

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Root canal treatment failure comprises a variety of reasons and persistence of microorganisms in the root canal system even after shaping and cleaning is one of them [1]. The primary objective of the root canal therapy revolves around thorough debridement [2]. However, due to the complexity of the root canal system, shaping and cleaning procedure has become a challenging phase for the clinician. The disinfection of the entire root canal system relies on the ability of chemical irrigants in the root canal system [3]. Smear layer forms on the inner root canal wall when it is in contact with the instruments and during filing motion. It comprises 2 parts, the thick superficial layer on the surface of root canal wall (approximately 1 to 2 μm) and a deeper layer (up to 40 μm) into the dentinal tubules which contain organic and inorganic tissues including microorganisms and necrotic debris [4567]. The smear layer interrupts the penetration of root canal irrigants and acts as a barrier between the root filling and the canal wall, which is a potential path of leakage for bacteria contamination between the 2 surfaces [489]. It has been known that removal of the smear layer is essential to achieve thorough disinfection and 3-dimensional filling of the root canal system, thereby affecting the outcome of the endodontic procedure [101112].
Various types of root canal irrigants such as sodium hypochlorite (NaOCl) [11], chlorhexidine (CHX) [12], and mixture of tetracycline isonomer, an acid and a detergent (MTAD) [13] have been used based on their tissue dissolving and antimicrobial properties, whereas 17% ethylenediaminetetraacetic acid (EDTA) [14] and citric acid [15] have been advocated to remove the smear layer. Thus far, it has yet to be found a single irrigant that is able to fulfill the objectives of root canal irrigation that dissolves the organic and inorganic components in the canal, disruption of biofilms, neutralization of endotoxins and eliminating smear layer [1617181920]. Amongst all the materials, the combination of NaOCl and 17% EDTA has been the preferred choice to remove both organic and inorganic parts of the smear layer in the root canal system [2122].
As an alternative to the recommended irrigation protocol (NaOCl + 17% EDTA as final irrigant), QMix was introduced for the dual effect of smear layer removal [18]. This consists of polyaminocarboxylic acid chelating agent, bisbiguanide antimicrobial agent (2% CHX), surfactant and deionized water. QMix has shown to have higher antimicrobial property against Enterococcus faecalis as compared to CHX and found similar to EDTA in removing the smear layer [2324]. Many studies have compared the effectiveness of QMix in smear layer removal with other irrigants and have shown varying results. Some studies have shown that QMix removes smear layer more effectively than other irrigants whereas some results were contradictory. Thirteen studies have claimed that higher effectiveness was affected by the duration of QMix irrigation [23242526272829303132333435].
Due to the lack of standardization of methodology in in vitro studies, such investigations can only be appraised individually. To the best of the authors' knowledge, no systematic review has been done to evaluate the effectiveness of QMix compared to other irrigants in removing the smear layer in a human root canal system, although a number of in vitro studies had been published. Therefore, the aim of this systematic review was to compare the smear layer removal efficacy of QMix with other commonly employed root canal irrigants.
Go to : 
MATERIALS AND METHODS
Review question
The Population, Intervention, Comparison, Outcome and Study design framework was employed to develop the research question: In the extracted permanent human teeth with smear layer (P), does QMix irrigant (I) show better smear layer removal ability (O) compared to the other irrigants (C) from in vitro studies (S).
Search strategy
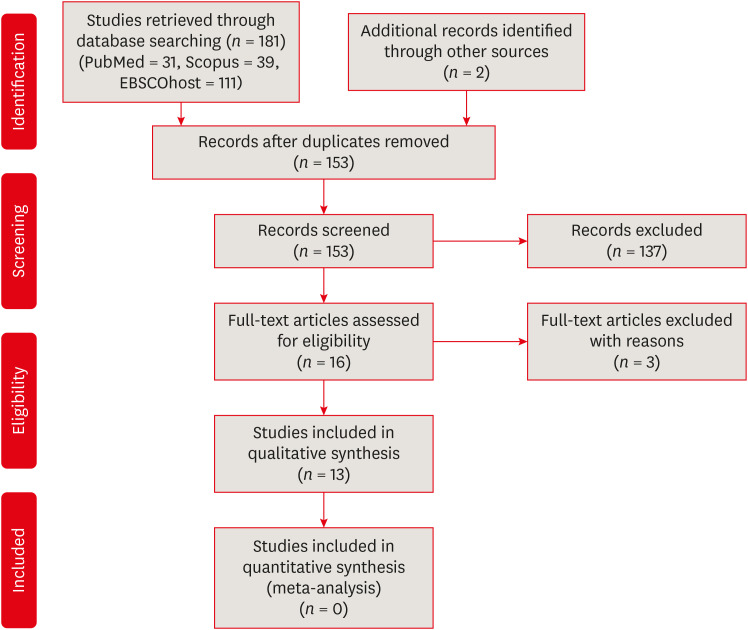
Literature search was performed comprehensively using 3 electronic databases including PubMed, Scopus, and EBSCOhost (Dentistry; Oral Sciences Source) was used for literature search to identify relevant articles: using the search strategy ((QMix) AND smear layer) AND ((root canal or endod)). Articles published from inception to October 2019 was included in this search. Reference list of the eligible studies and the journals publishing content relevant to the topic including Journal of Endodontics, International Endodontic Journal, Journal of Dentistry, Australian Endodontic Journal and Journal of Conservative Dentistry were hand-searched to identify any relevant studies. A flow chart of the search strategy was presented in Figure 1.
Inclusion criteria
Inclusion criteria for the selection of articles in this review were; 1) studies published in English, 2) studies performed in the extracted permanent human teeth, 3) studies that compared the smear layer removal ability of QMix with at least one irrigant, and 4) studies that tested the smear layer removal efficacy using scanning electronic microscopy (SEM), polarized light microscopy, and SEM-energy dispersive X-ray spectrometry.
Study selection and data extraction process
Firstly, the title and abstract of the selected articles were screened by 2 reviewers (MC, AP) based on the specified inclusion and exclusion criteria. Secondly, the reviewers independently read the articles and extracted the data using the data extraction form based on the items exclusive to this study. The following details were included in the data extraction form: author/s, year of publishing, country of the corresponding author, the total number of samples, type of teeth, interventions, evaluation method, results, irrigation regime including volume and duration, and scoring system. Any disagreement between the 2 reviewers in the selection of articles and the extraction of data was resolved in consultation with a third reviewer (JJ).
Quality assessment of the included articles
The quality of articles included in this review was assessed using revised Cochrane Risk of Bias tool (RoB 2.0). This tool was specifically modified to incorporate the contents relevant to the methodology of the included in vitro studies. Based on this, the quality of the studies was assessed on the following domains: randomization process, standardization of canal length, protocol for canal size enlargement, protocol for irrigating regimen (volume and duration) and bias in measurement outcome. The quality appraisal was independently performed by 2 authors (AP, MC) based on the above domains. In case of disagreement, a consensus was reached in discussion with a third reviewer (JJ).
Go to :
RESULTS
Study selection process
A total of 181 studies were identified from 3 electronic bases. 2 studies were retrieved through additional hand searching. After excluding studies based on title and abstract screening, 16 articles were available for full-text assessment. On careful reading, further 3 studies were excluded due to the following reasons: study done on bovine teeth [36], study that evaluated the effect of smear layer in infected dentinal tubules [8] and study that tested the bond strength of glass fiber post [37]. Finally, 13 papers were included in this systematic review. The search process employed to identify included studies was shown in Figure 1. Meta-analysis was not performed due to the presence of heterogeneity in the methodology and reporting outcomes of the included studies.
Eleven studies compared QMix to various irrigants like EDTA [2324252627282930313335], 4 studies on MTAD [23313435], 5 studies on NaOCl [2327282933], 2 studies on 7% EDTA (SmearClear) [3032], 10% citric acid [2933], one study on chitosan [32], glyde [32], 1% peracetic acid [33], Tubulicid Plus [34] and 7% maleic acid [28]. The effectiveness of smear layer removal was measured by different scoring systems. Four studies used Hülsmann et al. scoring system [25263035], 2 studies used Takeda et al. system [2729], 3 studies used Torabinejad et al. scoring system [283134] and others included Gishi et al. scoring system [33], Dai et al. scoring system [23] and Rome et al. scoring system [32] respectively. One study did not mention the scoring system and adhered to counting the number of open and closed tubules using imaging software, Adobe Photoshop CS3 [24].
Characteristics of included studies
Out of 13 studies, 4 studies included single-rooted teeth [23242532] and 5 studies specifically mentioned the type of single-rooted teeth. 2 studies utilized maxillary anterior teeth or incisors [2835], one study included canine [30], one used central incisors [27] and mandibular incisors [33] respectively. 4 studies included single-rooted mandibular premolar [26293134]. The apical instrumentation size and taper contribute to the efficacy of smear layer removal [3839]. The final instrumentation size, taper, standardized length of canal and system used for canal preparation varied among the included studies. It was found that 3 studies prepared canal length at 17 mm [232730] while other studies prepared the canal at 15 mm [252835], 14 mm [3134], 13 mm [26] and 16 mm [33] respectively. Three studies did not mention the standardized canal length in their studies [242932]. One study employed a combination of passive step-back and rotary 0.06 taper nickel-titanium files [32] and one did not mention the canal preparation system in their study [24]. Apical size of root canal in one study was reported as ISO #25 [26], 6 studies enlarged up to ISO #30 [272829313234], 3 studies enlarged up to the ISO #40 [253335] and 2 studies enlarged up to the ISO #50 [2330]. One study was done on dentin disc; hence no apical enlargement was mentioned in the study.
Four studies showed the effectiveness of QMix in smear layer removal was comparable to EDTA [23242830], while 3 studies showed QMix was more effective in removing the smear layer as compared to EDTA [252735]. Only 4 studies showed 17% EDTA was better than QMix in smear layer removal [26293132]. QMix was found to be more effective when used for 3 minutes as compared to 1 minute [26]. Comparing with other materials, one study showed QMix was more effective than MTAD [31] while another study showed QMix has smear layer removal ability similar to MTAD [35] and SmearClear [30]. 2 studies showed QMix was more effective than NaOCl [2933], Tubulicid Plus [34] and phytic acid [26]. One study showed QMix less effective as compared to 7% maleic acid [27] and 10% citric acid [28]. QMix and 1% peracetic acid remove the smear layer without alterations in inorganic structures, while 10% citric acid and 17% EDTA remove the smear layer with loss of structure (Table 1) [33].
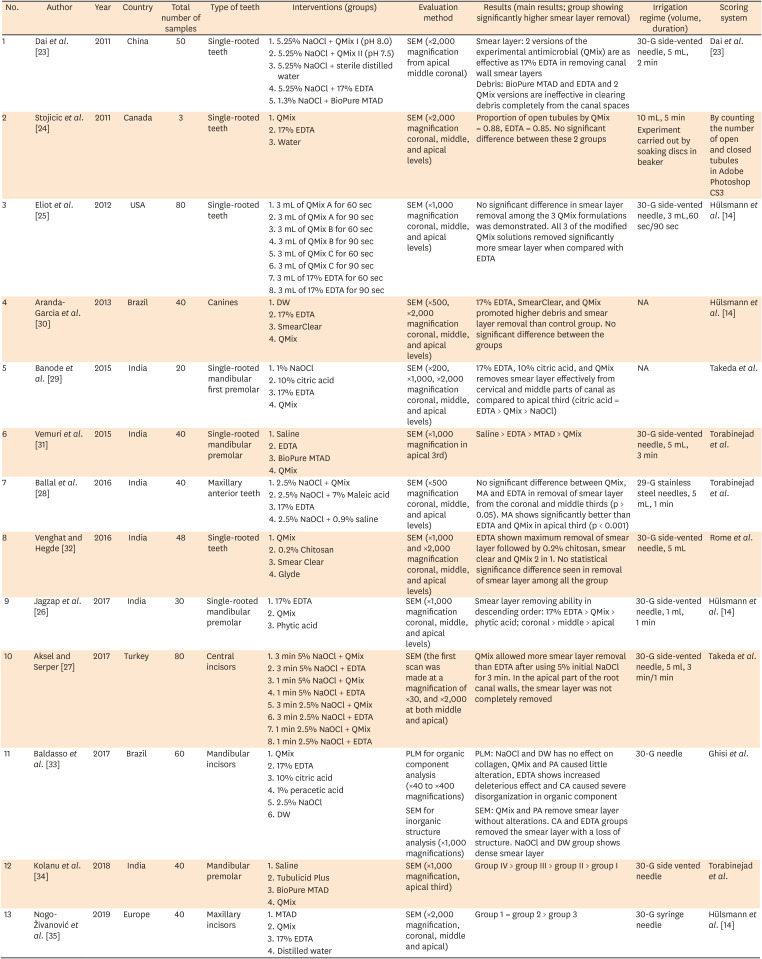
Table 1
Characteristics of included studies in the systematic review
| No. | Author | Year | Country | Total number of samples | Type of teeth | Interventions (groups) | Evaluation method | Results (main results; group showing significantly higher smear layer removal) | Irrigation regime (volume, duration) | Scoring system |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Dai et al. [23] | 2011 | China | 50 | Single-rooted teeth | 1. 5.25% NaOCl + QMix I (pH 8.0) | SEM (×2,000 magnification from apical middle coronal) | Smear layer: 2 versions of the experimental antimicrobial (QMix) are as effective as 17% EDTA in removing canal wall smear layers | 30-G side-vented needle, 5 mL, 2 min | Dai et al. [23] |
| 2. 5.25% NaOCl + QMix II (pH 7.5) | Debris: BioPure MTAD and EDTA and 2 QMix versions are ineffective in clearing debris completely from the canal spaces | |||||||||
| 3. 5.25% NaOCl + sterile distilled water | ||||||||||
| 4. 5.25% NaOCl + 17% EDTA | ||||||||||
| 5. 1.3% NaOCl + BioPure MTAD | ||||||||||
| 2 | Stojicic et al. [24] | 2011 | Canada | 3 | Single-rooted teeth | 1. QMix | SEM (×2,000 magnification coronal, middle, and apical levels) | Proportion of open tubules by QMix = 0.88, EDTA = 0.85. No significant difference between these 2 groups | 10 mL, 5 min | By counting the number of open and closed tubules in Adobe Photoshop CS3 |
| 2. 17% EDTA | Experiment carried out by soaking discs in beaker | |||||||||
| 3. Water | ||||||||||
| 3 | Eliot et al. [25] | 2012 | USA | 80 | Single-rooted teeth | 1. 3 mL of QMix A for 60 sec | SEM (×1,000 magnification coronal, middle, and apical levels) | No significant difference in smear layer removal among the 3 QMix formulations was demonstrated. All 3 of the modified QMix solutions removed significantly more smear layer when compared with EDTA | 30-G side-vented needle, 3 mL,60 sec/90 sec | Hülsmann et al. [14] |
| 2. 3 mL of QMix A for 90 sec | ||||||||||
| 3. 3 mL of QMix B for 60 sec | ||||||||||
| 4. 3 mL of QMix B for 90 sec | ||||||||||
| 5. 3 mL of QMix C for 60 sec | ||||||||||
| 6. 3 mL of QMix C for 90 sec | ||||||||||
| 7. 3 mL of 17% EDTA for 60 sec | ||||||||||
| 8. 3 mL of 17% EDTA for 90 sec | ||||||||||
| 4 | Aranda-Garcia et al. [30] | 2013 | Brazil | 40 | Canines | 1. DW | SEM (×500, ×2,000 magnification coronal, middle, and apical levels) | 17% EDTA, SmearClear, and QMix promoted higher debris and smear layer removal than control group. No significant difference between the groups | NA | Hülsmann et al. [14] |
| 2. 17% EDTA | ||||||||||
| 3. SmearClear | ||||||||||
| 4. QMix | ||||||||||
| 5 | Banode et al. [29] | 2015 | India | 20 | Single-rooted mandibular first premolar | 1. 1% NaOCl | SEM (×200, ×1,000, ×2,000 magnification coronal, middle, and apical levels) | 17% EDTA, 10% citric acid, and QMix removes smear layer effectively from cervical and middle parts of canal as compared to apical third (citric acid = EDTA > QMix > NaOCl) | NA | Takeda et al. |
| 2. 10% citric acid | ||||||||||
| 3. 17% EDTA | ||||||||||
| 4. QMix | ||||||||||
| 6 | Vemuri et al. [31] | 2015 | India | 40 | Single-rooted mandibular premolar | 1. Saline | SEM (×1,000 magnification in apical 3rd) | Saline > EDTA > MTAD > QMix | 30-G side-vented needle, 5 mL, 3 min | Torabinejad et al. |
| 2. EDTA | ||||||||||
| 3. BioPure MTAD | ||||||||||
| 4. QMix | ||||||||||
| 7 | Ballal et al. [28] | 2016 | India | 40 | Maxillary anterior teeth | 1. 2.5% NaOCl + QMix | SEM (×500 magnification coronal, middle, and apical levels) | No significant difference between QMix, MA and EDTA in removal of smear layer from the coronal and middle thirds (p > 0.05). MA shows significantly better than EDTA and QMix in apical third (p < 0.001) | 29-G stainless steel needles, 5 mL, 1 min | Torabinejad et al. |
| 2. 2.5% NaOCl + 7% Maleic acid | ||||||||||
| 3. 17% EDTA | ||||||||||
| 4. 2.5% NaOCl + 0.9% saline | ||||||||||
| 8 | Venghat and Hegde [32] | 2016 | India | 48 | Single-rooted teeth | 1. QMix | SEM (×1,000 and ×2,000 magnification coronal, middle, and apical levels) | EDTA shown maximum removal of smear layer followed by 0.2% chitosan, smear clear and QMix 2 in 1. No statistical significance difference seen in removal of smear layer among all the group | 30-G side-vented needle, 5 mL | Rome et al. |
| 2. 0.2% Chitosan | ||||||||||
| 3. Smear Clear | ||||||||||
| 4. Glyde | ||||||||||
| 9 | Jagzap et al. [26] | 2017 | India | 30 | Single-rooted mandibular premolar | 1. 17% EDTA | SEM (×1,000 magnification coronal, middle, and apical levels) | Smear layer removing ability in descending order: 17% EDTA > QMix > phytic acid; coronal > middle > apical | 30-G side-vented needle, 1 ml, 1 min | Hülsmann et al. [14] |
| 2. QMix | ||||||||||
| 3. Phytic acid | ||||||||||
| 10 | Aksel and Serper [27] | 2017 | Turkey | 80 | Central incisors | 1. 3 min 5% NaOCl + QMix | SEM (the first scan was made at a magnification of ×30, and ×2,000 at both middle and apical) | QMix allowed more smear layer removal than EDTA after using 5% initial NaOCl for 3 min. In the apical part of the root canal walls, the smear layer was not completely removed | 30-G side-vented needle, 5 ml, 3 min/1 min | Takeda et al. |
| 2. 3 min 5% NaOCl + EDTA | ||||||||||
| 3. 1 min 5% NaOCl + QMix | ||||||||||
| 4. 1 min 5% NaOCl + EDTA | ||||||||||
| 5. 3 min 2.5% NaOCl + QMix | ||||||||||
| 6. 3 min 2.5% NaOCl + EDTA | ||||||||||
| 7. 1 min 2.5% NaOCl + QMix | ||||||||||
| 8. 1 min 2.5% NaOCl + EDTA | ||||||||||
| 11 | Baldasso et al. [33] | 2017 | Brazil | 60 | Mandibular incisors | 1. QMix | PLM for organic component analysis (×40 to ×400 magnifications) | PLM: NaOCl and DW has no effect on collagen, QMix and PA caused little alteration, EDTA shows increased deleterious effect and CA caused severe disorganization in organic component | 30-G needle | Ghisi et al. |
| 2. 17% EDTA | SEM for inorganic structure analysis (×1,000 magnifications) | SEM: QMix and PA remove smear layer without alterations. CA and EDTA groups removed the smear layer with a loss of structure. NaOCl and DW group shows dense smear layer | ||||||||
| 3. 10% citric acid | ||||||||||
| 4. 1% peracetic acid | ||||||||||
| 5. 2.5% NaOCl | ||||||||||
| 6. DW | ||||||||||
| 12 | Kolanu et al. [34] | 2018 | India | 40 | Mandibular premolar | 1. Saline | SEM (×1,000 magnification, apical third) | Group IV > group III > group II > group I | 30-G side vented needle | Torabinejad et al. |
| 2. Tubulicid Plus | ||||||||||
| 3. BioPure MTAD | ||||||||||
| 4. QMix | ||||||||||
| 13 | Nogo-Živanović et al. [35] | 2019 | Europe | 40 | Maxillary incisors | 1. MTAD | SEM (×2,000 magnification, coronal, middle and apical) | Group 1 = group 2 > group 3 | 30-G syringe needle | Hülsmann et al. [14] |
| 2. QMix | ||||||||||
| 3. 17% EDTA | ||||||||||
| 4. Distilled water |
NA, not available; G, gauge; SEM, scanning electron microscope; DW, distilled water; NaOCl, sodium hypochlorite; EDTA, ethylenediaminetetraacetic acid; MTAD, mixture of tetracycline isonomer, an acid and a detergent; CA, Citric acid; MA, maleic acid; CSI, conventional syringe irrigation; PLM, polarized light microscopy.
![]()
Quality of included studies
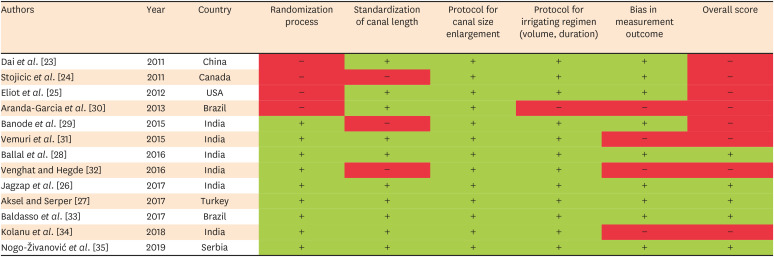
The studies were analyzed using the modified Risk of Bias tool and the overall quality of the included studies was found to be “moderate” (Figure 2). Most of the studies followed the randomization process [2628293132333435] and all studies stated the protocol for canal size enlargement, respectively. Three studies did not mention the standardization of canal length [242932]. In the protocol for irrigating regimens, all studies reported information on the volume of irrigants and the duration of their use except one study [30]. Four studies reported bias in measurement outcomes [30313234].
Go to :
DISCUSSION
Root canal disinfection can be achieved by mechanical and chemical means and irrigation plays a crucial role [8]. Irrigants can reach areas with anatomical complexities including isthmus, ramifications, dentinal tubules of the root canal system, where instrumentation cannot reach thereby, facilitate a reduction of microbial biofilms [1112]. Various studies published on QMix comparing with other irrigants on its smear layer removal property [23242526272829303132333435], but the results were inconsistent. Although it would be more applicable if the effectiveness was tested using in vivo settings, no study has been conducted in this manner. Hence, to answer our research question, only in vitro studies were included in the systematic review.
To evaluate the risk of bias of the included studies, Revised Cochrane ROB has been modified based on the characteristics of the included in vitro studies. A total of 5 parameters (randomization process, standardization of canal length, protocol for canal size enlargement, protocol for irrigating regimen [volume, duration], and bias in measurement outcome) have been used to appraise the quality of included studies. The standardization of canal length varied among the published literature. Root canal length and depth of insertion of irrigation needle have an effect on the efficacy of irrigant to remove the debris from the canal [40], and cleaning of the apical third of the canal has always been challenging compared to coronal and middle third [41]. This can be due to the formation of the vapor lock phenomenon at the apical third, as the root is a closed-ended channel being surrounded by periodontium [424344]. Hence, the importance of the depth of irrigation needle should be at the working length to irrigate the apical third of the canal, which can be implemented in a clinical setting [45]. Moreover, when activation and agitation were added on QMix, it enhanced its smear layer removal ability and showed a significant difference compared to QMix without agitation [4647484950515253].
It has been shown that the protocol for canal size preparation plays a crucial role in the removal of debris in the root canal. There was a significant difference in larger canal preparation which enabled a more effective removal of smear layer than a smaller sized canal [5455]. It was reported from a study that an increase in the size of ISO #35 to ISO #40 has a significant increase in mean irrigant volume, which was at 44% of the root canal system. It was proposed to enlarge the apical third to ISO #40 with a 0.04 taper to allow a maximum volume of irrigation at the apical third and tooth structure preservation [56]. Hence, the different protocol of canal preparation implied in respective studies has a significant impact on smear layer removal ability. In addition, few studies have shown that the duration of irrigation with QMix affects the smear layer removal effectiveness. This was apparent in this review as QMix showed better effect when used for a longer time (3 minutes) as compared to 1 minute [26].
Substantial differences in the method of scoring were observed in the studies included in this review. The use of different scoring systems can result in variations in the level of scoring based on the definition of each scoring criterion. For example, Torabinejad et al. scoring system consists of 3 scores (score 1: no smear layer; score 2: moderate smear layer; score 3: heavy smear layer) [283134]. In contrast, Hülsmann et al. scoring system has scores 1 to 5 [25263035], which is similar to Takeda et al. [2729] that consists of scores 1 to 4. The additional score in Hülsmann et al. [14] is score 4, corresponding to the complete root canal wall covered by a homogenous smear layer, with no open dentinal tubules. It is hard to interpret the gold standard scoring system and no evidence was found to make this recommendation. It is our view that a scoring system with more level of scores is precise and consequently provides accurate analysis of the presence of the smear layer. However, this may compromise the reliability of scoring. Considering the accuracy and reliability, Hülsmann et al. [14] scoring system can be considered more superior to other scoring systems used in the included studies.
Different endodontic file systems produce different amounts of debris within the root canal system [5758]. However, it is to be noted that studies have reported no significant difference in debris and smear layer formation in the root canal system prepared by ProTaper and MTwo rotary system [5960] and between ProTaper, K3 nickel-titanium and MTwo rotary system [41]. Therefore, it can be inferred that the rotary system does not have a huge impact on the evaluation of smear layer removal of irrigants despite various endodontic file systems employed in the included studies.
All the included in vitro studies performed in human teeth and smear layer was produced by using actual endodontic file except for one study [24] which uses dentin disc and formation of smear layer by drilling with long neck burs. One of the limitations of this review was a lack of homogeneity in the study design of the included studies. For example, different scoring systems were used to score the presence of smear layer. This would have led to inaccurate scoring and a possible obstacle to comparing the outcome between the studies. SEM analysis has been used to evaluate the number of blocked canals by the smear layer. Seven studies used ×2,000 magnification [23242729303235] whilst 5 studies only used ×1,000 magnification [2526313334] and one study used ×500 magnification [28]. Higher magnification influences the accuracy in evaluating the dentinal tubules blocked by the smear layer. Hence, SEM analysis using lower magnification might have impacted the results. Also, it was also found that one study included only 3 teeth as a sample size, which would have contributed to biased results [24].
It is recommended for future in vitro studies to use Hülsmann et al. [14] scoring system to evaluate dentinal tubules blocked by smear layer and SEM analysis with higher magnification as it is more accurate. To simulate the closed environment of the root canal which is surrounded by periodontium, it is recommended to close the apex of the tooth with wax, which provides an environment almost similar in the clinical setting.
Go to :
CONCLUSIONS
This systematic review showed better smear layer removal using QMix compared to MTAD, NaOCl, Tubulicid Plus, and Phytic acid. However, it was less effective than 7% maleic acid and 10% citric acid. There was no conclusive result between QMix and 17% EDTA due to conflicting results. To improve smear layer removal efficacy of QMix, it is recommended to use it for a longer duration.
Go to :
 XML Download
XML Download