

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The global population is growing and is experiencing both an increase in life expectancy and a decrease in tooth loss [1]. Since root canal treatment is performed in patients of all ages, clinicians should be aware of differences in root canal system morphology and dentinal structure depending on the patient's age.
It has been previously stated that it is virtually impossible to establish guidelines or instrument calibers that will guarantee adequate canal preparation in any age group [2]. Nonetheless, based on differences in canal morphology and dentinal structure and as a result of the diverse endodontic instruments and techniques that are available today, the clinician may adopt different means for instrumentation of the root canal system.
Meanwhile, various instruments—especially shaping files made of different heat-treated alloys with different geometric characteristics—have been reported to have distinctive mechanical properties and consequent shaping results [345]. The choice of instrumentation may result in inappropriate clinical results in certain cases, depending on the instrument's properties and the patient's clinical condition, including age. Therefore, the aim of this article was to review age-dependent clinical recommendations for root canal instrumentation techniques via a literature search and review.
Go to : 
METHODS
Literature search and scope of the review
An electronic literature search was carried out, including the MEDLINE (Ovid), PubMed, and Web of Science databases. The searches used controlled vocabulary and free-text terms, as follows: ‘age-related root canal treatment,’ ‘age-related instrumentation,’ ‘age-related chemo-mechanical preparation,’ ‘age-related endodontic clinical recommendations,’ ‘root canal instrumentation at different ages,’ ‘geriatric root canal treatment,’ and ‘pediatric root canal treatment.’ However, the review of the literature revealed a lack of studies with practical clinical recommendations referring to age in choosing appropriate root canal instrumentation.
Therefore, a comprehensive narrative review of canal morphology, the structural characteristics of dentin, and endodontic outcomes at different ages was undertaken from articles that were published from 1925 to 2018 instead of a systematic review. Narrative reviews are most useful for obtaining a broad perspective on a topic and are often more comparable to a textbook chapter, including sections on the physiology and/or epidemiology of a topic. Based on this narrative review, a clinical algorithm for choosing the most appropriate instrumentation during root canal treatment was proposed.
Previous studies have taken different approaches to categorizing age-related morphological and structural changes, either basing them on statistical preferences (to ensure larger sample sizes) [67] or without explaining the categorization [8910]. This review categorizes age-related differences by the following age groups: individuals who are 20 years old or less, between 21 and 40 years old, and 41 years old or more.
Age-related root canal morphology
1. Canal cross-sectional outline and diameter
Differentiation of the root canal system due to the deposition of secondary dentin is an age-dependent process [8]. The pulp cavity generally decreases in size as an individual ages (Figure 1) [111213].
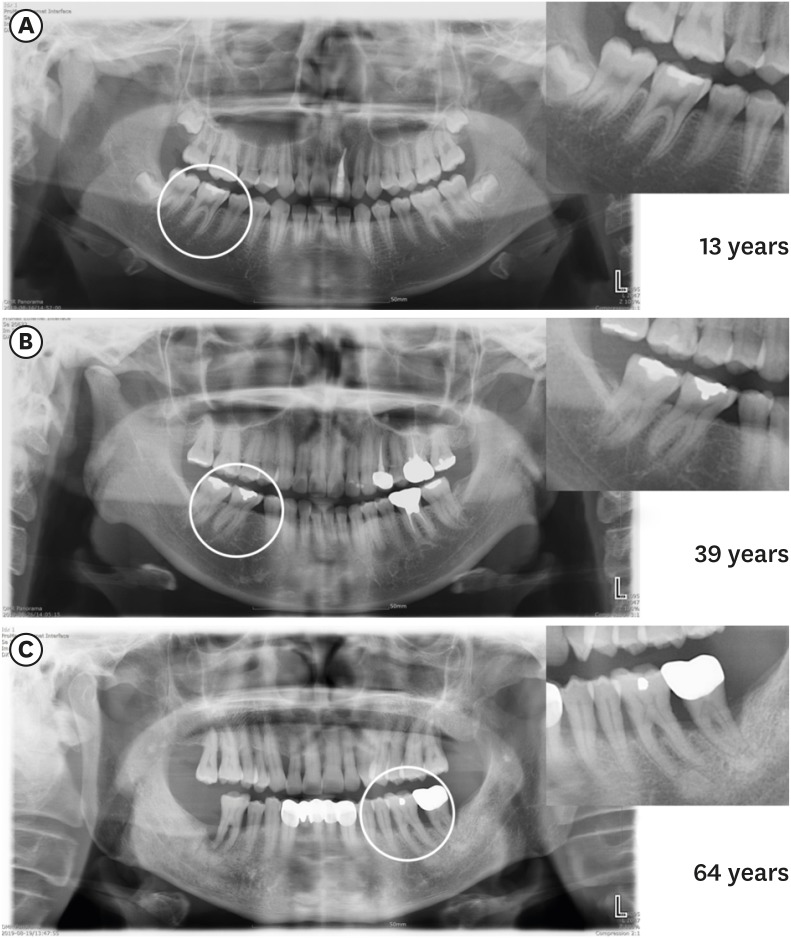 | Figure 1Panoramic radiography images showing the chamber and canal sizes according at different ages. (A) Individuals under 20 years old (13 years), (B) individuals between 20 and 40 years old (39 years), (C) individuals over 40 years old (64 years). The image in (A) shows a large chamber and a straight direction to the canal orifice. The image in (B) shows a dentin shelf area and an angulated direction to canal orifice. The image in (C) shows a thin chamber area and sclerotic canals.
|
In general, in individuals who are 20 years old or less, the roots have a single large root canal (mostly oval) [78111415]. Middle mesial canals in mandibular molars occur mostly in individuals younger than 21 years old [16]. Individuals who are 20 to 40 years old have multiple separate canals [781115]. The number of root canals was mainly found to increase in the maxillary and mandibular second premolars, the distal root of mandibular first molars, and the lower incisors [7141718]. More round canals were found in the second mandibular molars in patients over 35 years old, while more oval canals were found in the teeth of individuals younger than 35 years of age [14].
A C-shaped configuration (category III) is more common in the mandibular molars of individuals who are 40 years old or less [1419]. In a cone-beam computed tomography study, patients less than 42 years old were 4 times more likely to have a middle mesial canal than patients older than 42 years [20]. In individuals older than 40 years of age, the deposition of secondary dentin resulted in decreased canal diameter and the disappearance of additional canals [21]. In individuals 51–70 years of age, fewer canals were found [22]. For example, a decrease in the presence of the second mesiobuccal canal in the maxillary molars was observed in this age group [61517222324252627].
2. Isthmuses
The incidence of canal isthmuses appears to be age-related [28]. Individuals who are 20 years old or less have wide and oval canals without isthmuses at the early stages of root development [29]. In individuals between 20 and 40 years old, the deposition of secondary dentin in the mesiodistal direction results in the formation of 2 canals with an isthmus [2930]. Up to 81% of mesial roots of the mandibular first molars of individuals aged 20-39 years old have isthmuses, particularly at apical 4 to 6 mm [29]. In individuals who are 40 years old or more, the prevalence and volume of isthmuses significantly decrease, and the canal becomes completely separated. In individuals who are over 50, the prevalence of isthmuses was found to be 16.7% [31] and only 24% of individuals over 60 years of age had isthmuses in mesial roots of the mandibular molars [29]. The ratio of partial isthmuses to complete isthmuses has been shown to increase with age [2932]. Figure 2 shows the characteristics of isthmuses at different ages with axial cone-beam computed tomography images.
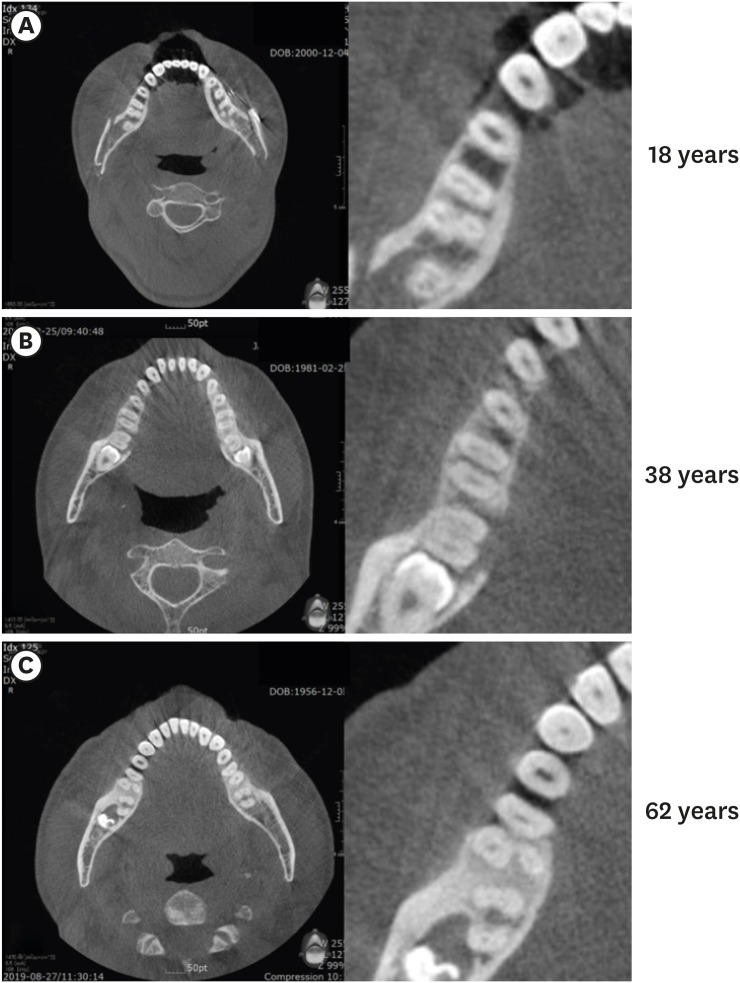 | Figure 2Axial cone-beam computed tomography images of 3 mandibular first molars, showing isthmus characteristics at different ages. (A) Individuals under 20 years old (18 years): a wide canal without an isthmus, (B) individuals between 20 and 40 years old (38 years): an isthmus in the mesial root, (C) individuals who are 40 years old or more (62 years): sclerotic mesial canals without an isthmus, resembling a single canal.
|
Age-related changes in dentinal structure
Normal dentin undergoes physiological alteration to transparent (sclerotic) dentin with age [3334]. As the tooth matures, the peritubular dentin becomes more mineralized [35], and there is a decrease in the mean number of dentinal tubules [36]. The mineralization process and dentin sclerosis result in a narrowing of the tubules. In some instances, the process can lead to complete obliteration of the dentinal tubules [333537]. Mineralization starts in the third decade of life in the apical region and advances coronally with age [53839].
The penetration of bacteria into the dentinal tubules could be a determinant of their virulence in the root canal environment [40]. The microbial load and diversity are higher in young individuals and decrease with age [41]. This decrease may be attributed to tubular mineralization, as well as to a decrease in the pulp cavity space, isthmuses, and additional canals. Tubules are usually larger in diameter than the average Enterococcus faecalis (E. faecalis) cell diameter by approximately 0.8–1 nm [4243444546]. However, due to age-dependent tubular mineralization, there is a decreased depth of E. faecalis penetration into the dentin through sclerotic or obliterated tubules in aged dentin [40]. On average, bacteria invade 65 µm less deeply in individuals who are 60–77 years old than in individuals who are 18–24 years old [40].
As an individual ages, the water content of dentin decreases and modifications of collagen, such as cross-linking, increase [47]. Due to these age-related changes, the damage tolerance of teeth decreases in older individuals [484950], as well as a significant reduction in dentin strength and fracture toughness, resulting in an increase in vertical root fracture (VRF) incidence with age [495152]. VRFs mostly occur in the posterior teeth of patients between 40 and 60 years old [5354]. In addition, the incremental crack growth rate in ‘old’ dehydrated dentin is 100 times faster than in ‘young’ hydrated dentin [55]. Pre-existing dentinal microcracks in non-endodontically treated roots become more common with age (8.3% in individuals over 40 years old vs. 3.7% in individuals who are 20–39 years old) [56]. In contrast, in individuals who are under 20 years old, the dentin walls are thin, which may lead to coronal or radicular tooth fractures during normal functional stress [5758].
Age-related outcomes
The reports of the effects of the patient's age on the outcomes of endodontic treatment are conflicting. Some studies have reported that age had no statistically significant influence on the results [59606162], while others claimed that the patient's age significantly influenced the results [63]. Some studies found that older patients had a higher percentage of success than younger patients [12646566], while other researchers found better outcomes in younger patients [6367] and demonstrated that age was a risk factor for experiencing an adverse event. For instance, older patients were 1.4 times more likely to undergo an extraction procedure after root canal therapy [68]. The incidence of a subsequent extraction increases by 1% to 2% each decade, until reaching a plateau after the age of 60 [69].
Findings of better outcomes for older individuals might be explained by the progressive reduction of pulp space, disappearance of auxiliary canals and isthmuses, and narrowing of dentinal tubules up to total obliteration [3640]. These changes limit the volume available for infection and make it easier to provide adequate canal debridement, as well as root canal shaping and cleaning [12]. Reports of better outcomes for younger individuals might be explained by the increased prevalence of pre-existing apical periodontitis with age, which has been associated with a lower likelihood of success of endodontic procedures [70]. Another explanation might be that older individuals have slower and less effective healing processes or a prolonged healing time [1271]. The immunological changes that occur due to aging [7273] include changes in the pulpal cells expressing macrophage-associated antigens [74]. Aging is associated with a low level of expression of genes encoding for transcription regulators and a high level of expression of genes involved in apoptotic processes [75].
Furthermore, systemic diseases are more prevalent in older age groups [76], and it has been reported that some systemic diseases might be correlated with endodontic outcomes [77]. Diabetes (non-insulin dependent or insulin dependent) or an impaired, nonspecific immune response results in a reduced likelihood of successful endodontic treatment in patients with preoperative periradicular lesions [7879].
Table 1 displays the characteristics of canal morphology and dentinal structure in different age groups, including the canal cross-sectional outline and diameter, the presence and characteristics of isthmuses, auxiliary canals, the quantity and diameter of dentinal tubules, and dentinal sclerosis. Collectively, these age-related changes suggest that the clinician may opt for different clinical approaches for different age groups.
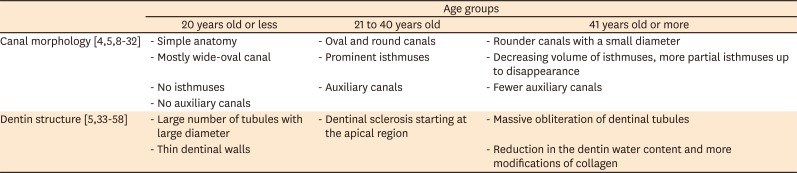
Table 1
Characteristics of canal morphology and dentinal structure in different age groups
| Age groups | |||
|---|---|---|---|
| 20 years old or less | 21 to 40 years old | 41 years old or more | |
| Canal morphology [45891011121314151617181920212223242526272829303132] | - Simple anatomy | - Oval and round canals | - Rounder canals with a small diameter |
| - Mostly wide-oval canal | - Prominent isthmuses | - Decreasing volume of isthmuses, more partial isthmuses up to disappearance | |
| - No isthmuses | - Auxiliary canals | - Fewer auxiliary canals | |
| - No auxiliary canals | |||
| Dentin structure [53334353637383940414243444546474849505152535455565758] | - Large number of tubules with large diameter | - Dentinal sclerosis starting at the apical region | - Massive obliteration of dentinal tubules |
| - Thin dentinal walls | - Reduction in the dentin water content and more modifications of collagen | ||
![]()
Possible clinical suggestions
Within the limitations of the studies that were analyzed, the following possible clinical suggestions for root canal instrumentation can be made. For individuals who are 20 years old or less, the recommendations are as follows. Large canals do not require additional widening. Instruments with a scraping action may be preferred to clean the root canal wall of biofilm and simultaneously activate the irrigation solution [8081]. Possible instruments are the Self-Adjusting File (SAF; ReDent, Ra'anana, Israel) [82] and the XP-Endo Finisher (FKG Dentaire, La Chaux-de-Fonds, Switzerland) [83]. These systems are efficient for cleaning the comparably large and oval canal lumen by a scrubbing action with simultaneous continual replacement of the irrigant for the SAF or eccentric movements drawing upon the specific properties of controlled-memory wired instruments such as the XP-Endo Finisher.
For individuals who are 20 to 40 years old, the following recommendations can be made. The canals are mostly patent and difficulties in the glide path are rare. In these root canal systems, regular nickel-titanium (NiTi) rotary systems can be used to shape the canal up to an apical diameter size of #30–#35 [84] with subsequent agitation using sodium hypochlorite. Possible instruments include the ProTaper Next (Dentsply Sirona, Ballaigues, Switzerland), XP-Shaper (FKG Dentaire, La Chaux-de-Fonds, Switzerland), and 2Shape (MicroMega, Besançon, France). Using scraping instruments in this age group can be considered in oval canals.
For individuals who are 40 years old or more, the recommendations are as follows. In these root canal systems, after the use of manual stainless-steel K-files (#06, #08, and #10), a NiTi system for the glide path can be used. Possible instruments include the G-file (MicroMega), PathFile (Dentsply Sirona), OneG (MicroMega), ProGlider (Dentsply Sirona), Scout RaCe, and Race ISO 10 (FKG Dentaire). Afterward, widening of the canal apical diameter up to size #30 or #35 is preferably done with NiTi instruments, which create less loading on dentin [85]. Possible instruments for this purpose are those with a smaller core (MTwo [VDW, Munich, Germany], Race [FKG Dentaire], ProFile [Dentsply Sirona], 2Shape), those with a smaller taper (0.02 and 0.04) (Race, ProFile), and those made of flexible NiTi (controlled memory wire) such as HyFlex (Coltene/Whaledent, Inc, Cuyahoga Falls, OH, USA) and Typhoon (Clinician's Choice Dental Products, New Milford, CT, USA).
Table 2 displays the proposed algorithm for root canal instrumentation in different age groups. The current suggestions are based on the available evidence and reflect the limitations of the studies that were included in the review. However, no one algorithm suits all teeth. The clinician may face incompatibility between chronological age and biological age. Pathological or iatrogenic factors might modify the canal cross-sectional outline and diameter. These factors include carious lesions or deep restorations [27], attrition or abrasion [86], occlusal trauma [87], periodontal disease and treatment [8889], and orthodontic treatment [90]. The stimuli that each tooth encounters over its lifespan should be taken into consideration due to a possible rapid increase in reactionary dentin deposition [7]. In contrast, pulp necrosis in younger patients due to trauma or caries might lead to the formation of wider canals with thin dentinal walls when those patients become older.

Table 2
The algorithm for root canal instrumentation in different age groups
![]()
The content of this review does not necessarily support any specific technique for certain clinical conditions in patients of various age ranges and root canal conditions. However, it may be generally acceptable to reinforce the importance of chemo-mechanical preparation, which always enhances canal cleaning by shaping, and activated irrigation, regardless of patients' age and canal condition. A proper evaluation of root canal morphology, coupled with an adequate understanding of the influence of age on these characteristics, may help the clinician to choose the most appropriate instrumentation and irrigation activation technique.
Go to :
CONCLUSIONS
The current review considered age-dependent differences in canal morphology, the structural characteristics of dentin, and endodontic outcomes. Age-dependent clinical suggestions for instrumentation would be ideally based on a systematic review of randomized controlled trials considering the quality of the evidence and patients' values, preferences, and financial resources. However, no studies suitable for this purpose have been carried out. Thus, the present article is the first to attempt to interpret age-dependent morphological and structural changes and to make practical clinical suggestions within the limitations of existing studies.
A systematic review is a comprehensive search method for relevant studies on a specific topic, and the identified studies are then appraised and synthesized according to a predetermined and explicit method. In contrast, a narrative review is a traditional expert review method. This method is subjective and there are no formal rules for selecting studies or standard statistical methods for combining studies. Therefore, when reading and evaluating a narrative review, readers need to keep in mind that authorial bias may or may not be present.
An additional limitation of these proposed clinical suggestions is that the abovementioned instruments are not available to all clinicians because of characteristics of the local market and financial resources. Further studies should investigate the influence of the patient's age on other aspects of root canal treatment (e.g., the preparation of access cavities, irrigant agitation methods, and obturation technique). It can be concluded that the clinician's awareness of age-related differences in root canal morphology and dentin characteristics can influence the choice of instruments for root canal treatment.
Go to :
 XML Download
XML Download