

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Single-visit apexification has been used for the endodontic treatment of teeth with necrotic pulps and open apices [12]. Single one-visit apexification has taken precedence over the previous technique that used calcium hydroxide, after the introduction of calcium silicate cements, including ProRoot mineral trioxide aggregate (MTA) (Dentsply-Sirona, Ballaigues, Switzerland) [2]. Witherspoon et al. [2] reported that over 90% of teeth treated with MTA demonstrated healing. Although pulp regeneration therapy has become an increasingly valuable and standard protocol in current endodontic practice [3456], apexification has been reported as a successful treatment option [7]. Alobaid et al. [7] reported a favorable result in their retrospective cohort study, with retention of 100% of teeth in recalled cases, following apexification. There have been several case reports and clinical studies related to MTA apexification or revascularization [8910]; however, direct observation of extracted human teeth after apexification using an MTA barrier has been rarely reported. Several histological studies on extracted human teeth after pulp regenerative therapy have been conducted [111213]. Herein, we report a case of an extracted lower premolar that was endodontically treated 2.5 years ago using apexification with MTA barrier and extracted recently for orthodontic treatment.
Go to : 
CASE REPORT
Endodontic treatment of an infected immature premolar
A 12-year old boy was referred to our institution for the evaluation and treatment of the right mandibular premolar (tooth #45) (Figure 1A and 1E). He had experienced swelling and pain on the gingiva and mucosa of tooth #45 several days before the visit. A sinus tract with purulent discharge was observed and there was no response to cold and electric pulp testing with tooth #45. The tubercle of the dens evaginatus tooth had fractured, with pulp exposure. Tooth #45 was diagnosed with pulp necrosis and an asymptomatic apical abscess due to dens evaginatus. Regenerative pulp treatment was planned initially, and the access cavity was prepared under isolation. During the first visit, copious irrigation was performed using 2.5% sodium hypochlorite (NaOCl), saline, and 17% ethylenediaminetetraacetic acid (EDTA) solution, with a 27-G needle with a rubber stopper, up to 1 mm short of the tentative length of root apex, followed by an intracanal dressing with a calcium hydroxide paste (Calcipex II, Nippon Shika Yakujin Co., Simonoseki, Japan). At the second visit after 3 weeks, the sinus tract had disappeared and the tooth was asymptomatic. The tooth was isolated and irrigated copiously with 2.5% NaOCl and 17% EDTA, following which bleeding was initiated using a curved K-type file (Dentsply-Sirona), without local anesthesia. However, the bleeding induced was insufficient and the bleeding point was detected 16 mm from the buccal cusp. Consequently, we decided to perform apexification using ProRoot MTA (Dentsply-Sirona). The cement was mixed with water according to the manufacturer's instructions and applied to the bleeding point as a 4-mm thick layer. After confirming that the MTA filling was 4–5 mm thick and without any defects, a 3-mm gutta-percha filling, and resin core build-up were performed using Tetric N-Ceram (Ivoclar-Vivadent, Schaan, Liechtenstein) and Clearfil SE bond (Kuraray Dental, New York, NY, USA) (Figure 1B). The patient was asymptomatic and root growth was observed at the 6-months recall (Figure 1C). The patient was asymptomatic for 1.5 years (Figure 1D).
 | Figure 1Series of periapical radiographs taken during the treatment of tooth #45. (A) A preoperative periapical radiograph showing an immature root with periapical radiolucency with tooth #45. A gutta-percha cone was used to trace the periapical lesion to tooth #45. (B) A postoperative periapical radiograph showing apexification with tooth #45. (C) A periapical radiograph taken 6 months after the treatment demonstrating the resolution of the previous periapical radiolucency. (D) A periapical radiograph taken 1.5 years after the treatment showing the formation of the root apex. (E) A preoperative panoramic view. (F) A panoramic view taken 2.5 years after the root canal treatment with tooth #45.op, operative.
|
Micro-computed tomography (micro-CT) observation of the extracted premolar
This tooth and the other three second premolars were to be extracted for orthodontic treatment, 2.5 years after the endodontic treatment (Figure 1F). After obtaining the patient's written consent form, the extracted teeth (tooth #45 and its contralateral tooth, tooth #35) were scanned using micro-CT (SkyScan1173, Bruker-CT, Kontich, Belgium) to observe the root shape and canal anatomy (Figure 2).

Micro-CT imaging revealed irregular root growth with tooth #45, after the apexification procedure. The outline of the root shape of tooth #45 was different from its contralateral tooth. The lengths of both premolars were similar. Dentinal bridge formation was not observed to be in direct contact with the MTA filling. The newly formed root portion seemed calcified without an obvious canal space (Figure 3).
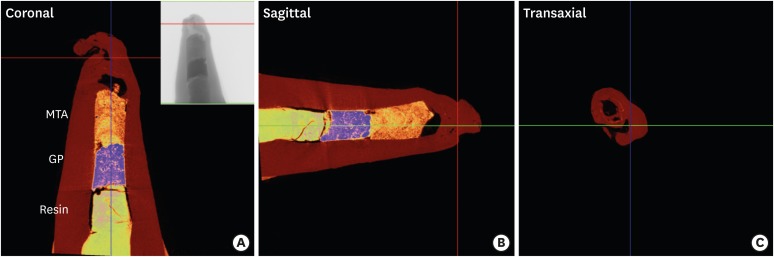 | Figure 3Representative colored images of tooth #45 obtained by micro-computed tomography (micro-CT). (A) A coronal image of micro-CT of tooth #45 showing composite resin, gutta-percha (GP), and mineral trioxide aggregate (MTA) filling in the canal. An irregularly shaped root tip was observed. (B) A sagittal image of tooth #45. (C) A transaxial view of tooth #45.
|
Go to :
DISCUSSION
This case demonstrated an increase in the root length, although the results of earlier studies have been controversial. There was no root length increase in the teeth treated by MTA apexification in some studies [1415]. However, Alobaid et al. [7] demonstrated that the apexification group also showed an increase in root length and width. We speculated that root growth occurred in this case, due to some leftover vital tissue at the apical portion, since we tried to induce bleeding before MTA apexification.
As discussed previously, a pulp regenerative therapy would have been a better choice in this case. As described in the case report section, the bleeding induced up to coronal root was insufficient. Moreover, there was concern regarding irritating the mental foramen, which appeared close on radiographs, if the K-file was extruded further beyond the apex. Another concern was the lack of sufficient bleeding after manipulation with the K-file. During the first visit, calcium hydroxide paste was applied, which could have dissolved some vital tissue around the root apex. Yassen et al. [16] demonstrated superficial collagen degradation in the radicular dentin, if calcium hydroxide was used as an intracanal medicament. Some studies [1718] advocated the usage of triple antibiotic paste, although the best intracanal medicament is still controversial [316].
Hard tissue formation around the MTA filling was an interesting finding of micro-CT imaging. MTA enhances osteogenesis/dentinogenesis by pulp cells or other cells [19]. Yan et al. [19] claimed that MTA could induce dentinogenesis and osteogenesis by apical papillary stem cells. A gap was observed between the MTA filling and hard tissue in this case. This was a limitation of micro-CT evaluation, since we were unable to confirm the nature of this gap. An animal study by Tobias Duarte et al. [20] showed that vital tissue was observed in 67% of specimens after complete pulpal necrosis in immature rat teeth.
Although we tried to obtain a histological section of #45, the specimen had unfortunately broken during sectioning of the decalcified tooth. The thick composite filling may have damaged the tooth specimen damaged during sectioning. Norstat et al. [11] reported that they removed the glass ionomer filling before embedding the histologic section. Peng et al. [12] demonstrated the presence of pulp-like tissue and cementocyte-like cells in the root canal space, in their study of an extracted lower premolar treated with pulp regeneration one year ago. They failed to demonstrate the interface between MTA filling and pulp space in their imaging findings. Another histological study by Norstat et al. [13] showed that MTA was involved in pulp regeneration and the pulp-like tissue was in direct contact with the layer of MTA. However, they used teeth extracted 4 months after regenerative treatment, which was considered a relatively short period for hard tissue formation.
To the best of our knowledge, this is the first case report demonstrating the morphology of a tooth treated by apexification using an MTA barrier and its contralateral tooth using micro-CT. The advantages of micro-CT observation included preservation of the tooth structure and precise observation of the root canal space and apical anatomy. Therefore, apexification or pulp regenerative therapy could be performed in young patients and more information could be obtained if these teeth require extraction for orthodontic or other purposes.
Go to :
 XML Download
XML Download