables. Differences in incidence ratio were determined by survival analysis using the log-rank test to compare hypoglycemic admission status and various disease entities. All statistical analyses were performed using SAS version 9.4 (SAS Institute, Cary, NC, USA). A P value of <0.05 was considered statistically significant.
RESULTS
In total, 3,862 patients were admitted for glycemic control between January 2009 and July 2018 at our department. Among them, 831 patients were hospitalized due to reasons besides glycemic control. Finally, 3,031 patients were included.
Baseline characteristics of study subjects
The mean age was 59.3±16.5 years (range, 42.8 to 75.8 years), and 50.9% (1,543/3,031) were female. The mean BMI was 24.9±4.4 kg/m2 (range, 20.5 to 29.3 kg/m2). Of 3,031 patients, 2,937 (96.9%) had diagnostic codes for T2DM, 91 (3.0%) for T1DM, and three (0.1%) for DM in pregnancy. Moreover, 50.7% of patients were treated with multiple insulin injections using basal and bolus insulin, while 8.0% (243/3,031) were prescribed with premixed insulin. The mean length of hospital stay was 8.0±6.5 days (Table 1).
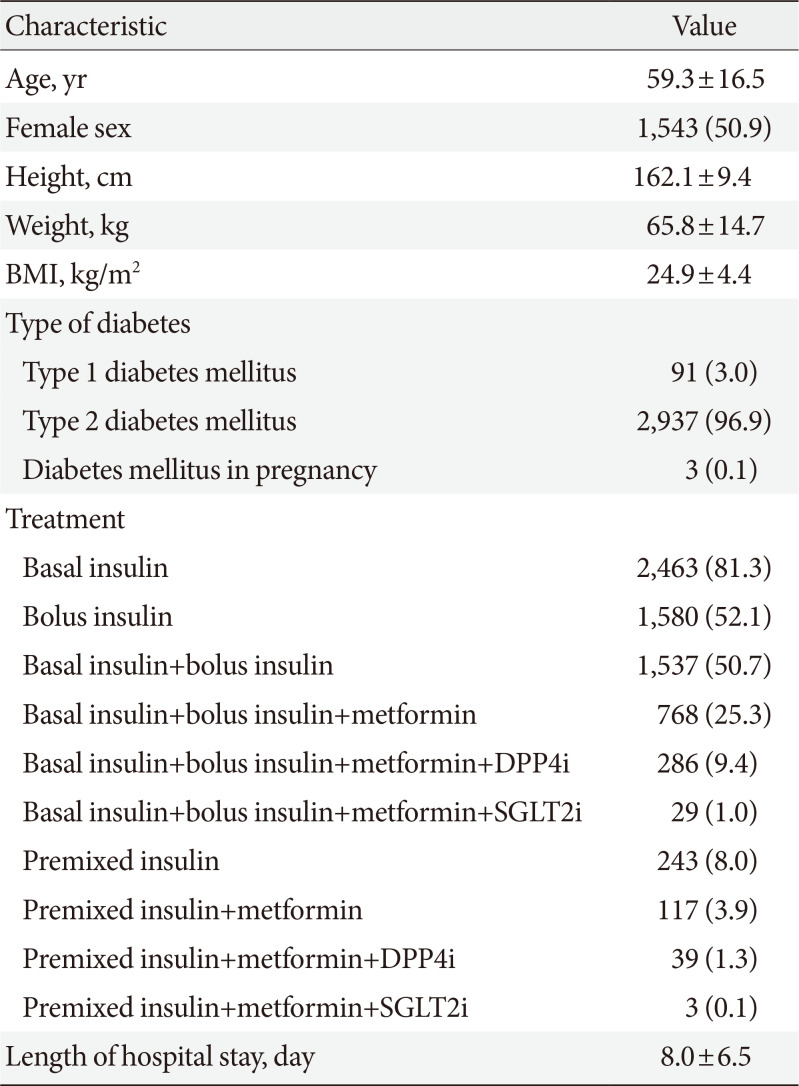
Table 1
Baseline characteristics of patients (n=3,031)
![]()
Baseline characteristics according to hypoglycemia occurrence during hospitalization
Table 2 summarizes the demographic characteristics between the HYPO and control groups. Of 3,031 patients, 12.5% (379) experienced at least one episode of HYPO group, whereas 87.5% (2,652) were treated without experiencing hypoglycemia during the stay (control group). The HYPO group had significantly older age (61.0±16.8 years vs. 59.1±16.5 years, P=0.035), more females (60.4% vs. 49.6%, P<0.001), and significantly lower BMI (23.5±4.2 kg/m2 vs. 25.1±4.4 kg/m2, P<0.001). T1DM was more prevalent in the HYPO group (6.1% vs. 2.6%, P<0.001).
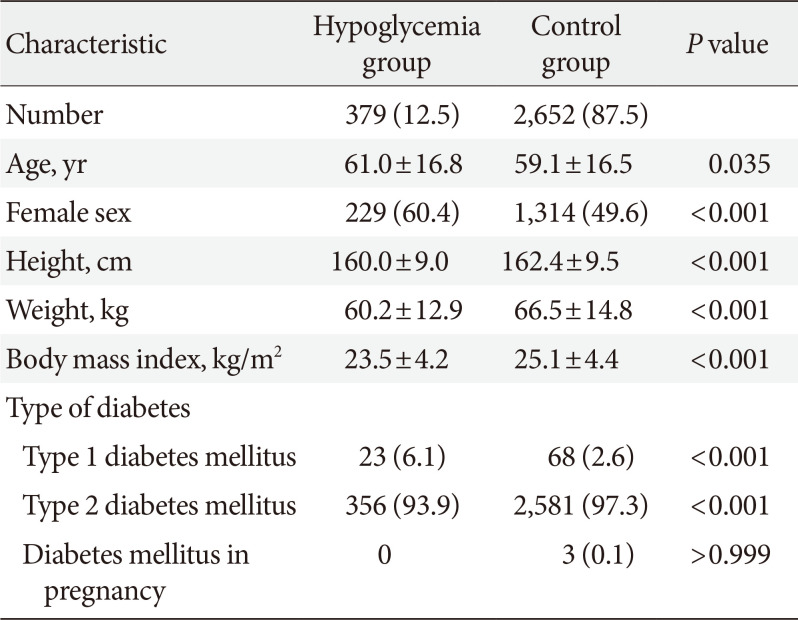
Table 2
Demographic characteristics of the hypoglycemia group and control group
![]()
Treatment pattern in the HYPO and control groups
Regarding treatment pattern during hospital stay (Table 3), there were no significant differences in basal insulin (82.3% vs. 81.1%, P=0.571) and bolus insulin (53.8% vs. 51.9%, P=0.479) between both groups. There was also no significant difference in treatment with basal insulin+bolus insulin between both groups (53.0% vs. 50.4%, P=0.333). Use of treatment with a basal insulin+bolus insulin+metformin combination was significantly less common in the HYPO group (21.1% vs. 25.9%, P=0.043). Furthermore, there was no significant difference between both groups regarding treatment with basal insulin+bolus insulin+metformin combined with DPP4i (9.5% vs. 9.4%, P=0.964) and SGLT2i (0.3% vs. 1.1%, P=0.251). However, premixed insulin was significantly more used in the HYPO group (10.8% vs. 7.2%, P=0.012). Use of the regimen consisting of a premixed insulin and metformin combination was significantly more commonly used in the HYPO group (6.3% vs. 3.5%, P=0.008). We analyzed the association between hypoglycemia and treatment regimen using logistic regression analysis. The risk of hypoglycemia differed according to treatment regimen. Odds ratio (OR) was obtained by referring to OR of control group as 1.0. Hypoglycemia was prominent in those who used premixed insulin (OR, 1.57; 95% confidence interval [CI], 1.10 to 2.24; P=0.013) and premixed insulin with metformin (OR, 1.85; 95% CI, 1.17 to 2.95; P=0.009) (Supplementary Table 1).
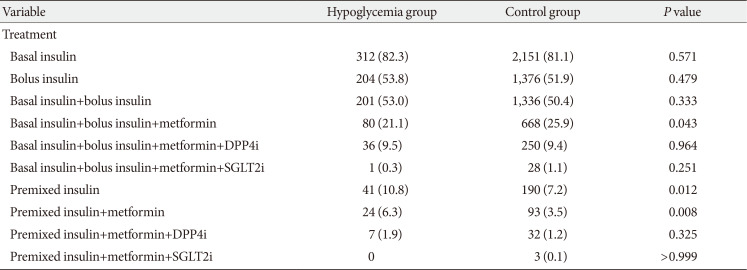
Table 3
Treatment pattern between the hypoglycemia group and control group
![]()
Laboratory findings in the HYPO group
Those in the HYPO group had a lower HbA1c level than the control group, but there was no significant difference (10.0%±2.3% vs. 10.1%±2.3%, P=0.410) (Supplementary Table 2). C-peptide was significantly lower in the HYPO group (0.9 ng/mL [0.3 to 2.0] vs. 1.7 ng/mL [0.9 to 2.7], P<0.001). There were no significant differences in insulin (20 µIU/mL [11 to 42] vs. 18 µIU/mL [12 to 34], P=0.323), HOMA-IR (7 [3 to 19] vs. 8 [4 to 16], P=0.492), and HOMA-β (63 [21 to 205] vs. 61 [28 to 136], P=0.768). The mean AST (20 U/L [16 to 26] vs. 21 U/L [17 to 28], P=0.049), ALT (18 U/L [13 to 27] vs. 21 U/L [15 to 32], P<0.001), lipase (28 U/L [19 to 48] vs. 35 U/L [21 to 55], P=0.005), and γ-GTP (23 mg/dL [16 to 50] vs. 29 mg/dL [19 to 54], P<0.001) were significantly lower in the HYPO group than in the control group, but with no clinically meaningful differences. There were no significant differences in BUN and creatinine. However, the HYPO group showed significantly lower GFR than the control group (29.3±12.3 mL/min/1.73 m2 vs. 32.3±12.6 mL/min/1.73 m2, P<0.001). There were significantly more patients with a GFR of <30 mL/min/1.73 m2 in the HYPO group than in the control group (P=0.002) (Supplementary Table 3). In addition, there were no significant differences in ESR (19 mm/hr [10 to 38] vs. 17 mm/hr [9 to 33], P=0.077) and hsCRP (0.1 mg/dL [0.1 to 0.5] vs. 0.1 mg/dL [0.1 to 0.4], P=0.052). For lipid profiles, the HYPO group demonstrated significantly lower TC (156±51 mg/dL vs. 162±50 mg/dL, P=0.047), triglycerides (104 mg/dL [70 to 152] vs. 125 mg/dL [88 to 187], P<0.001), and LDL-C (85±39 mg/dL vs. 91±37 mg/dL, P=0.015) and significantly higher HDL-C (44±16 mg/dL vs. 40±12 mg/dL, P=0.001). Sodium (136±5 mEq/L vs. 137±5 mEq/L, P=0.001) and potassium (4.1 mEq/L [3.6 to 4.4] vs. 4.2 mEq/L [3.9 to 4.5], P<0.001) levels were significantly lower in the HYPO group; however, there was no clinically meaningful difference.
Comparison of comorbidities
For heart failure, there was no significant difference between both groups (5.5% vs. 5.6%, P=0.738). Hypertensive disease (41.2% vs. 38.7%, P=0.363), angina (13.5% vs. 13.5%, P=0.966), AMI (5.0% vs. 3.4%, P=0.124), IHD (20.8% vs. 18.6%, P=0.294), CVD (11.9% vs. 10.8%, P=0.525), and renal failure (9.2% vs. 7.3%, P=0.177) had higher prevalence in the HYPO group than in the control group; however, these results were not significant (Table 4).
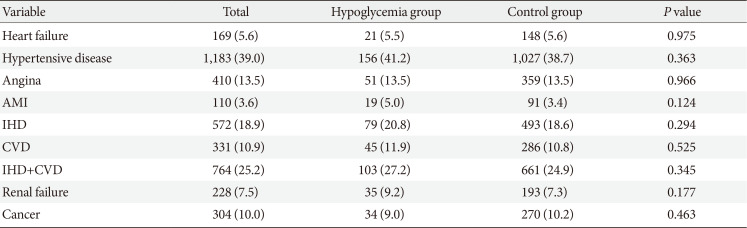
Table 4
Comparison of comorbidities between the hypoglycemia group and control group
![]()
Comparison of length of hospital stay and HbA1c after discharge
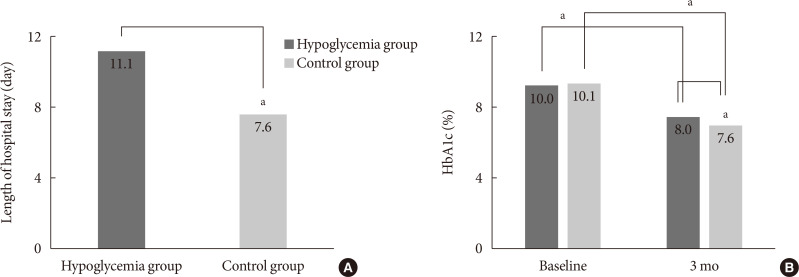
The mean length of hospital stay was significantly longer in the HYPO group than in the control group (11.1±13.5 days vs. 7.6±4.6 days, P<0.001) (Fig. 1A). Significant improvement in HbA1c after discharge was achieved in both the HYPO (from 10.0% to 8.0%, P<0.01) and control group (from 10.1% to 7.6%, P<0.01). However, the HYPO group showed less improvement in HbA1c than the control group (−2.0%±0.2% vs. −2.5%±0.1%, P=0.003) (Fig. 1B).
Two-year follow-up morbidity and hypoglycemia
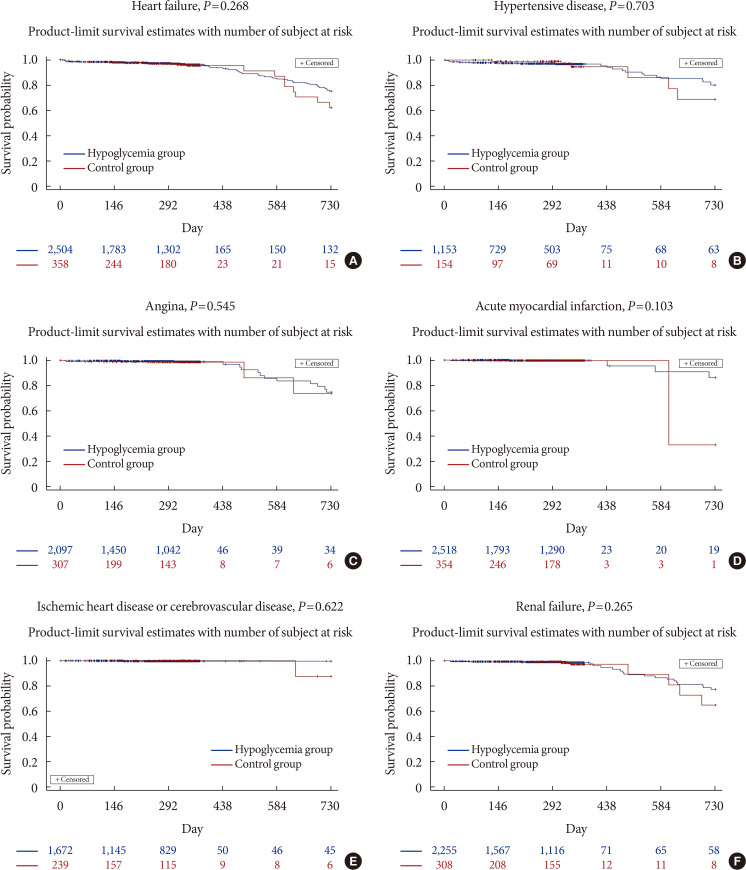
Analyses of 2-year follow-up morbidity were performed (Fig. 2). The HYPO group showed higher incidence of heart failure (P=0.268) (Fig. 2A), hypertensive disease (P=0.703) (Fig. 2B), angina (P=0.545) (Fig. 2C), AMI (P=0.103) (Fig. 2D), IHD or CVD (P=0.622) (Fig. 2E), and renal failure (P=0.265) (Fig. 2F) than the control group; however, there were no significant differences.
DISCUSSION
Hypoglycemia is a crucial complication of intensive glycemic control. Severe hypoglycemia is associated with increased risk of microvascular and macrovascular complications, including cardiovascular disease and non-cardiovascular disease [56]. Moreover, hypoglycemia induces poor outcomes in hospitalized patients [13]. Inpatient hypoglycemia is correlated with longer length of hospital stay and increased mortality [1415]. We revealed that an experience of hypoglycemia during hospitalization affected the length of hospital stay and poorly controlled the HbA1c level.
Hypoglycemia acts as a barrier to insulin therapy for glycemic control. Basal insulin and premixed insulin reduced HbA1c level by a similar amount, and hypoglycemia risk was higher with premixed insulin [161718]. Premixed insulin is usually preferred to reduce the inconvenience of multiple injections compared with basal-bolus insulin injection. Premixed insulin may be beneficial in controlling postprandial glucose, but it can be applied mainly to patients with constant, regular meals and meal volume [19202122]. When variations in blood glucose control arise due to irregular meals or when food intake is impossible, premixed insulin often induces hypoglycemia [23]. In our study, hospitalized patients were provided with regular meals according to adjusted calories, and insulin dose was determined according to protocol. However, the hypoglycemia rate was high in the case of premixed insulin treatment in this study. It is also important to consider the possibility of differences between individual characteristics. These are the reasons why personalized treatment is necessary. In fact, in this study, the frequency of hypoglycemia was higher in older and leaner females. Another reason could be insufficient medical management for increasing insulin by the clinician. Clinicians have less experience with premixed insulin than with basal or bolus insulin [242526].
Older age is an important factor of hypoglycemia. Premixed insulin causes hypoglycemia more frequently in the elderly [27]. In our results, in-hospital hypoglycemia was more common among older and female patients with lower BMI. Therefore, insulin selection is very crucial in reducing hypoglycemia among older females with low BMI.
In our study, glucose and C-peptide levels were significantly lower in the HYPO group, with no differences in HbA1c, HOMA-IR, and HOMA-β. Our results of lower C-peptide level and hypoglycemia are consistent with those of some studies on T1DM [2829]. Meanwhile, lower C-peptide level and hypoglycemia in T2DM are less commonly studied. C-peptide is an amino acid that is a cleaved form of proinsulin [30]. Although previous studies have investigated that C-peptide has no glucose-lowering effect, C-peptide induces insulin action at lower levels of the hormone and inhibits insulin action at higher levels [31]. Hence, C-peptide might predict hypoglycemia. This study also presented that GFR could be a predictor of hypoglycemic events. With kidney dysfunction, OHAs and insulin can accumulate and increase the body's susceptibility to hypoglycemia. Moreover, kidney disease could impair glucose counter-regulation and reduce renal gluconeogenesis [32].
In the analysis of short-term follow-up after discharge, patients with hypoglycemia showed 146% longer hospital stay than those without hypoglycemia. This was consistent with the findings of other studies [3334]. After hospitalization, HbA1c level was lower in patients without hypoglycemia than in those with hypoglycemia. Glycemic control analyzed based on differences in HbA1c levels was better among patients without hypoglycemia than among those with hypoglycemia. The effect of glycemic control on admission was apparent in both groups. If hypoglycemia affected the course of treatments for hypoglycemia itself, the delay would have to prolong the length of hospital stay. Hypoglycemia is correlated with cardiovascular mortality in insulin-treated patients [35]. Likewise, in our study, patients in the HYPO group showed higher incidence for hypertensive disease, AMI, IHD, CVD, and stage 4 kidney disease, reflecting a greater tendency for cardiovascular disease. Since our study period (2 years) was short for analyzing outcomes, little significant difference was found between patients with hypoglycemia and those without hypoglycemia. Moreover, this study did not focus on ICU patients but focused on patients hospitalized only for glycemic control. Thus, further research involving a large number of patients and a longer follow-up period will be needed.
This study has some limitations. As this study was based on retrospective data obtained from only one hospital, we could not confirm a causal relationship between hypoglycemia and various risk factors or occurrence of cardiovascular disease. Furthermore, the diagnostic data were based on ICD-10 codes; therefore, misclassification may have occurred, including failure to classify other diagnoses unrelated to DM due to the research focus on hypoglycemia. Although, it is possible that alteration of the post-discharge treatment regimen affected HbA1c levels, the treatment regimen used after discharge was not analyzed in the current study because of limitations of the data.
The greatest advantage of this EMR-based retrospective study is that it used real-world evidence (RWE) based on real-world data obtained from real practice. This study was conducted in patients experiencing hypoglycemia rather than in ICU patients only. The results of randomized controlled trials and RWE differ significantly when applied in actual practice, including when assessing the actual effects of treatment [36]. RWE can be used to judge the current treatment situation because it reflects the actual treatment field [37]. Although our results showed a tendency to agree with the results of most previous studies, it is worth noting that premixed insulin-induced hypoglycemia occurred more often in leaner and older females and was associated with poor outcomes in terms of length of hospital stay and glycemic control. Therefore, clinicians should focus on preventing hypoglycemia during hospitalization when prescribing premixed insulin.
In summary, the frequency of hypoglycemia during hospitalization was higher among older and leaner females. Hypoglycemia also correlated with increased length of hospital stay and poorly controlled hyperglycemia. This study was based on RWE regarding hypoglycemia, and therefore the findings could be applicable to patients with DM in real life. While there was lack of causative factors for increased cardiovascular morbidity in our data, our findings support the trend of increased cardiovascular morbidity among patients who experience hypoglycemia. However, further research with a longer study period and larger sample size is required to identify whether hypoglycemia among inpatients is associated with adverse outcomes after discharge.
 XML Download
XML Download