

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The main aim of endodontic treatment is to retain teeth affected by pulpal or periradicular diseases. Root canal infection is the main etiologic factor of apical periodontitis [1] and endodontic failure [2]. Thus, successful endodontic therapy depends on their elimination or reduction [23].
Since mechanical instrumentation and irrigation cannot completely eliminate microbiota, the use of intracanal medications (ICM) with antimicrobial properties has been recommended [45]. Calcium hydroxide (CH) has been considered as the most favorable antimicrobial agent [4678], which can also have anti-inflammatory and pain-preventive properties [49101112].
Despite the extensive endodontic literature about CH from in vitro and animal studies [1314], studies that assessed its pain and flare-up effects are few with a lack of pooled effect-size estimates [1516]. A systematic review is thus, needed to provide a quantitative pooled estimate relative to the effectiveness of CH in comparison to no or other ICMs. The aim of this study, thus, was to systematically review and provide a pooled effect size estimate, if possible, for postoperative pain and flare-up incidence of CH on the endodontic treatment of non-vital teeth with or without apical periodontitis.
MATERIALS AND METHODS
Protocol and registration
The protocol was registered in the PROSPERO database (registration number: CRD42016041953). This systematic review and meta-analysis were reported according to the preferred reporting items for systematic reviews and meta-analyses (PRISMA) statement [17].
Research question
The research question was: “In adult patients with mature permanent non-vital teeth, what is the effect of CH compared to no or other ICMs on postoperative pain, flare-up incidence, and swelling incidence?
Eligibility criteria
Randomized clinical trials (RCTs) that fulfilled the following criteria were included: Studies of adult patients with non-vital mature permanent teeth treated in multiple visits where CH mixed with inert vehicles is compared to no or other ICMs regarding postoperative pain (binary [yes/no] or continuous), flare-up (binary [yes/no]) and/or swelling incidence. No restrictions were set on publication dates or language.
Information sources and search strategy
The following electronic databases were searched from inception to September 2019: Cochrane Central Register of Controlled Trials (CENTRAL), MEDLINE via PubMed, Latin American and Caribbean Health Sciences Literature (LILACS), ISI Web of Science, Trip database, EBSCOhost, Scopus database, and Google Scholar; Open grey, ProQuest dissertation, and thesis database were searched to capture the ‘grey literature’. Clinical trial registries were searched including clinicaltrials.gov and World Health Organization trials register. Searching citations, reference lists of included studies and related systematic reviews, as well as manual search for major journals in endodontics and dentistry, were also done. Two independent reviewers conducted the search using free-text terms and controlled vocabulary where the search strategy was first developed in PubMed (Supplementary Table 1) and adapted for other electronic databases.
Study selection and identification
Two independent reviewers screened the search results by title and abstract, then by full-text assessment to determine the included studies. Studies were selected based on the pre-specified eligibility criteria. The full-text assessment was done for the potentially-relevant studies and those with insufficient data in the title and abstract to confirm their eligibility. Any disagreements in the selection process were resolved by discussion to reach a consensus, and when needed, the opinion of the third reviewer was considered.
Data extraction
Data were extracted in a customized structured data-extraction form, and the following items were included: study design, number of arms, randomization, selection criteria, tooth type, diagnostic criteria, gender/age, number randomized/analyzed, cleaning and shaping technique, ICMs evaluated, outcome(s) and main findings. Data extraction was done by 2 independent reviewers and any disagreements were resolved by discussion to reach a consensus or consulting a third reviewer.
Risk-of-bias assessment
Two independent reviewers used the individually-randomized-parallel-group-trials template of the revised Cochrane risk of bias tool for randomized trials (RoB 2.0) [18]. Risk of bias assessment was done on the outcome level in each study. The following domains were assessed: bias arising from randomization process, bias due to deviation from the intended interventions, bias due to missing outcome data, bias in the measurement of the outcome, and bias in the selection of the reported results. Risk of bias was judged in each domain as “low risk”, “high risk” or showing “some concerns”. A judgment of “high risk” in at least one domain or the judgment of “some concerns” in multiple domains would result in overall high risk of bias in the assessed outcome. A judgment of “some concerns” in at least one domain would result in overall some concerns of bias in the assessed outcome. Judgments of “low risk” in all domains would result in overall low risk of bias in the assessed outcome. Any disagreements among the 2 independent reviewers were resolved by discussion and, when needed, consulting a third reviewer. Authors of included studies were contacted via e-mail in case of needing more information or clarification to facilitate judgment.
Quantitative data analysis
Risk ratio (RR) was used as an effective measure for the dichotomous outcomes. Mean difference (MD) and standardized mean difference (SMD) were used as effect measures for the continuous outcomes. Categorical data measured using ordinal scales were dichotomized for postoperative pain incidence (Supplementary Table 2). Included studies that assessed postoperative pain at multiple time points had their data transformed to fit the following intervals: ≤ 1 day, > 1-day-till-3-days, and > 3-till-14-days where data at the longest time point within the interval was selected from each study. The definition of ‘flare-up’ varied across studies (Supplementary Table 3). Swelling incidence was defined as by the trials' authors. Studies with an arm having a corticosteroid/antibiotic combination (CS/AB) were pooled in the same meta-analysis regardless of the type of corticosteroid or antibiotic. Data of non-vital teeth only were used from studies reporting data of vital and non-vital teeth separately.
Meta-analysis for studies with the same comparison, outcome measure, and time interval were conducted using the fixed-effect model in RevMan software 5.3 (Cochrane Collaboration, Copenhagen, Denmark). Heterogeneity was assessed using the Cochrane's test and quantified by I-square test (I2). In the case of substantial heterogeneity (I2 > 50% and p value < 0.1), sensitivity analysis using the random-effect model was conducted. Single tooth was the unit-of-analysis. Studies with the number of teeth exceeding the number of patients, without stating if the patients were randomized an equal number of times as the teeth, were considered as having a unit-of-analysis issue (UOA) and bias in allocation [19]. If studies per comparison were less than 10, subgroup and publication bias analyses were precluded. The level of certainty of the evidence was assessed according to the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) working group guidelines.
RESULTS
Search and Study selection
A total of 5,012 articles were identified after searching for electronic sources and 25 articles were identified through searching for other sources. After removal of duplicates, 3,920 articles were identified (Figure 1). After screening with title and abstract, 3,878 articles were considered irrelevant and 42 articles were assessed for full-text eligibility. Twenty-six articles were excluded for different reasons (Supplementary Table 4). Sixteen articles from 15 studies [451011122021222324252627282930] were included in the qualitative analysis (Tables 1 and 2).
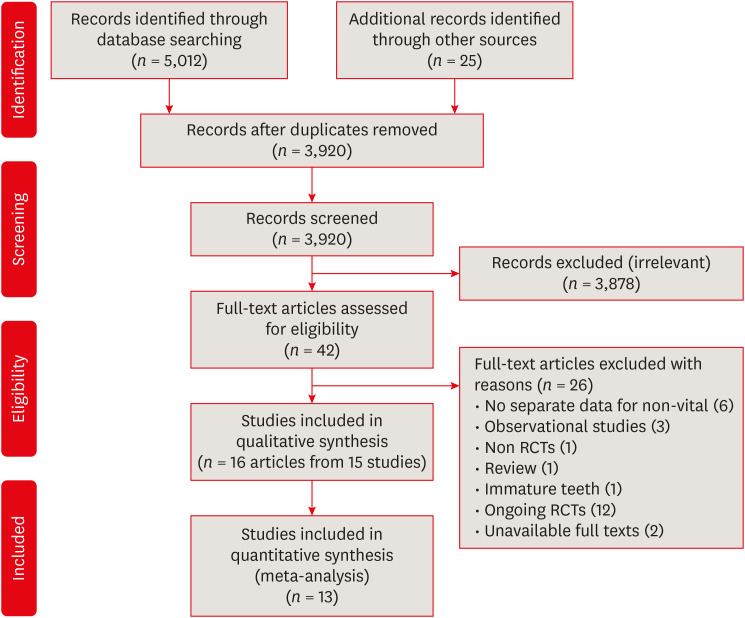
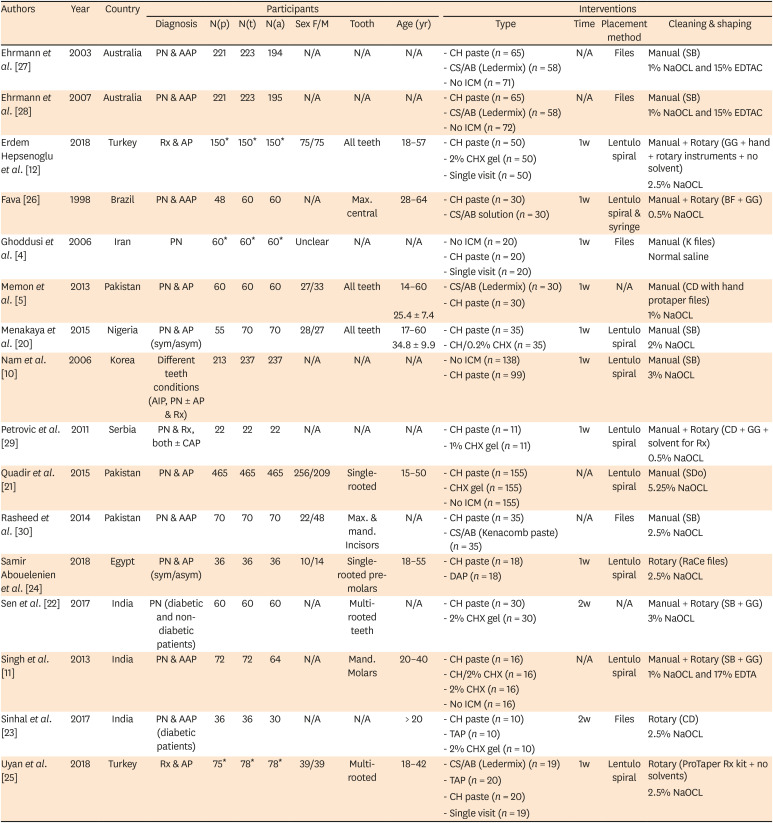
Table 1
Characteristics of included studies: study, participant and interventions' characteristics
| Authors | Year | Country | Participants | Interventions | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Diagnosis | N(p) | N(t) | N(a) | Sex F/M | Tooth | Age (yr) | Type | Time | Placement method | Cleaning & shaping | |||
| Ehrmann et al. [27] | 2003 | Australia | PN & AAP | 221 | 223 | 194 | N/A | N/A | N/A | - CH paste (n = 65) | N/A | Files | Manual (SB) |
| - CS/AB (Ledermix) (n = 58) | 1% NaOCL and 15% EDTAC | ||||||||||||
| - No ICM (n = 71) | |||||||||||||
| Ehrmann et al. [28] | 2007 | Australia | PN & AAP | 221 | 223 | 195 | N/A | N/A | N/A | - CH paste (n = 65) | N/A | Files | Manual (SB) |
| - CS/AB (Ledermix) (n = 58) | 1% NaOCL and 15% EDTAC | ||||||||||||
| - No ICM (n = 72) | |||||||||||||
| Erdem Hepsenoglu et al. [12] | 2018 | Turkey | Rx & AP | 150* | 150* | 150* | 75/75 | All teeth | 18–57 | - CH paste (n = 50) | 1w | Lentulo spiral | Manual + Rotary (GG + hand + rotary instruments + no solvent) |
| - 2% CHX gel (n = 50) | 2.5% NaOCL | ||||||||||||
| - Single visit (n = 50) | |||||||||||||
| Fava [26] | 1998 | Brazil | PN & AAP | 48 | 60 | 60 | N/A | Max. central | 28–64 | - CH paste (n = 30) | 1w | Lentulo spiral & syringe | Manual + Rotary (BF + GG) |
| - CS/AB solution (n = 30) | 0.5% NaOCL | ||||||||||||
| Ghoddusi et al. [4] | 2006 | Iran | PN | 60* | 60* | 60* | Unclear | N/A | N/A | - No ICM (n = 20) | 1w | Files | Manual (K files) |
| - CH paste (n = 20) | Normal saline | ||||||||||||
| - Single visit (n = 20) | |||||||||||||
| Memon et al. [5] | 2013 | Pakistan | PN & AP | 60 | 60 | 60 | 27/33 | All teeth | 14–60 | - CS/AB (Ledermix) (n = 30) | 1w | N/A | Manual (CD with hand protaper files) |
| 25.4 ± 7.4 | - CH paste (n = 30) | 1% NaOCL | |||||||||||
| Menakaya et al. [20] | 2015 | Nigeria | PN & AP (sym/asym) | 55 | 70 | 70 | 28/27 | All teeth | 17–60 | - CH paste (n = 35) | 1w | Lentulo spiral | Manual (SB) |
| 34.8 ± 9.9 | - CH/0.2% CHX (n = 35) | 2% NaOCL | |||||||||||
| Nam et al. [10] | 2006 | Korea | Different teeth conditions (AIP, PN ± AP & Rx) | 213 | 237 | 237 | N/A | N/A | N/A | - No ICM (n = 138) | 1w | Lentulo spiral | Manual (SB) |
| - CH paste (n = 99) | 3% NaOCL | ||||||||||||
| Petrovic et al. [29] | 2011 | Serbia | PN & Rx, both ± CAP | 22 | 22 | 22 | N/A | N/A | N/A | - CH paste (n = 11) | 1w | Lentulo spiral | Manual + Rotary (CD + GG + solvent for Rx) |
| - 1% CHX gel (n = 11) | 0.5% NaOCL | ||||||||||||
| Quadir et al. [21] | 2015 | Pakistan | PN & AP | 465 | 465 | 465 | 256/209 | Single-rooted | 15–50 | - CH paste (n = 155) | N/A | Lentulo spiral | Manual (SDo) |
| - CHX gel (n = 155) | 5.25% NaOCL | ||||||||||||
| - No ICM (n = 155) | |||||||||||||
| Rasheed et al. [30] | 2014 | Pakistan | PN & AAP | 70 | 70 | 70 | 22/48 | Max. & mand. Incisors | N/A | - CH paste (n = 35) | N/A | Files | Manual (SB) |
| - CS/AB (Kenacomb paste) (n = 35) | 2.5% NaOCL | ||||||||||||
| Samir Abouelenien et al. [24] | 2018 | Egypt | PN & AP (sym/asym) | 36 | 36 | 36 | 10/14 | Single-rooted pre-molars | 18–55 | - CH paste (n = 18) | 1w | Lentulo spiral | Rotary (RaCe files) |
| - DAP (n = 18) | 2.5% NaOCL | ||||||||||||
| Sen et al. [22] | 2017 | India | PN (diabetic and non-diabetic patients) | 60 | 60 | 60 | N/A | Multi-rooted teeth | N/A | - CH paste (n = 30) | 2w | N/A | Manual + Rotary (SB + GG) |
| - 2% CHX gel (n = 30) | 3% NaOCL | ||||||||||||
| Singh et al. [11] | 2013 | India | PN & AAP | 72 | 72 | 64 | N/A | Mand. Molars | 20–40 | - CH paste (n = 16) | N/A | Lentulo spiral | Manual + Rotary (SB + GG) |
| - CH/2% CHX (n = 16) | 1% NaOCL and 17% EDTA | ||||||||||||
| - 2% CHX (n = 16) | |||||||||||||
| - No ICM (n = 16) | |||||||||||||
| Sinhal et al. [23] | 2017 | India | PN & AAP (diabetic patients) | 36 | 36 | 30 | N/A | N/A | > 20 | - CH paste (n = 10) | 2w | Files | Rotary (CD) |
| - TAP (n = 10) | 2.5% NaOCL | ||||||||||||
| - 2% CHX gel (n = 10) | |||||||||||||
| Uyan et al. [25] | 2018 | Turkey | Rx & AP | 75* | 78* | 78* | 39/39 | Multi-rooted | 18–42 | - CS/AB (Ledermix) (n = 19) | 1w | Lentulo spiral | Rotary (ProTaper Rx kit + no solvents) |
| - TAP (n = 20) | 2.5% NaOCL | ||||||||||||
| - CH paste (n = 20) | |||||||||||||
| - Single visit (n = 19) | |||||||||||||
Age are presented as range or mean ± standard deviation.
AAP, acute apical periodontitis; AIP, acute irreversible pulpitis; AP, apical periodontitis; BF, balanced force technique; CAP, chronic apical periodontitis; CD, crown down; CH, calcium hydroxide; CHX, chlorhexidine; CS/AB, corticosteroid and antibiotic combination; DAP, double antibiotic paste; EDTA, ethylenediaminetetraacetic acid; EDTAC, ethylenediaminetetraacetic acid plus Cetavlon; F/M, female/male; ICM, intracanal medication; GG, gates-glidden drills; Mand., mandibular; Max., maxillary; NaOCl, sodium hypochlorite; N/A, not available; N(a), total number of teeth analysed; N(p), total number of participants included; N(t), total number of teeth randomized; PN, pulp necrosis; Rx, endodontic retreatment; SB, step-back technique; SDo, step-down technique; sym/asym, symptomatic and asymptomatic; TAP, triple antibiotic paste; w, week.
*Study has a group not within review scope.
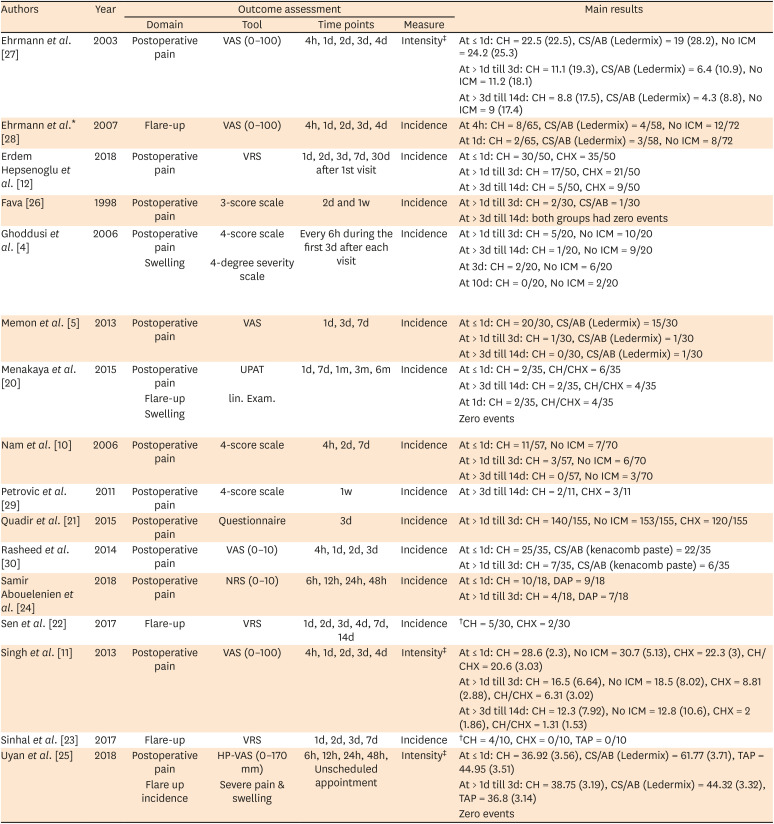
Table 2
Characteristics of included studies: outcome assessment and main results
| Authors | Year | Outcome assessment | Main results | |||
|---|---|---|---|---|---|---|
| Domain | Tool | Time points | Measure | |||
| Ehrmann et al. [27] | 2003 | Postoperative pain | VAS (0–100) | 4h, 1d, 2d, 3d, 4d | Intensity‡ | At ≤ 1d: CH = 22.5 (22.5), CS/AB (Ledermix) = 19 (28.2), No ICM = 24.2 (25.3) |
| At > 1d till 3d: CH = 11.1 (19.3), CS/AB (Ledermix) = 6.4 (10.9), No ICM = 11.2 (18.1) | ||||||
| At > 3d till 14d: CH = 8.8 (17.5), CS/AB (Ledermix) = 4.3 (8.8), No ICM = 9 (17.4) | ||||||
| Ehrmann et al.* [28] | 2007 | Flare-up | VAS (0–100) | 4h, 1d, 2d, 3d, 4d | Incidence | At 4h: CH = 8/65, CS/AB (Ledermix) = 4/58, No ICM = 12/72 |
| At 1d: CH = 2/65, CS/AB (Ledermix) = 3/58, No ICM = 8/72 | ||||||
| Erdem Hepsenoglu et al. [12] | 2018 | Postoperative pain | VRS | 1d, 2d, 3d, 7d, 30d after 1st visit | Incidence | At ≤ 1d: CH = 30/50, CHX = 35/50 |
| At > 1d till 3d: CH = 17/50, CHX = 21/50 | ||||||
| At > 3d till 14d: CH = 5/50, CHX = 9/50 | ||||||
| Fava [26] | 1998 | Postoperative pain | 3-score scale | 2d and 1w | Incidence | At > 1d till 3d: CH = 2/30, CS/AB = 1/30 |
| At > 3d till 14d: both groups had zero events | ||||||
| Ghoddusi et al. [4] | 2006 | Postoperative pain | 4-score scale | Every 6h during the first 3d after each visit | Incidence | At > 1d till 3d: CH = 5/20, No ICM = 10/20 |
| Swelling | 4-degree severity scale | At > 3d till 14d: CH = 1/20, No ICM = 9/20 | ||||
| At 3d: CH = 2/20, No ICM = 6/20 | ||||||
| At 10d: CH = 0/20, No ICM = 2/20 | ||||||
| Memon et al. [5] | 2013 | Postoperative pain | VAS | 1d, 3d, 7d | Incidence | At ≤ 1d: CH = 20/30, CS/AB (Ledermix) = 15/30 |
| At > 1d till 3d: CH = 1/30, CS/AB (Ledermix) = 1/30 | ||||||
| At > 3d till 14d: CH = 0/30, CS/AB (Ledermix) = 1/30 | ||||||
| Menakaya et al. [20] | 2015 | Postoperative pain | UPAT | 1d, 7d, 1m, 3m, 6m | Incidence | At ≤ 1d: CH = 2/35, CH/CHX = 6/35 |
| Flare-up | lin. Exam. | At > 3d till 14d: CH = 2/35, CH/CHX = 4/35 | ||||
| Swelling | At 1d: CH = 2/35, CH/CHX = 4/35 | |||||
| Zero events | ||||||
| Nam et al. [10] | 2006 | Postoperative pain | 4-score scale | 4h, 2d, 7d | Incidence | At ≤ 1d: CH = 11/57, No ICM = 7/70 |
| At > 1d till 3d: CH = 3/57, No ICM = 6/70 | ||||||
| At > 3d till 14d: CH = 0/57, No ICM = 3/70 | ||||||
| Petrovic et al. [29] | 2011 | Postoperative pain | 4-score scale | 1w | Incidence | At > 3d till 14d: CH = 2/11, CHX = 3/11 |
| Quadir et al. [21] | 2015 | Postoperative pain | Questionnaire | 3d | Incidence | At > 1d till 3d: CH = 140/155, No ICM = 153/155, CHX = 120/155 |
| Rasheed et al. [30] | 2014 | Postoperative pain | VAS (0–10) | 4h, 1d, 2d, 3d | Incidence | At ≤ 1d: CH = 25/35, CS/AB (kenacomb paste) = 22/35 |
| At > 1d till 3d: CH = 7/35, CS/AB (kenacomb paste) = 6/35 | ||||||
| Samir Abouelenien et al. [24] | 2018 | Postoperative pain | NRS (0–10) | 6h, 12h, 24h, 48h | Incidence | At ≤ 1d: CH = 10/18, DAP = 9/18 |
| At > 1d till 3d: CH = 4/18, DAP = 7/18 | ||||||
| Sen et al. [22] | 2017 | Flare-up | VRS | 1d, 2d, 3d, 4d, 7d, 14d | Incidence | †CH = 5/30, CHX = 2/30 |
| Singh et al. [11] | 2013 | Postoperative pain | VAS (0–100) | 4h, 1d, 2d, 3d, 4d | Intensity‡ | At ≤ 1d: CH = 28.6 (2.3), No ICM = 30.7 (5.13), CHX = 22.3 (3), CH/CHX = 20.6 (3.03) |
| At > 1d till 3d: CH = 16.5 (6.64), No ICM = 18.5 (8.02), CHX = 8.81 (2.88), CH/CHX = 6.31 (3.02) | ||||||
| At > 3d till 14d: CH = 12.3 (7.92), No ICM = 12.8 (10.6), CHX = 2 (1.86), CH/CHX = 1.31 (1.53) | ||||||
| Sinhal et al. [23] | 2017 | Flare-up | VRS | 1d, 2d, 3d, 7d | Incidence | †CH = 4/10, CHX = 0/10, TAP = 0/10 |
| Uyan et al. [25] | 2018 | Postoperative pain | HP-VAS (0–170 mm) | 6h, 12h, 24h, 48h, Unscheduled appointment | Intensity‡ | At ≤ 1d: CH = 36.92 (3.56), CS/AB (Ledermix) = 61.77 (3.71), TAP = 44.95 (3.51) |
| Flare up incidence | Severe pain & swelling | At > 1d till 3d: CH = 38.75 (3.19), CS/AB (Ledermix) = 44.32 (3.32), TAP = 36.8 (3.14) | ||||
| Zero events | ||||||
CH, calcium hydroxide; CHX, chlorhexidine; CS/AB, corticosteroid and antibiotic combination; d, day; DAP, double antibiotic paste; h, hour; HP-VAS, Heft-Parker visual analogue scale; ICM, intracanal medication; m, month; NRS, numerical rating scale; TAP, triple antibiotic paste; UPAT, Universal pain assessment tool; VAS, visual analogue scale, VRS, verbal rating scale; w, week.
*Author did not report results for all time points; †Author did not specify time points for this result; ‡Results presented as mean (standard deviation).
Characteristics of the included studies
The characteristics of the included studies are summarized in Tables 1 and 2. All the included studies were RCTs with parallel-arm or multi-arm design and published in English language except for one study in Korean [10]. A total of 1,643 participants with 1,699 teeth were enrolled in the included studies and a total of 1,657 teeth analyzed. One study was reported in two articles [2728]. Five studies in six articles had a UOA issue [102025262728]. However, one study has mentioned that the participants were randomized an equal number of times as that of the teeth included [20].
All types of teeth were included, whether anterior or posterior, single- or multi-rooted, and maxillary or mandibular. All included studies investigated teeth with primary endodontic infection except for four studies that included failed endodontically-treated teeth [10122529]. Participants included in all studies were systemically-healthy subjects except in 2 studies including diabetic subjects [2223].
The intervention of interest in the included studies was CH mixed with different inert vehicles including distilled water, sterile saline, glycerine, glycerol, or a commercially-available CH paste with an inert vehicle. ICMs were placed for a duration of 7 to 14 days. In the included studies, six different comparators were identified and they were: no ICM, chlorhexidine (CHX), CH/CHX, CS/AB (e.g. Ledermix paste, Kenacomb paste, a solution of corticosteroid and antibiotics), triple-antibiotic paste (TAP; metronidazole, ciprofloxacin and minocycline) and double-antibiotic paste (DAP; metronidazole, ciprofloxacin) (Table 1).
Risk of bias assessment
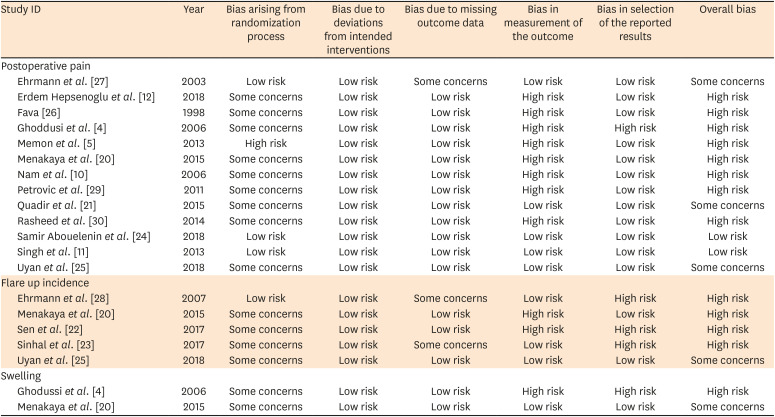
The summary of the risk of bias assessment is presented in Table 3. For the studies assessing postoperative pain, 8 of 13 studies [45101220262930] showed an overall high risk of bias, primarily due to a high risk of bias in outcome measurement. Three studies had ‘Some Concerns’ about bias [212527], and 2 had an overall low risk of bias [1124].
Table 3
Risk of bias assessment per outcome for the included studies
| Study ID | Year | Bias arising from randomization process | Bias due to deviations from intended interventions | Bias due to missing outcome data | Bias in measurement of the outcome | Bias in selection of the reported results | Overall bias | |
|---|---|---|---|---|---|---|---|---|
| Postoperative pain | ||||||||
| Ehrmann et al. [27] | 2003 | Low risk | Low risk | Some concerns | Low risk | Low risk | Some concerns | |
| Erdem Hepsenoglu et al. [12] | 2018 | Some concerns | Low risk | Low risk | High risk | Low risk | High risk | |
| Fava [26] | 1998 | Some concerns | Low risk | Low risk | High risk | Low risk | High risk | |
| Ghoddusi et al. [4] | 2006 | Some concerns | Low risk | Low risk | High risk | High risk | High risk | |
| Memon et al. [5] | 2013 | High risk | Low risk | Low risk | High risk | Low risk | High risk | |
| Menakaya et al. [20] | 2015 | Some concerns | Low risk | Low risk | High risk | Low risk | High risk | |
| Nam et al. [10] | 2006 | Some concerns | Low risk | Low risk | High risk | Low risk | High risk | |
| Petrovic et al. [29] | 2011 | Some concerns | Low risk | Low risk | High risk | Low risk | High risk | |
| Quadir et al. [21] | 2015 | Some concerns | Low risk | Low risk | Low risk | Low risk | Some concerns | |
| Rasheed et al. [30] | 2014 | Some concerns | Low risk | Low risk | High risk | Low risk | High risk | |
| Samir Abouelenin et al. [24] | 2018 | Low risk | Low risk | Low risk | Low risk | Low risk | Low risk | |
| Singh et al. [11] | 2013 | Low risk | Low risk | Low risk | Low risk | Low risk | Low risk | |
| Uyan et al. [25] | 2018 | Some concerns | Low risk | Low risk | Low risk | Low risk | Some concerns | |
| Flare up incidence | ||||||||
| Ehrmann et al. [28] | 2007 | Low risk | Low risk | Some concerns | Low risk | High risk | High risk | |
| Menakaya et al. [20] | 2015 | Some concerns | Low risk | Low risk | High risk | Low risk | High risk | |
| Sen et al. [22] | 2017 | Some concerns | Low risk | Low risk | High risk | High risk | High risk | |
| Sinhal et al. [23] | 2017 | Some concerns | Low risk | Some concerns | Low risk | High risk | High risk | |
| Uyan et al. [25] | 2018 | Some concerns | Low risk | Low risk | Low risk | Low risk | Some concerns | |
| Swelling | ||||||||
| Ghodussi et al. [4] | 2006 | Some concerns | Low risk | Low risk | High risk | High risk | High risk | |
| Menakaya et al. [20] | 2015 | Some concerns | Low risk | Low risk | Low risk | Low risk | Some concerns | |
Qualitative and quantitative synthesis
Of the 16 articles, thirteen, [451011122122232526272930] comprising a total of 1,289 teeth, were included in quantitative synthesis in three comparisons (CH versus each of no ICM, CHX and CS/AB) for postoperative pain (incidence and intensity) and flare-up incidence.
1. Postoperative pain
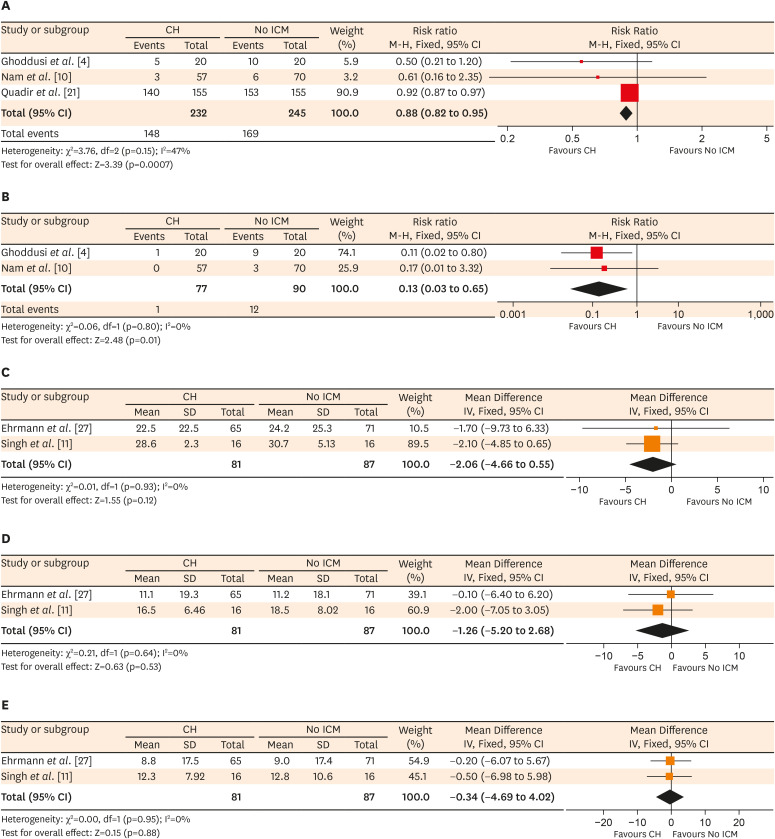
On comparing CH with no ICM, 3 studies assessed pain incidence [41021]. At the ≤ 1-day interval, there was no difference in pain risk (RR, 1.93; 95% CI, 0.80 to 4.66; 1 study, 127 teeth, High RoB) [10]; the certainty of evidence (CoE) is very low (Supplementary Table 5). At the > 1-day-till-3-days interval, CH decreased the risk of pain (RRpooled, 0.88; 95% CI, 0.82 to 0.95; I2 = 47%; 477 teeth, 3 studies, 1 ‘Some Concerns’ & 2 High RoB, Figure 2A) [41021]; the CoE is moderate (Supplementary Table 5). At the > 3-day-till-14-days interval, CH decreased pain risk (RRpooled, 0.13; 95% CI, 0.03 to 0.65; I2 = 0%; 167 teeth, 2 studies, 2 High RoB, Figure 2B) [410]; the CoE is low (Supplementary Table 5). 2 studies [1127] reported data for pain intensity. There was no difference in pain intensity at the ≤ 1-day interval (MDpooled, −2.06; 95% CI, −4.66 to 0.55; I2 = 0%; 168 teeth, 2 studies, 1 Low & 1 ‘Some Concerns’ RoB, Figure 2C), the > 1-day-till-3-days interval (MDpooled, −1.26; 95% CI, −5.2 to 2.68; I2 = 0%; Figure 2D) or at the > 3-day-till-14-days interval (MDpooled, −0.34; 95% CI, −4.69 to 4.02; I2 = 0%; Figure 2E); the CoE for all the time intervals is moderate (Supplementary Table 5).
Figure 2
Calcium hydroxide (CH) versus no intracanal medication (ICM) comparison. Forest plots showing postoperative pain incidence within (A) the > 1-day-till-3-days interval, and (B) the > 3-day-till-14-days interval; and postoperative pain intensity within (C) the ≤ 1-day interval, (D) the > 1-day-till-3-days interval, and (E) the > 3-day-till-14-days interval.
CI, confidence interval; SD, standard deviation.
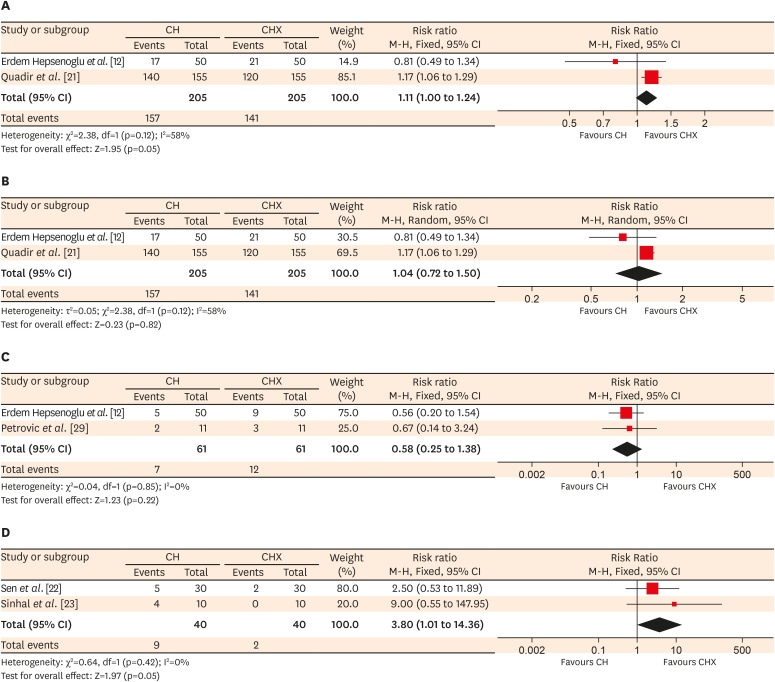
Three studies assessed pain incidence of CH versus CHX [122129]. There was no differences in pain risk at the ≤ 1-day interval (RR, 0.86; 95% CI, 0.64 to 1.16; 100 teeth, 1 study, High RoB) [12] or the > 1-day-till-3-days interval (RRpooled, 1.11; 95% CI, 1 to 1.24; I2 = 58%; 410 teeth, 2 studies, 1 ‘Some Concerns’ & 1 High RoB, Figure 3A); a sensitivity analysis using the random-effect model also showed no difference (RR, 1.04; 95% CI, 0.72 to 1.50; Figure 3B) [1221]. No difference was also reported at the > 3-day-till-14-days interval (RR, 0.58; 95% CI, 0.25 to 1.38; I2 = 0%; 122 teeth, 2 studies, 2 High RoB, Figure 3C) [1229]. The CoE for all the time intervals is very low (Supplementary Table 6). One study [11] showed that CHX decreased pain intensity than CH at the ≤ 1-day (MD, 6.3; 95% CI, 4.45 to 8.15; 32 teeth, Low RoB), the > 1-day-till-3-days (MD, 7.69; 95% CI, 4.22 to 11.16) and the > 3-day-till-14-days (MD, 10.3; 95% CI, 6.31 to 14.29) intervals. The CoE for all the time intervals is moderate (Supplementary Table 6).
Figure 3
Calcium hydroxide (CH) versus chlorhexidine (CHX) comparison. Forest plots showing postoperative pain incidence within (A) the > 1-day-till-3-days interval, with (B) its sensitivity analysis using the random-effect model, then within (C) the > 3-day-till-14-days interval. (D) Flare-up incidence forest plot.
CI, confidence interval.
On comparing CH with CH/CHX, one study [20] reported no difference in pain incidence at either the ≤ 1-day (RR, 0.33; 95% CI, 0.07 to 1.54; 70 teeth, High RoB) or the > 3-day-till-14-days (RR, 0.5; 95% CI, 0.1 to 2.56) intervals; the CoE is very low (Supplementary Table 7). One study [11] showed a significant decrease in pain intensity with CH/CHX than CH at the ≤ 1-day (MD, 8; 95% CI, 6.14 to 9.86; 32 teeth, Low RoB), the > 1-day-till-3-days (MD, 10.19; 95% CI, 6.7 to 13.68) and the > 3-day-till-14-days (MD, 10.99; 95% CI, 7.04 to 14.94) intervals; the CoE is moderate (Supplementary Table 7).
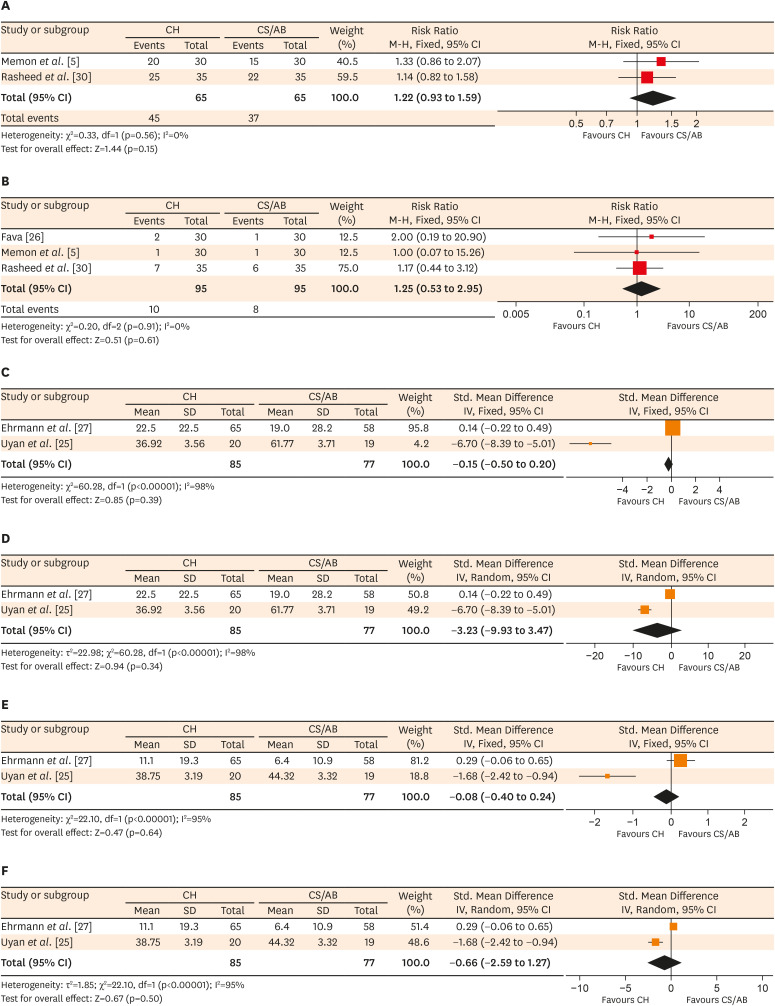
Three studies assessed pain incidence of CH versus CS/AB [52630]. There was no difference in pain risk at the ≤ 1-day interval (RRpooled, 1.22; 95% CI, 0.93 to 1.59; I2 = 0%; 130 teeth, 2 studies, 2 High RoB, Figure 4A) [530], the > 1-day-till-3-days interval (RRpooled, 1.25; 95% CI, 0.53 to 2.95; I2 = 0%; 190 teeth, 3 studies, 3 High RoB, Figure 4B) or the > 3-day-till-14-days interval (RR, 0.33; 95% CI, 0.01 to 7.87; I2 = 0%; 60 teeth, 1 study, High RoB) [5]; at the latest interval, a second study [26] reported zero events in both groups so RR was not estimable (60 teeth, 1 study, High RoB). The CoE for all the time intervals is very low (Supplementary Table 8). Two studies reported data for pain intensity [2527]. There was no differences at the ≤ 1-day interval (SMDpooled, −0.15; 95% CI, −0.5 to 0.2; I2 = 98%; 162 teeth, 2 studies, 2 ‘Some Concerns’ RoB, Figure 4C); sensitivity analysis using the random-effect model showed no difference (SMDpooled, −3.23; 95% CI, −9.93 to 3.47; Figure 4D). There was no difference at the > 1-day-till-3-days interval (SMDpooled, −0.08; 95% CI, −0.4 to 0.24; I2 = 95%; 162 teeth, 2 studies, 2 ‘Some Concerns’ RoB, Figure 4E) or the > 3-day-till-14-days interval (MD, 4.5; 95% CI, −0.32 to 9.32; 123 teeth, 1 study, ‘Some Concerns’ RoB) [27]. A sensitivity analysis, using the random-effect model, showed no difference for the > 1-day-till-3-days interval (SMDpooled, −0.66; 95% CI, −2.59 to 1.27; Figure 4F). The CoE is very low for the first two time intervals and low for the last (Supplementary Table 8).
Figure 4
Calcium hydroxide (CH) versus corticosteroid/antibiotic combination (CS/AB) comparison. Forest plots showing postoperative pain incidence within (A) the ≤ 1-day interval, and (B) the > 1-day-till-3-days interval; and postoperative pain intensity within (C) the ≤ 1-day interval, with (D) its sensitivity analysis using the random-effect model, then within (E) the > 1-day-till-3-days interval with (F) its sensitivity analysis using the random-effect model.
One study [25] showed less pain intensity with CH than TAP at the ≤ 1-day interval (MD, −8.03; 95% CI, −0.22 to −5.84; 40 teeth, ‘Some Concerns’ RoB) but no difference at the > 1-day-till-3-days interval (MD, 1.93; 95% CI, −0.03 to 3.89); the CoE is low for both time intervals (Supplementary Table 9).
One study [24] showed no difference between CH and DAP in pain risk at the ≤ 1-day interval (RR, 1.11; 95% CI, 0.60 to 2.07; 36 teeth, Low RoB) or the > 1-day-till-3-days (RR, 0.57; 95% CI, 0.20 to 1.62) intervals.
2. Flare-up
One study [28] assessed flare-up incidence of CH versus no ICM and reported no difference in flare-up incidence between CH and no ICM at 4 hours (RR, 0.74; 95% CI, 0.32 to 1.69; 137 teeth, High RoB) and 1 day (RR, 0.28; 95% CI, 0.06 to 1.26) postoperatively; the CoE is very low (Supplementary Table 5).
Two studies [2223] (90 participants, 2 High RoB) assessed flare-up incidence of CH versus CHX showing a decrease in the risk with CHX risk than CH (RRpooled, 3.80; 95% CI, 1.01 to 14.36; I2 = 0%; 80 teeth, 2 studies, 2 High RoB, Figure 3D); the CoE is very low (Supplementary Table 6).
One study [20] reported no difference between CH and CH/CHX in flare-up risk (RR, 0.5; 95% CI, 0.1 to 2.56; 70 teeth, High RoB); the CoE is very low (Supplementary Table 7).
One study [28] reported no difference between CH and CS/AB at 4 hours (RR, 1.78; 95% CI, 0.57 to 5.62; 123 teeth, High RoB) and 1 day (RR, 0.59; 95% CI, 0.1 to 3.44) and another study [25] reported zero events for both groups (39 teeth, ‘Some concerns’ RoB). The CoE is very low (Supplementary Table 8).
One study [23] reported no difference between CH and TAP in the risk of flare-up between groups (RR, 9; 95% CI, 0.55 to 147.95; 20 teeth, High RoB) and another study [25] reported zero events for both groups (40 teeth, ‘Some concerns’ RoB); the CoE is very low (Supplementary Table 9).
3. Swelling
One study [4] compared swelling incidence with CH versus no ICM reporting no difference at 3 days (RR, 0.33; 95% CI, 0.08 to 1.46; 40 teeth, High RoB) or at 10 days (RR, 0.2; 95% CI, 0.01 to 3.92). One study [20] (70 teeth, ‘Some Concerns’ RoB) compared CH versus CH/CHX reporting zero events of swelling at 1 day, 1 week, and 1, 3, and 6 months.
DISCUSSION
Despite that CH is considered the most common ICM used during root canal treatment [7], yet, very few systematic reviews have assessed its effect on postoperative pain [1516]. Thus, this study aimed to systematically review and provide a pooled effect estimate, if possible, for effects on pain and flare-up regarding CH compared to no other ICMs.
In the present review, nine electronic databases were searched, using free-text and controlled-vocabulary terms that represent sources for published and grey literature with no restriction to date, language, or publication status to allow a comprehensive search. At least 2 reviewers independently performed the identification of the included studies, data extraction, and risk of bias assessment. The authors of the trials were contacted via e-mail whenever missing data was detected. Inclusion criteria reflected the population most likely to receive an ICM during non-surgical endodontic treatment of patients having mature teeth with non-vital pulp. The best study design to answer a therapeutic clinical question is a randomized clinical trial, which was the only design included in the present review. Whenever detected, substantial heterogeneity causes were assessed using sensitivity analysis by using the random-effects model while being cautious in interpreting results.
A total of 16 articles were included in this systematic review, which included 1643 participants with 1699 teeth, of which 1,657 were analyzed. Available clinical trials have compared CH to no or various other ICMs. However, very few studies were included in most comparisons precluding the possibility of drawing valid, reliable conclusions. The majority of studies had a relatively small size (11 of 16 articles with < 100 participants) (Table 2). Despite the relatively-homogenous clinical procedures across studies, yet, statistical heterogeneity existed in some instances which could influence the validity of the pooled estimates. Most studies showed a high risk of bias relative to most outcomes (Table 3), which further downgrades the certainty of estimates.
According to the RoB 2.0 tool, only two articles of the included 13 assessing postoperative pain [1124] showed a low risk of bias. Most of the included articles showed an overall high risk of bias on the outcome level mostly due to having a high risk of bias in the domain of “bias in measurement of the outcome” which is attributed to the lack of information about blinding of the outcome assessor to the intervention regarding participants-reported outcomes (e.g., pain and flare-up). Some studies had a high risk of bias in the domain “bias in selection of the reported results” due to the selective reporting of one time point or more in each outcome from those time points reported by the authors. Regarding the domain “bias arising from randomization process”, the majority of the studies had ‘Some Concerns’ about bias due to lack of information about sequence generation, allocation sequence concealment, and baseline characteristics.
On comparing CH with no ICM, CH does not seem to affect postoperative pain prevention within the first 24 hours [10], yet it could be of benefit afterward in reducing pain risk by about 12% within the following 2 days and 87% afterward (Figure 2A and 2B) [41021]. Results, however, should be interpreted with caution due to the overall low-to-moderate quality evidence (Supplementary Table 5). Considering the potential microbiologic etiology of post-endodontic pain [31], CH has been postulated to have pain-preventive properties which can be attributed due to its antibacterial, anti-inflammatory, and tissue-altering properties [4910111226]. However, such effect may fail to always occur [2728] which has been attributed to the dentin-buffering effect or the resistance of some of the canal microbiota against CH in addition to the ineffectiveness of CH to penetrate deep into dentinal tubules [11162728].
Very-low quality evidence revealed a similarity in the efficacy of CH and CHX alone or when mixed with CH in pain-risk prevention (Figure 3A-3C, Supplementary Tables 6 and 7) [122129], while moderate-quality evidence showed that CHX may be more beneficial in reducing pain severity either alone or when added to CH [11] (Supplementary Tables 6 and 7); such reduction in severity, however, may not be that clinically significant being less than 15 points on a 0–100 pain scale [32]. CHX was also effective in reducing flare-up risk than CH by around 75% (RRpooled, 0.26; 95% CI, 0.07 to 0.99) in a population with the majority of patients being diabetic; evidence, however, is of very low quality.
The superiority of CHX and its enhancing effect to CH in controlling postoperative painful incidents compared to CH alone has been demonstrated in several studies [11212223]. This has been attributed to CHX’s high diffusibility, substantivity, better effectiveness against resistant microbiota (e.g., Enterococcus faecalis and Candida albicans); its addition to CH also had a positive effect on CH's antimicrobial activity and the medication wettability to dentin [333435]. Diabetic patients have higher incidence rates of Candida-based infections [36], which can be more sensitive to CHX than CH [2223]. Two of the three studies assessing pain incidence [1229] included cases with endodontic failure requiring retreatment; endodontic failure cases show a prevalence of Enterococcus faecalis within their microbiota [37].
Pooled estimates showed a similar effect of CH and CS/AB on pain incidence and severity; results, however, should be interpreted with caution due to the overall very-low quality of evidence (Figure 4A-4F, Supplementary Table 8). Despite that CH statistically significantly reduced pain severity than TAP within the first 24 hours [25], such reduction may be of little clinical importance being only a difference of 8 points on a 0–170 cm Heft-Parker scale (MD, −8.03; 95% CI, −10.22 to −5.84); evidence, however, is of low quality from a single study (Supplementary Table 9).
Substantial heterogeneity has been recorded in some instances of data synthesis with pain incidence (Figure 3A) or pain intensity (Figure 4C and 4E). The main concern with pain studies is the tool used to measure pain since it can introduce a source of clinical heterogeneity among studies [1932] where the number of response points within a scale is important since a small number requires a larger change in pain before scores change. In contrast, a large number can be useless as it can have more levels of discrimination than most patients use [3238]. Differences in the included populations in studies can also be a source of heterogeneity among pain-intensity studies comparing CH with CS/AB (Figure 4C and 4E), and pain-incidence studies comparing CH with CHX (Figure 3A).
The scarcity of available studies relevant to the research question in the endodontic literature, together with their limited sample size, is considered an obvious limitation that precludes meta-analysis in several instances. When performed, however, meta-analyses were often associated with substantial heterogeneity. The high risk of bias in most of the included studies in this review also represents a critical limitation affecting the ability to draw valid, reliable conclusions about CH effects on pain and flare-up. An important strength of this study, however, might be the ability to perform the meta-analysis to obtain pooled estimates.
CONCLUSIONS
Most comparisons for different outcomes at the different time points had their results based on very few studies, usually 1 or 2 low-powered studies, with an overall low certainty of evidence. Thus, available evidence can be considered insufficient to either support or refute CH effectiveness or to recommend one ICM over another. Further well-designed, larger-size randomized clinical trials are, thus, required to provide higher-quality, reliable evidence.
 XML Download
XML Download