

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The goal of root canal therapy is to remove and prevent apical periodontitis. To achieve this goal, complete removal of bacteria from the canal is important, as is the choice of filling material [1]. Since gutta-percha was introduced to dentistry as a root canal filling material in the mid-19th century, no significant advancements have been made over the past 170 years except for the introduction of silver cones. Instead, developments in root canal filling materials have focused on the chemical and physical properties of the sealer [2].
Root canal sealers seal off of the root canal system, entombing the remaining bacteria and filling irregularities in the prepared canal. A root canal sealer should display appropriate physicochemical and biological properties. Grossmann suggested that excellent sealing ability, dimensional stability, slow setting time, insolubility, and biocompatibility are required for an ideal root canal sealer [3]. Since the initial development of root canal sealers in the early 20th century, various root canal sealers have been developed to more adequately meet those requirements [2].
Root canal sealers are classified according to their composition as zinc oxide-eugenol (ZOE), calcium hydroxide, glass ionomer, silicone, resin, and bioceramic-based. The sealers included in this review are outlined in Table 1. The earliest, a ZOE-based root canal sealer, was introduced by Rickert in 1931. However, the sealer contained silver, which caused discoloration. In 1958, Grossman introduced a non-staining ZOE sealer as a substitute for Rickert’s formula, and this formula was used for a considerable amount of time. Calcium hydroxide was introduced to endodontics by Herman in 1920 for pulpal repair. It is characterized by its biocompatibility and high pH due to the hydroxyl ion, which induces hard tissue formation and antimicrobial activity. With these advantages, it has been widely used as a pulp capping agent for intracanal medicament and as a root canal sealer. However, calcium hydroxide-based sealers are not physically robust, as demonstrated by their significant leakage [245].
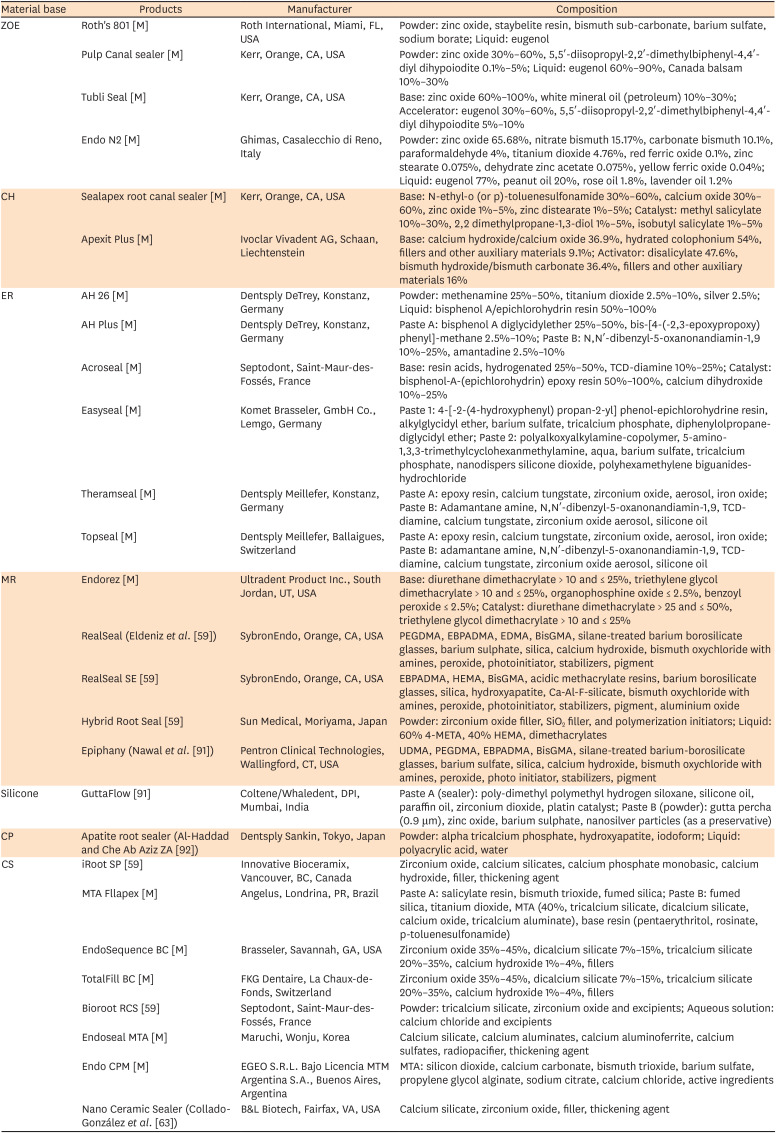
Table 1
Root canal sealers reviewed in this article and their chemical compositions
| Material base | Products | Manufacturer | Composition |
|---|---|---|---|
| ZOE | Roth's 801 [M] | Roth International, Miami, FL, USA | Powder: zinc oxide, staybelite resin, bismuth sub-carbonate, barium sulfate, sodium borate; Liquid: eugenol |
| Pulp Canal sealer [M] | Kerr, Orange, CA, USA | Powder: zinc oxide 30%–60%, 5,5′-diisopropyl-2,2′-dimethylbiphenyl-4,4′-diyl dihypoiodite 0.1%–5%; Liquid: eugenol 60%–90%, Canada balsam 10%–30% | |
| Tubli Seal [M] | Kerr, Orange, CA, USA | Base: zinc oxide 60%–100%, white mineral oil (petroleum) 10%–30%; Accelerator: eugenol 30%–60%, 5,5′-diisopropyl-2,2′-dimethylbiphenyl-4,4′-diyl dihypoiodite 5%–10% | |
| Endo N2 [M] | Ghimas, Casalecchio di Reno, Italy | Powder: zinc oxide 65.68%, nitrate bismuth 15.17%, carbonate bismuth 10.1%, paraformaldehyde 4%, titanium dioxide 4.76%, red ferric oxide 0.1%, zinc stearate 0.075%, dehydrate zinc acetate 0.075%, yellow ferric oxide 0.04%; Liquid: eugenol 77%, peanut oil 20%, rose oil 1.8%, lavender oil 1.2% | |
| CH | Sealapex root canal sealer [M] | Kerr, Orange, CA, USA | Base: N-ethyl-o (or p)-toluenesulfonamide 30%–60%, calcium oxide 30%–60%, zinc oxide 1%–5%, zinc distearate 1%–5%; Catalyst: methyl salicylate 10%–30%, 2,2 dimethylpropane-1,3-diol 1%–5%, isobutyl salicylate 1%–5% |
| Apexit Plus [M] | Ivoclar Vivadent AG, Schaan, Liechtenstein | Base: calcium hydroxide/calcium oxide 36.9%, hydrated colophonium 54%, fillers and other auxiliary materials 9.1%; Activator: disalicylate 47.6%, bismuth hydroxide/bismuth carbonate 36.4%, fillers and other auxiliary materials 16% | |
| ER | AH 26 [M] | Dentsply DeTrey, Konstanz, Germany | Powder: methenamine 25%–50%, titanium dioxide 2.5%–10%, silver 2.5%; Liquid: bisphenol A/epichlorohydrin resin 50%–100% |
| AH Plus [M] | Dentsply DeTrey, Konstanz, Germany | Paste A: bisphenol A diglycidylether 25%–50%, bis-[4-(-2,3-epoxypropoxy) phenyl]-methane 2.5%–10%; Paste B: N,N′-dibenzyl-5-oxanonandiamin-1,9 10%–25%, amantadine 2.5%–10% | |
| Acroseal [M] | Septodont, Saint-Maur-des-Fossés, France | Base: resin acids, hydrogenated 25%–50%, TCD-diamine 10%–25%; Catalyst: bisphenol-A-(epichlorohydrin) epoxy resin 50%–100%, calcium dihydroxide 10%–25% | |
| Easyseal [M] | Komet Brasseler, GmbH Co., Lemgo, Germany | Paste 1: 4-[-2-(4-hydroxyphenyl) propan-2-yl] phenol-epichlorohydrine resin, alkylglycidyl ether, barium sulfate, tricalcium phosphate, diphenylolpropane-diglycidyl ether; Paste 2: polyalkoxyalkylamine-copolymer, 5-amino-1,3,3-trimethylcyclohexanmethylamine, aqua, barium sulfate, tricalcium phosphate, nanodispers silicone dioxide, polyhexamethylene biguanides-hydrochloride | |
| Theramseal [M] | Dentsply Meillefer, Konstanz, Germany | Paste A: epoxy resin, calcium tungstate, zirconium oxide, aerosol, iron oxide; Paste B: Adamantane amine, N,N′-dibenzyl-5-oxanonandiamin-1,9, TCD-diamine, calcium tungstate, zirconium oxide aerosol, silicone oil | |
| Topseal [M] | Dentsply Meillefer, Ballaigues, Switzerland | Paste A: epoxy resin, calcium tungstate, zirconium oxide, aerosol, iron oxide; Paste B: adamantane amine, N,N′-dibenzyl-5-oxanonandiamin-1,9, TCD-diamine, calcium tungstate, zirconium oxide aerosol, silicone oil | |
| MR | Endorez [M] | Ultradent Product Inc., South Jordan, UT, USA | Base: diurethane dimethacrylate > 10 and ≤ 25%, triethylene glycol dimethacrylate > 10 and ≤ 25%, organophosphine oxide ≤ 2.5%, benzoyl peroxide ≤ 2.5%; Catalyst: diurethane dimethacrylate > 25 and ≤ 50%, triethylene glycol dimethacrylate > 10 and ≤ 25% |
| RealSeal (Eldeniz et al. [59]) | SybronEndo, Orange, CA, USA | PEGDMA, EBPADMA, EDMA, BisGMA, silane-treated barium borosilicate glasses, barium sulphate, silica, calcium hydroxide, bismuth oxychloride with amines, peroxide, photoinitiator, stabilizers, pigment | |
| RealSeal SE [59] | SybronEndo, Orange, CA, USA | EBPADMA, HEMA, BisGMA, acidic methacrylate resins, barium borosilicate glasses, silica, hydroxyapatite, Ca-Al-F-silicate, bismuth oxychloride with amines, peroxide, photoinitiator, stabilizers, pigment, aluminium oxide | |
| Hybrid Root Seal [59] | Sun Medical, Moriyama, Japan | Powder: zirconium oxide filler, SiO2 filler, and polymerization initiators; Liquid: 60% 4-META, 40% HEMA, dimethacrylates | |
| Epiphany (Nawal et al. [91]) | Pentron Clinical Technologies, Wallingford, CT, USA | UDMA, PEGDMA, EBPADMA, BisGMA, silane-treated barium-borosilicate glasses, barium sulfate, silica, calcium hydroxide, bismuth oxychloride with amines, peroxide, photo initiator, stabilizers, pigment | |
| Silicone | GuttaFlow [91] | Coltene/Whaledent, DPI, Mumbai, India | Paste A (sealer): poly-dimethyl polymethyl hydrogen siloxane, silicone oil, paraffin oil, zirconium dioxide, platin catalyst; Paste B (powder): gutta percha (0.9 μm), zinc oxide, barium sulphate, nanosilver particles (as a preservative) |
| CP | Apatite root sealer (Al-Haddad and Che Ab Aziz ZA [92]) | Dentsply Sankin, Tokyo, Japan | Powder: alpha tricalcium phosphate, hydroxyapatite, iodoform; Liquid: polyacrylic acid, water |
| CS | iRoot SP [59] | Innovative Bioceramix, Vancouver, BC, Canada | Zirconium oxide, calcium silicates, calcium phosphate monobasic, calcium hydroxide, filler, thickening agent |
| MTA Fllapex [M] | Angelus, Londrina, PR, Brazil | Paste A: salicylate resin, bismuth trioxide, fumed silica; Paste B: fumed silica, titanium dioxide, MTA (40%, tricalcium silicate, dicalcium silicate, calcium oxide, tricalcium aluminate), base resin (pentaerythritol, rosinate, p-toluenesulfonamide) | |
| EndoSequence BC [M] | Brasseler, Savannah, GA, USA | Zirconium oxide 35%–45%, dicalcium silicate 7%–15%, tricalcium silicate 20%–35%, calcium hydroxide 1%–4%, fillers | |
| TotalFill BC [M] | FKG Dentaire, La Chaux-de-Fonds, Switzerland | Zirconium oxide 35%–45%, dicalcium silicate 7%–15%, tricalcium silicate 20%–35%, calcium hydroxide 1%–4%, fillers | |
| Bioroot RCS [59] | Septodont, Saint-Maur-des-Fossés, France | Powder: tricalcium silicate, zirconium oxide and excipients; Aqueous solution: calcium chloride and excipients | |
| Endoseal MTA [M] | Maruchi, Wonju, Korea | Calcium silicate, calcium aluminates, calcium aluminoferrite, calcium sulfates, radiopacifier, thickening agent | |
| Endo CPM [M] | EGEO S.R.L. Bajo Licencia MTM Argentina S.A., Buenos Aires, Argentina | MTA: silicon dioxide, calcium carbonate, bismuth trioxide, barium sulfate, propylene glycol alginate, sodium citrate, calcium chloride, active ingredients | |
| Nano Ceramic Sealer (Collado-González et al. [63]) | B&L Biotech, Fairfax, VA, USA | Calcium silicate, zirconium oxide, filler, thickening agent |
ZOE, zinc oxide-eugenol; CH, calcium hydroxide; ER, epoxy resin; MR, methacrylate resin; CP, calcium phosphate; CS, calcium silicate; M, provided from manufacturer; 4‐META, 4‐methacryloxyethyl trimellitic anhydride; HEMA, 2‐hydroxyethyl methacrylate; TCD, tricyclodecane; PEGDMA, polyethylene glycol dimethacrylate; EBPADMA, ethoxylated bisphenol A dimethacrylate; EDMA, 3,4-ethylenedioxy-N-methylamphetamine; BisGMA, bisphenol A-glycidyl methacrylate; UDMA, urethane dimethylate.
![]()
Among the clinically available root canal sealers, epoxy resin-based sealers are currently widely used. The prototype of the AH series was introduced by Schroeder in 1957, with excellent physical properties and sealing ability. AH Plus (Dentsply DeTrey, Konstanz, Germany) resolved the problem seen in AH 26-leaching formaldehyde during setting [45]. Several studies have considered AH Plus to be the gold standard for sealers, due to its resorption resistance and dimensional stability [6789]. However, it has limitations, such as possible mutagenicity [10], cytotoxicity [1112], and an inflammatory response [13]. In addition, its hydrophobicity prevents the complete filling of the hydrophilic canal. Specifically, defects in AH Plus adhesion to the canal walls can occur due to retained dental moisture [14].
Mineral trioxide aggregate (MTA), a calcium silicate-based hydrophilic cement, was introduced to dentistry in the early 1990s as a material displaying superior biological and physical properties [15161718]. With its good sealing ability, biocompatibility, and osteoconductivity, it was initially used as a root-end filling material, but is now widely used for various applications, such as root perforation repair, pulp-dentin regeneration, apical barrier formation, pulp capping, pulpotomy, and root canal filling [1719]. With these excellent properties of calcium silicate-based cements, endodontic sealers based on calcium silicate have been introduced. This kind of sealer sets by reacting with water or under humid conditions. In 2007, the first calcium silicate-based sealer, iRoot SP (Innovative Bioceramix, Vancouver, BC, Canada), was introduced, and displayed biocompatibility and hydrophilicity [20]. Since then, various sealers have been introduced to the market, making various claims but exhibiting small improvements.
Even though various calcium silicate-based root canal sealers are commercially available, some are still in early stages, requiring further laboratory and clinical study. Therefore, in this review, the 5 most studied calcium silicate-based sealers are included: iRoot SP, EndoSequence BC (Brasseler, Savannah, GA, USA), BioRoot RCS (Septodont, Saint-Maur-des -Fossés, France), MTA Fillapex (Angelus, Londrina, PR, Brazil), and Endoseal MTA (Maruchi, Wonju, Korea).
This review aims to summarize the properties of calcium silicate-based sealers and to compare them with those of the resin-based sealer, AH Plus. First, physical properties such as water sorption and solubility, leakage or sealing ability, and push-out bond strength are discussed. Then, biological properties such as biocompatibility, antimicrobial activity, and bioactive potential are presented and compared.
Go to : 
REVIEW
Physical properties
1. Water sorption and solubility
Water sorption and solubility are related to dimensional stability. Table 2 compares the dimensional stability of calcium silicate sealers and conventional sealers. Calcium silicate sealers produce calcium hydroxide by hydration, which affects water sorption and solubility more than is the case for conventional resin-based sealers. The favorable biological properties of calcium silicate sealers result from their solubility or water absorption, but these factors can decrease dimensional stability, with a negative impact on the sealing quality of root canals [202122].
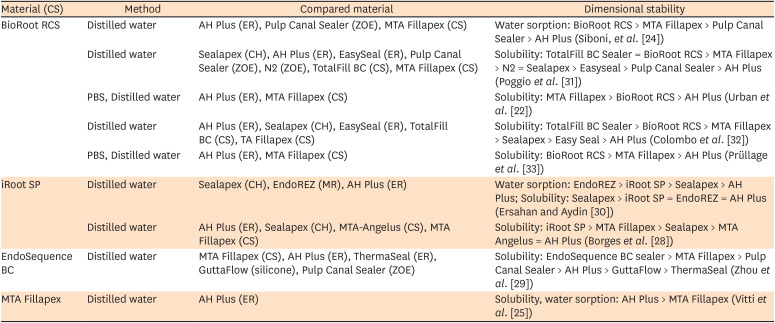
Table 2
Dimensional stability of calcium silicate sealers in the articles included in this review
| Material (CS) | Method | Compared material | Dimensional stability |
|---|---|---|---|
| BioRoot RCS | Distilled water | AH Plus (ER), Pulp Canal Sealer (ZOE), MTA Fillapex (CS) | Water sorption: BioRoot RCS > MTA Fillapex > Pulp Canal Sealer > AH Plus (Siboni, et al. [24]) |
| Distilled water | Sealapex (CH), AH Plus (ER), EasySeal (ER), Pulp Canal Sealer (ZOE), N2 (ZOE), TotalFill BC (CS), MTA Fillapex (CS) | Solubility: TotalFill BC Sealer = BioRoot RCS > MTA Fillapex > N2 = Sealapex > Easyseal > Pulp Canal Sealer > AH Plus (Poggio et al. [31]) | |
| PBS, Distilled water | AH Plus (ER), MTA Fillapex (CS) | Solubility: MTA Fillapex > BioRoot RCS > AH Plus (Urban et al. [22]) | |
| Distilled water | AH Plus (ER), Sealapex (CH), EasySeal (ER), TotalFill BC (CS), MTA Fillapex (CS) | Solubility: TotalFill BC Sealer > BioRoot RCS > MTA Fillapex > Sealapex > Easy Seal > AH Plus (Colombo et al. [32]) | |
| PBS, Distilled water | AH Plus (ER), MTA Fillapex (CS) | Solubility: BioRoot RCS > MTA Fillapex > AH Plus (Prüllage et al. [33]) | |
| iRoot SP | Distilled water | Sealapex (CH), EndoREZ (MR), AH Plus (ER) | Water sorption: EndoREZ > iRoot SP > Sealapex > AH Plus; Solubility: Sealapex > iRoot SP = EndoREZ = AH Plus (Ersahan and Aydin [30]) |
| Distilled water | AH Plus (ER), Sealapex (CH), MTA-Angelus (CS), MTA Fillapex (CS) | Solubility: iRoot SP > MTA Fillapex > Sealapex > MTA Angelus = AH Plus (Borges et al. [28]) | |
| EndoSequence BC | Distilled water | MTA Fillapex (CS), AH Plus (ER), ThermaSeal (ER), GuttaFlow (silicone), Pulp Canal Sealer (ZOE) | Solubility: EndoSequence BC sealer > MTA Fillapex > Pulp Canal Sealer > AH Plus > GuttaFlow > ThermaSeal (Zhou et al. [29]) |
| MTA Fillapex | Distilled water | AH Plus (ER) | Solubility, water sorption: AH Plus > MTA Fillapex (Vitti et al. [25]) |
CS, calcium silicate; ER, epoxy resin; ZOE, zinc oxide-eugenol; CH, calcium hydroxide; MR, methacrylate resin.
![]()
Water sorption of calcium silicate sealers promotes slight expansion and promotes sealing [23]. A study reported that BioRoot RCS demonstrated high initial water sorption after setting; however, water sorption decreased 7 days after setting [24]. Only 1 study showed lower water sorption of calcium silicate sealers compared to conventional epoxy resin sealers [25].
The solubility standards of root canal sealers are well described in International Organization for Standardization (ISO) 6876: 2012, according to which sealers should exhibit a solubility of less than 3% weight loss after water immersion [26]. The solubility of calcium silicate-based sealers is higher than that of epoxy resin-based sealers [22
272829303132]. In several articles, BioRoot RCS and iRoot SP lost more than 3% weight after water immersion [24283132]. Ersahan and Aydin [30] reported no significant difference between the solubility of AH Plus and iRoot SP. Only 1 study reported that the solubility of MTA Fillapex was lower than that of AH Plus. However, the authors concluded that both sealers satisfied the ISO 6876: 2012 standard [25]. BioRoot RCS showed less solubility when immersed in phosphate-buffered saline (PBS) than when immersed in distilled water [2233]. Although ISO 6876: 2012 requires the use of distilled water, it does not predict the sealer’s exact stability in the applicable biological environment. Therefore, some studies have used PBS to provide a better understanding of sealer solubility in biological fluids. In addition, the long-term solubility of BioRoot RCS satisfied the ISO 6876: 2012 requirements when stored in PBS [22].
2. Microleakage
Sealing ability is an important property of a sealer, as one of the goals of root canal therapy is to obtain a bacteria-tight seal of the canals. Wu et al. [34] proposed an experimental model for assessing leakage known as the fluid transport method. It can provide a quantitative measurement of microleakage without destruction of the specimen, and its sensitivity can be adjusted by altering the pressure and diameter of the micropipette.
In contrast, to evaluate dentin penetration, a confocal laser scanning microscopy (CLSM) assay is used. After canal obturation with each sealer, roots are embedded in a self-cure resin and sectioned perpendicular to the long axis of the root. Then, CLSM is used to evaluate the patterns or depth of dentin-penetrating sealer [35]. In the evaluation of dye leakage, each root is immersed in freshly prepared 1% methylene blue dye for 72 hours after canal obturation. Roots are sectioned longitudinally and scored by the depth of dye penetration [3637].
As shown in Table 3 the sealing ability of calcium silicate sealers varies among studies due to differences in experimental methods and materials. Overall, conventional epoxy resin-based sealers show similar or significantly lower leakage than calcium silicate-based sealers. However, in some leakage studies using the dye penetration method, the leakage of conventional resin-based sealers was significantly higher than that of calcium silicate-based sealers [3637]. Furthermore, the leakage of calcium silicate sealers and conventional resin sealers may change over time. In a study by Asawaworarit et al. [23], conventional resin-based sealers showed better sealing after 7 days. However, calcium silicate-based sealers showed better sealing at 4 weeks after setting. The authors concluded that the calcium silicate sealer exhibited a better seal after complete setting [23]. Although experimental methods can influence the results, leakage studies can achieve predictable outcomes when standardized techniques, large sample sizes, and proper control groups are used [38].
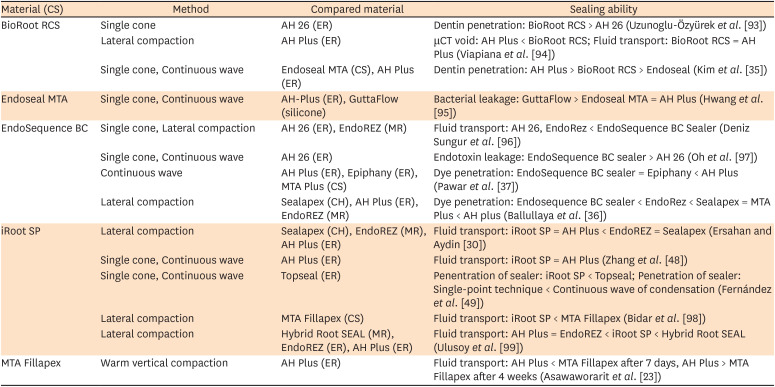
Table 3
Sealing ability of the calcium silicate sealers in the articles included in this review
| Material (CS) | Method | Compared material | Sealing ability |
|---|---|---|---|
| BioRoot RCS | Single cone | AH 26 (ER) | Dentin penetration: BioRoot RCS > AH 26 (Uzunoglu-Özyürek et al. [93]) |
| Lateral compaction | AH Plus (ER) | μCT void: AH Plus < BioRoot RCS; Fluid transport: BioRoot RCS = AH Plus (Viapiana et al. [94]) | |
| Single cone, Continuous wave | Endoseal MTA (CS), AH Plus (ER) | Dentin penetration: AH Plus > BioRoot RCS > Endoseal (Kim et al. [35]) | |
| Endoseal MTA | Single cone, Continuous wave | AH-Plus (ER), GuttaFlow (silicone) | Bacterial leakage: GuttaFlow > Endoseal MTA = AH Plus (Hwang et al. [95]) |
| EndoSequence BC | Single cone, Lateral compaction | AH 26 (ER), EndoREZ (MR) | Fluid transport: AH 26, EndoRez < EndoSequence BC Sealer (Deniz Sungur et al. [96]) |
| Single cone, Continuous wave | AH 26 (ER) | Endotoxin leakage: EndoSequence BC sealer > AH 26 (Oh et al. [97]) | |
| Continuous wave | AH Plus (ER), Epiphany (ER), MTA Plus (CS) | Dye penetration: EndoSequence BC sealer = Epiphany < AH Plus (Pawar et al. [37]) | |
| Lateral compaction | Sealapex (CH), AH Plus (ER), EndoREZ (MR) | Dye penetration: Endosequence BC sealer < EndoRez < Sealapex = MTA Plus < AH plus (Ballullaya et al. [36]) | |
| iRoot SP | Lateral compaction | Sealapex (CH), EndoREZ (MR), AH Plus (ER) | Fluid transport: iRoot SP = AH Plus < EndoREZ = Sealapex (Ersahan and Aydin [30]) |
| Single cone, Continuous wave | AH Plus (ER) | Fluid transport: iRoot SP = AH Plus (Zhang et al. [48]) | |
| Single cone, Continuous wave | Topseal (ER) | Penentration of sealer: iRoot SP < Topseal; Penetration of sealer: Single-point technique < Continuous wave of condensation (Fernández et al. [49]) | |
| Lateral compaction | MTA Fillapex (CS) | Fluid transport: iRoot SP < MTA Fillapex (Bidar et al. [98]) | |
| Lateral compaction | Hybrid Root SEAL (MR), EndoREZ (ER), AH Plus (ER) | Fluid transport: AH Plus = EndoREZ < iRoot SP < Hybrid Root SEAL (Ulusoy et al. [99]) | |
| MTA Fillapex | Warm vertical compaction | AH Plus (ER) | Fluid transport: AH Plus < MTA Fillapex after 7 days, AH Plus > MTA Fillapex after 4 weeks (Asawaworarit et al. [23]) |
CS, calcium silicate; ER, epoxy resin; μCT, micro-computed tomography; CH, calcium hydroxide; MR, methacrylate resin.
![]()
Another characteristic related to the leakage of calcium silicate sealer is biomineralization. Calcium silicate produces a tag-like structure at the calcium silicate/dentin interface. The so-called “mineral infiltration zone” is a hybrid zone where hydroxyapatite recrystallization occurs when calcium silicate is applied in dentin [39]. However, it has not been definitively proven that the mineral infiltration zone affects the outcome of endodontic treatment, positively or negatively [40]. It might positively impact outcomes because calcium ions react with the carbon dioxide in the tissue to form calcite crystals [41]. These crystals can reduce marginal gaps and porosity, and increase the retention of the cement [4243]. Conversely, in some studies, apatite deposition by a calcium silicate-based sealer did not reduce leakage because of its porous shape [44].
Ethylenediaminetetraacetic acid (EDTA) treatment as the final irrigation can increase the bond strength of epoxy resin-based sealers and decrease leakage [45]. However, the use of EDTA for the final irrigation can disrupt the hydration of calcium silicate, which decreases the hardness and biocompatibility of calcium silicate sealer due to calcium chelation by EDTA [46]. Conversely, using NaOCl for the final irrigation creates an alkaline environment that is suitable for calcium silicate cement hydration and improves the sealing ability of calcium silicate-based sealers [23].
The leakage of calcium silicate-based sealers using different obturation techniques has also been compared. The single cone technique requires a greater amount of sealer than other filling techniques [4748]. In contrast, Jeong et al. [40] showed that the hygroscopic expansion of calcium silicate-based sealers did not enhance the dentinal penetration depth, and concluded that dentinal penetration was independent of the obturation technique. In addition, a calcium silicate sealer showed similar leakage rates regardless of whether the single cone technique or the continuous wave technique was used [48]. However, in another study, a calcium silicate-based sealer showed better filling when obturated by the continuous wave technique, and not the single cone technique recommended by the manufacturer [49].
3. Push-out bond strength
Push-out bond strength is used to evaluate interfacial bond strength between the root canal sealer and radicular dentin [5051]. Calcium silicate-based sealers display improved dislocation resistance, as they micromechanically bond to dentin, which decreases the gap at the interface [52]. Some studies showed that calcium silicate sealers had a push-out strength comparable to that of conventional resin-based sealers. However, they generally display a lower push-out bond strength than resin-based sealers that chemically bond to dentin (Table 4).
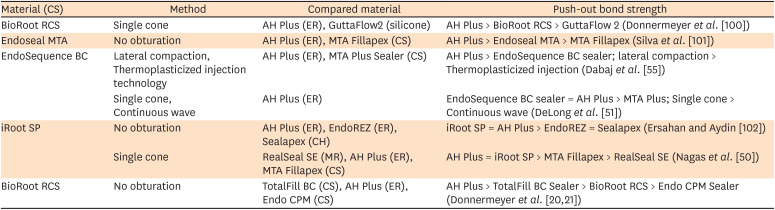
Table 4
Push-out bond strength of the calcium silicate sealers in the articles included in this review
| Material (CS) | Method | Compared material | Push-out bond strength |
|---|---|---|---|
| BioRoot RCS | Single cone | AH Plus (ER), GuttaFlow2 (silicone) | AH Plus > BioRoot RCS > GuttaFlow 2 (Donnermeyer et al. [100]) |
| Endoseal MTA | No obturation | AH Plus (ER), MTA Fillapex (CS) | AH Plus > Endoseal MTA > MTA Fillapex (Silva et al. [101]) |
| EndoSequence BC | Lateral compaction, Thermoplasticized injection technology | AH Plus (ER), MTA Plus Sealer (CS) | AH Plus > EndoSequence BC sealer; lateral compaction > Thermoplasticized injection (Dabaj et al. [55]) |
| Single cone, Continuous wave | AH Plus (ER) | EndoSequence BC sealer = AH Plus > MTA Plus; Single cone > Continuous wave (DeLong et al. [51]) | |
| iRoot SP | No obturation | AH Plus (ER), EndoREZ (ER), Sealapex (CH) | iRoot SP = AH Plus > EndoREZ = Sealapex (Ersahan and Aydin [102]) |
| Single cone | RealSeal SE (MR), AH Plus (ER), MTA Fillapex (CS) | AH Plus = iRoot SP > MTA Fillapex > RealSeal SE (Nagas et al. [50]) | |
| BioRoot RCS | No obturation | TotalFill BC (CS), AH Plus (ER), Endo CPM (CS) | AH Plus > TotalFill BC Sealer > BioRoot RCS > Endo CPM Sealer (Donnermeyer et al. [2021]) |
![]()
The push-out bond strength varies in calcium silicate-based sealers depending on the obturation technique employed. The single cone technique is recommended in each manufacturer's instructions. Sealer properties are affected by the application of heat during warm vertical compaction. Under heated conditions, conventional resin-based sealers exhibit increased film thickness and reduced setting time and strength [5354]. Heat can accelerate hydration and hydroxyapatite formation in calcium silicate-based root canal sealers [55]. Faster setting times [56] decrease flowability [53] and result in lower bond strength of the calcium silicate-based sealer [55]. In a study by Dabaj et al. [55], a calcium silicate sealer showed a lower bond strength with the thermo-plasticized injectable technique than when cold lateral condensation was used. Residual water in the tubular orifice can be evaporated by heat application, which could result in insufficient hydration. Therefore, calcium silicate-based sealers should be used with the single cone technique, as recommended in the manufacturer's manual.
Biological properties
1. Biocompatibility
Biocompatibility is a requirement for a root canal sealer because the sealer directly contacts the periradicular tissue at the apical and lateral foramina of the root [2]. Most studies analyzed in this review that assessed the cytotoxicity of sealers used mouse and human fibroblast cells or human periodontal ligament cells (PDLCs) [5758596061]. Clinically, sealers are inserted into root canals before setting; thus, it is possible that toxic components are released into the tissue [6062]. Leachable toxic substances could also be released after setting. For this reason, the cytotoxicity of sealers needs to be evaluated both before and after setting.
Generally, calcium silicate sealers have shown higher cell viability than AH Plus (Table 5). However, it cannot be concluded which calcium silicate sealer is the most biocompatible, although BioRoot RCS could be considered more biocompatible than iRoot SP, MTA Fillapex, and Endoseal MTA within the limitations of this review article [3259606163]. Despite the similar chemical characteristics of calcium silicate-based sealers, they showed different cytocompatibility [64]. These results were ascribed to differences between commercially available calcium silicate-based sealers, such as unknown filler and thickening agents.
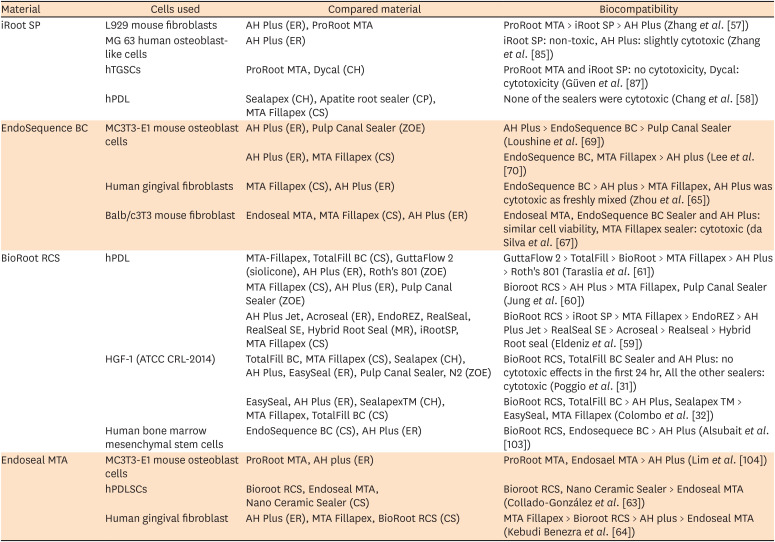
Table 5
Biocompatibility of the calcium silicate sealers in the articles included in this review
| Material | Cells used | Compared material | Biocompatibility |
|---|---|---|---|
| iRoot SP | L929 mouse fibroblasts | AH Plus (ER), ProRoot MTA | ProRoot MTA > iRoot SP > AH Plus (Zhang et al. [57]) |
| MG 63 human osteoblast-like cells | AH Plus (ER) | iRoot SP: non-toxic, AH Plus: slightly cytotoxic (Zhang et al. [85]) | |
| hTGSCs | ProRoot MTA, Dycal (CH) | ProRoot MTA and iRoot SP: no cytotoxicity, Dycal: cytotoxicity (Güven et al. [87]) | |
| hPDL | Sealapex (CH), Apatite root sealer (CP), MTA Fillapex (CS) | None of the sealers were cytotoxic (Chang et al. [58]) | |
| EndoSequence BC | MC3T3-E1 mouse osteoblast cells | AH Plus (ER), Pulp Canal Sealer (ZOE) | AH Plus > EndoSequence BC > Pulp Canal Sealer (Loushine et al. [69]) |
| AH Plus (ER), MTA Fillapex (CS) | EndoSequence BC, MTA Fillapex > AH plus (Lee et al. [70]) | ||
| Human gingival fibroblasts | MTA Fillapex (CS), AH Plus (ER) | EndoSequence BC > AH plus > MTA Fillapex, AH Plus was cytotoxic as freshly mixed (Zhou et al. [65]) | |
| Balb/c3T3 mouse fibroblast | Endoseal MTA, MTA Fillapex (CS), AH Plus (ER) | Endoseal MTA, EndoSequence BC Sealer and AH Plus: similar cell viability, MTA Fillapex sealer: cytotoxic (da Silva et al. [67]) | |
| BioRoot RCS | hPDL | MTA-Fillapex, TotalFill BC (CS), GuttaFlow 2 (siolicone), AH Plus (ER), Roth's 801 (ZOE) | GuttaFlow 2 > TotalFill > BioRoot > MTA Fillapex > AH Plus > Roth's 801 (Taraslia et al. [61]) |
| MTA Fillapex (CS), AH Plus (ER), Pulp Canal Sealer (ZOE) | Bioroot RCS > AH Plus > MTA Fillapex, Pulp Canal Sealer (Jung et al. [60]) | ||
| AH Plus Jet, Acroseal (ER), EndoREZ, RealSeal, RealSeal SE, Hybrid Root Seal (MR), iRootSP, MTA Fillapex (CS) | BioRoot RCS > iRoot SP > MTA Fillapex > EndoREZ > AH Plus Jet > RealSeal SE > Acroseal > Realseal > Hybrid Root seal (Eldeniz et al. [59]) | ||
| HGF-1 (ATCC CRL-2014) | TotalFill BC, MTA Fillapex (CS), Sealapex (CH), AH Plus, EasySeal (ER), Pulp Canal Sealer, N2 (ZOE) | BioRoot RCS, TotalFill BC Sealer and AH Plus: no cytotoxic effects in the first 24 hr, All the other sealers: cytotoxic (Poggio et al. [31]) | |
| EasySeal, AH Plus (ER), SealapexTM (CH), MTA Fillapex, TotalFill BC (CS) | BioRoot RCS, TotalFill BC > AH Plus, Sealapex TM > EasySeal, MTA Fillapex (Colombo et al. [32]) | ||
| Human bone marrow mesenchymal stem cells | EndoSequence BC (CS), AH Plus (ER) | BioRoot RCS, Endosequece BC > AH Plus (Alsubait et al. [103]) | |
| Endoseal MTA | MC3T3-E1 mouse osteoblast cells | ProRoot MTA, AH plus (ER) | ProRoot MTA, Endosael MTA > AH Plus (Lim et al. [104]) |
| hPDLSCs | Bioroot RCS, Endoseal MTA, Nano Ceramic Sealer (CS) | Bioroot RCS, Nano Ceramic Sealer > Endoseal MTA (Collado-González et al. [63]) | |
| Human gingival fibroblast | AH Plus (ER), MTA Fillapex, BioRoot RCS (CS) | MTA Fillapex > Bioroot RCS > AH plus > Endoseal MTA (Kebudi Benezra et al. [64]) |
MR, methacrylate resin; ER, epoxy resin; hTGSC, human tooth germ stem cell; CH, calcium hydroxide; hPDL, human periodontal ligament; CP, calcium phosphate; ZOE, zinc oxide-eugenol; CS, calcium silicate; HGF-1, human gingival fibroblast; hPDLSC, human periodontal ligament stem cell.
![]()
However, MTA Fillapex showed the least biocompatibility among the calcium silicate sealers [3259606165] except in 2 articles [5864], as well as significant cytotoxicity [6667]. The main component of MTA Fillapex is salicylate resin, which has shown considerable cytotoxicity and prolongation of setting [68], contributing to increased dissolution of toxic materials. MTA Fillapex was found to be more soluble than AH Plus even after setting [33]. However, according to the recent study of Kebudi et al. [64], MTA Fillapex enhanced cell attachment and proliferation, in contrast to previous studies; these findings were suggested to be due to a compositional change in the re-launched material, with calcium tungstate substituted for bismuth oxide.
While most studies have shown that calcium silicate sealers are biocompatible and non-cytotoxic, several reports have found the contrary. Loushine et al. [69] reported that EndoSequence BC was cytotoxic to mouse osteoblast cells for 6 weeks, and Endoseal MTA was reported not to promote the growth of human gingival fibroblasts on its surface [64]. In vitro methods such as direct testing on the surface of the sealer, and cell culture of extract from the sealer or transwell inserts including it [646569], could yield different results. The cell line chosen to test the biocompatibility also greatly influences the results [63]. Fortunately, the results reported from different studies in this review are consistent, regardless of the cell line that was used. On the contrary, 2 separate investigations of EndoSequence BC reported differences in biocompatibility, even though the same mouse osteoblast cell line was used [6970]. This difference may be related to differences in experimental conditions.
2. Antibacterial effects
Complete elimination of microbes from the root canal system is impossible. Thus, the use of root canal sealers with antibacterial effects is essential for the prevention of intracanal infections or bacterial invasion due to microleakage [7172]. Enterococcus faecalis is the most frequently isolated microorganism from infected root canals, especially in recurrent infections after root canal treatment [73]. Therefore, most studies have evaluated the antibacterial effect of sealers against E. faecalis.
Previous research has shown that the antimicrobial properties of root canal sealers depend upon their alkalinity [74]. The alkalinity of calcium silicate sealers is higher than that of AH Plus. The highest pH values were observed in iRoot SP, EndoSequence BC, and Endo CPM, followed by MTA Fillapex and Endoseal MTA [75]. In addition, hydrophilicity and calcium hydroxide diffusion also affect antimicrobial properties. Hydrophilicity reduces the contact angle of the sealer and increases sealer penetration into the dentinal tubule [71]. Calcium hydroxide diffusion helps to deliver the hydroxyl ion through the root canal, including the dentinal tubules, fins, isthmuses, lateral canals, and accessory canals, where residual microbes may be located [76].
The agar diffusion test [7778] and the direct contact test are commonly used to evaluate the antimicrobial activity of root canal sealers [7177]. Recently, CLSM has been introduced to evaluate the penetration of microorganisms, which can be observed by fluorescent-staining cells in the dentinal tubule after root canal filling [787980]. The antimicrobial effects of calcium silicate sealers depend on the material, method, and time, as they decrease after setting.
Most calcium silicate sealers showed antibacterial effects against E. faecalis (Table 6) [3271777879808182]. For iRoot SP, all bacteria were eradicated directly after contact, whereas for AH Plus, the viable bacteria were significantly reduced and eradicated within 5–20 minutes. However, after 7 days, most sealers had lost their antibacterial effect [71]. BioRoot RCS showed stronger antibacterial effects than AH Plus in several studies [327880], and its effects lasted for 30 days [80]. However, EndoSequence BC showed antibacterial effects in 2 articles and no effect in 1 other article that we reviewed [798283]. The discrepancy in these results may stem from differences in the testing method. There were only 3 articles about the antibacterial activity of Endosequence BC; therefore, further evaluation is needed. Endoseal MTA showed a stronger antibacterial effect against E. faecalis than EndoSequence BC, due to higher levels of metal oxides, such as Na2O, MgO, Al2O3, SO2, and Fe2O [82]. However, only 1 report has dealt with the antibacterial effects of Endoseal MTA; as such, the limitations of our knowledge mean that further studies are required for a definitive assessment.
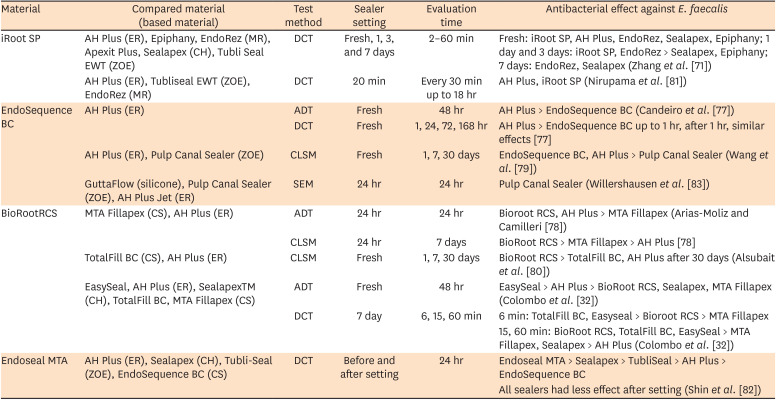
Table 6
Antibacterial effects on Enterococcus faecalis of the various calcium silicate sealers in the articles included in this review
| Material | Compared material (based material) | Test method | Sealer setting | Evaluation time | Antibacterial effect against E. faecalis |
|---|---|---|---|---|---|
| iRoot SP | AH Plus (ER), Epiphany, EndoRez (MR), Apexit Plus, Sealapex (CH), Tubli Seal EWT (ZOE) | DCT | Fresh, 1, 3, and 7 days | 2–60 min | Fresh: iRoot SP, AH Plus, EndoRez, Sealapex, Epiphany; 1 day and 3 days: iRoot SP, EndoRez > Sealapex, Epiphany; 7 days: EndoRez, Sealapex (Zhang et al. [71]) |
| AH Plus (ER), Tubliseal EWT (ZOE), EndoRez (MR) | DCT | 20 min | Every 30 min up to 18 hr | AH Plus, iRoot SP (Nirupama et al. [81]) | |
| EndoSequence BC | AH Plus (ER) | ADT | Fresh | 48 hr | AH Plus > EndoSequence BC (Candeiro et al. [77]) |
| DCT | Fresh | 1, 24, 72, 168 hr | AH Plus > EndoSequence BC up to 1 hr, after 1 hr, similar effects [77] | ||
| AH Plus (ER), Pulp Canal Sealer (ZOE) | CLSM | Fresh | 1, 7, 30 days | EndoSequence BC, AH Plus > Pulp Canal Sealer (Wang et al. [79]) | |
| GuttaFlow (silicone), Pulp Canal Sealer (ZOE), AH Plus Jet (ER) | SEM | 24 hr | 24 hr | Pulp Canal Sealer (Willershausen et al. [83]) | |
| BioRootRCS | MTA Fillapex (CS), AH Plus (ER) | ADT | 24 hr | 24 hr | Bioroot RCS, AH Plus > MTA Fillapex (Arias-Moliz and Camilleri [78]) |
| CLSM | 24 hr | 7 days | BioRoot RCS > MTA Fillapex > AH Plus [78] | ||
| TotalFill BC (CS), AH Plus (ER) | CLSM | Fresh | 1, 7, 30 days | BioRoot RCS > TotalFill BC, AH Plus after 30 days (Alsubait et al. [80]) | |
| EasySeal, AH Plus (ER), SealapexTM (CH), TotalFill BC, MTA Fillapex (CS) | ADT | Fresh | 48 hr | EasySeal > AH Plus > BioRoot RCS, Sealapex, MTA Fillapex (Colombo et al. [32]) | |
| DCT | 7 day | 6, 15, 60 min | 6 min: TotalFill BC, Easyseal > Bioroot RCS > MTA Fillapex | ||
| 15, 60 min: BioRoot RCS, TotalFill BC, EasySeal > MTA Fillapex, Sealapex > AH Plus (Colombo et al. [32]) | |||||
| Endoseal MTA | AH Plus (ER), Sealapex (CH), Tubli-Seal (ZOE), EndoSequence BC (CS) | DCT | Before and after setting | 24 hr | Endoseal MTA > Sealapex > TubliSeal > AH Plus > EndoSequence BC |
| All sealers had less effect after setting (Shin et al. [82]) |
ER, epoxy resin; MR, methacrylate resin; CH, calcium hydroxide; ZOE, zinc oxide-eugenol; DCT, direct contact test; ADT, agar diffusion test; CLSM, confocal laser scanning microscopy; SEM, scanning electron microscopy; CS, calcium silicate.
![]()
3. Bioactivity
Bioactive materials are bone-bonding materials that form bone-like apatite upon immersion in a serum-like solution [84]. Similarly, calcium silicate-based sealers are considered to be bioactive materials because they can induce hard tissue formation in both the periodontal ligament (PDL) and bone [8586]. Bioactive properties can be evaluated through osteogenic differentiation and mineralization potential. These properties have been assessed in terms of alkaline phosphatase activity, alizarin red staining, and mineralization-related gene expression [58708788].
Most research has concluded that calcium silicate sealers show stronger bioactive effects on PDL, osteoblasts, and stem cells than other sealers. As shown in Table 7, calcium silicate sealers improve the expression of osteoblastic marker genes and induce an higher amount of mineralization matrix than other types of sealers [245870858687888990].
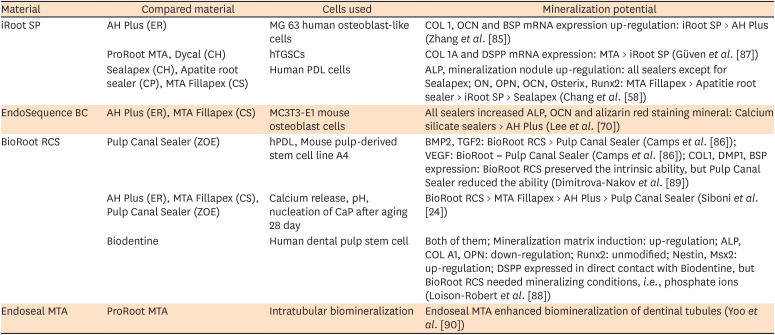
Table 7
Bioactivity of the calcium silicate sealers in the articles included in this review
| Material | Compared material | Cells used | Mineralization potential |
|---|---|---|---|
| iRoot SP | AH Plus (ER) | MG 63 human osteoblast-like cells | COL 1, OCN and BSP mRNA expression up-regulation: iRoot SP > AH Plus (Zhang et al. [85]) |
| ProRoot MTA, Dycal (CH) | hTGSCs | COL 1A and DSPP mRNA expression: MTA > iRoot SP (Güven et al. [87]) | |
| Sealapex (CH), Apatite root sealer (CP), MTA Fillapex (CS) | Human PDL cells | ALP, mineralization nodule up-regulation: all sealers except for Sealapex; ON, OPN, OCN, Osterix, Runx2: MTA Fillapex > Apatitie root sealer > iRoot SP > Sealapex (Chang et al. [58]) | |
| EndoSequence BC | AH Plus (ER), MTA Fillapex (CS) | MC3T3-E1 mouse osteoblast cells | All sealers increased ALP, OCN and alizarin red staining mineral: Calcium silicate sealers > AH Plus (Lee et al. [70]) |
| BioRoot RCS | Pulp Canal Sealer (ZOE) | hPDL, Mouse pulp-derived stem cell line A4 | BMP2, TGF2: BioRoot RCS > Pulp Canal Sealer (Camps et al. [86]); VEGF: BioRoot = Pulp Canal Sealer (Camps et al. [86]); COL1, DMP1, BSP expression: BioRoot RCS preserved the intrinsic ability, but Pulp Canal Sealer reduced the ability (Dimitrova-Nakov et al. [89]) |
| AH Plus (ER), MTA Fillapex (CS), Pulp Canal Sealer (ZOE) | Calcium release, pH, nucleation of CaP after aging 28 day | BioRoot RCS > MTA Fillapex > AH Plus > Pulp Canal Sealer (Siboni et al. [24]) | |
| Biodentine | Human dental pulp stem cell | Both of them; Mineralization matrix induction: up-regulation; ALP, COL A1, OPN: down-regulation; Runx2: unmodified; Nestin, Msx2: up-regulation; DSPP expressed in direct contact with Biodentine, but BioRoot RCS needed mineralizing conditions, i.e., phosphate ions (Loison-Robert et al. [88]) | |
| Endoseal MTA | ProRoot MTA | Intratubular biomineralization | Endoseal MTA enhanced biomineralization of dentinal tubules (Yoo et al. [90]) |
ER, epoxy resin; COL, collagen; OCN, osteocalcin; BSP, bone sialoprotein; CH, calcium hydroxide; hTGSC, human tooth germ stem cell; DSPP, dentin sialophosphoprotein; CP, calcium phosphate; CS, calcium silicate; PDL, periodontal ligament; ALP, alkaline phosphatase; ON, osteonectin; OPN, osteopontin; Runx, runt-related transcription factor; ZOE, zinc oxide-eugenol; hPDL, human periodontal ligament; BMP, bone morphogenic protein; TGF, transforming growth factor; VEGF, vascular endothelial growth factor; DMP, dentin matrix protein; BSP, bone sialoprotein; CaP, calcium phosphate; Msx, msh homeobox.
![]()
iRoot SP induces human tooth germ stem cell differentiation into odontoblast-like cells [87], and further induces osteoblast-like cells to produce more mineralized matrix gene and protein expression [85]. However, iRoot SP has less inductive potential and hard tissue deposition compared to ProRoot MTA [87]. Apatite Root Sealer, MTA Fillapex, and iRoot SP demonstrated osteogenic potential through osteoblastic differentiation of PDLCs compared with Sealapex [58]. BioRoot RCS had higher bioactivity than ZOE sealers on mouse pulp-derived stem cells and human PDLCs [8689]. Human dental pulp stem cells also showed significantly increased mineralization in the presence of BioRoot RCS [88]. The osteogenic potential of calcium silicate sealers seems to be higher than that of AH Plus. Calcium release from calcium silicate sealers is thought to promote osteoblastic differentiation and calcium nodule formation [247085].
Studies have also been conducted regarding direct mineral deposition. When the surfaces of sealers immersed in Hank's balanced salt solution were examined with elemental dispersive X-ray microanalysis, BioRoot RCS induced carbonated apatite deposits, with a prolonged ability to release calcium ions and alkalization [24]. In addition, when the root canal was obturated with GP and Endoseal MTA sealer, the biomineralization of the dentinal tubules was confirmed by observations using scanning electron microscopy and energy-dispersive spectroscopy [90]. Therefore, it can be concluded that calcium silicate-based sealers are bioactive and stimulate hard tissue formation.
Go to :
CONCLUSIONS
Endodontic sealers are used to seal minor discrepancies between the dentinal wall of the root canal and the root filling material, including irregularities in the apical foramen and canal. Therefore, the physical properties of root canal sealers have a major impact on the quality of the root canal filling. Due to the hydrophilic environment of root canals, water resorption and the solubility of root canal sealers are important factors for their 3-dimensional stability.
Minimal microleakage of the sealer and high push-out bond strength are needed to endure the dynamic tooth environment. Although these physical properties of calcium silicate-based sealers meet ISO recommendations, they are either less favorable or comparable to conventional resin-based sealers. However, calcium silicate-based sealers have consistently been reported to be biocompatible, non-cytotoxic, and non-genotoxic. They show good antimicrobial properties that are comparable to those of epoxy resin sealers. Above all, calcium silicate-based sealers are bioactive and stimulate hard tissue formation, which is the main advantage of this material.
Even though the biological properties of calcium silicate-based sealers are adequate, further investigations into ways of improving their physical properties are needed.
Go to :
 XML Download
XML Download