

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
When bleaching gels come into contact with dental structures, they promote the release of reactive oxygen species (ROS), which cleave the chromophore molecules present in dentin, turning them into smaller molecules and hence lightening the teeth [123]. However, the action of ROS is not limited to the oxidation of pigmenting agents; in general, these molecules are extremely unstable and highly reactive, and as a result, abnormally elevated concentrations of peroxides in the pulp tissue are frequently reported after the use of in-office bleaching techniques [2]. Peroxide formation has been associated with mild and transient hypersensitivity to inflammatory processes, and may cause irreversible pulp involvement [456].
In vivo studies on human teeth reported slight disturbances in the odontoblastic layer in the premolar pulp tissue [5] and areas of coagulative necrosis in the lower incisors [6] following in-office bleaching treatment. In vitro studies have shown that the number of bleaching sessions was closely related to morphological changes [78] and a decreased mitochondrial respiration rate in MDPC-239 odontoblast cells [9], and similar results were found for time and concentration of the bleaching agent in an in vivo study [10]. Similarly, clinical research has confirmed that patients undergoing bleaching treatments experience various levels of discomfort and alteration of the dental pain sensitivity threshold [1112].
The cellular damage caused by hydrogen peroxide penetration leads to the synthesis and release of biochemical mediators involved in the inflammatory process (e.g., prostaglandins, histamines, and bradykinins) [7]. These mediators cause increased vascular permeability and vasodilation within the pulp cavity. It is noteworthy that any increase in pulp pressure mechanically stimulates peripheral nerve fibers [13], which respond by producing and releasing certain peptide neurotransmitters, such as substance P (SP) and calcitonin gene-related peptide (CGRP) [61415]. These neuropeptides excite the transmitting neurons, thereby promoting the onset of pain signals from the tissue injury area.
In clinical practice, analgesics are administered and/or topical desensitizing agents are used before or after the bleaching procedure to minimize the discomfort that aesthetic bleaching may cause [161718]. There are several types of desensitizing agents with different mechanisms of action; some function through a physical mechanism by sealing dentinal tubules, while others exert effects on nerves by blocking nerve stimuli [19]. As examples of the latter type of mechanism, potassium nitrate products have the ability to reach the dentin-pulp complex, where they modulate the activity of sodium (Na+) and potassium (K+) channels present in the membrane, affecting the transmission of nerve impulses and decreasing tooth sensitivity [20].
Non-steroidal anti-inflammatory drugs (NSAIDs) are also widely used by professionals prior to bleaching treatment to reduce post-whitening sensitivity [2122]. NSAIDs have anti-inflammatory, analgesic, and antipyretic properties; they inhibit the cyclooxygenase pathway and decrease the production of some substances present in the inflammatory process, such as prostaglandins and thromboxanes. These drugs are also an effective alternative for postoperative analgesia because they decrease the action of these mediators on pulp pressure, attenuating peripheral nerve fiber stimulation and reducing pain [23].
Thus, considering that the clinical reports on tooth sensitivity during bleaching treatment are highly contradictory and the methods used in most studies are inaccurate, an in vivo study of the levels of SP and CGRP may provide objective information about the inflammatory profile and pain caused by bleaching treatment. These findings may help clinicians choose an efficient protocol to treat the pain caused by this aesthetic treatment, making the process more comfortable for the patient. Therefore, this in vivo study evaluated the influence of ibuprofen and the topical desensitizing agent Desensibilize KF 2% on inflammation and the expression of SP and CGRP in pulp nerve fibers after dental bleaching.
Go to : 
MATERIALS AND METHODS
Experimental design
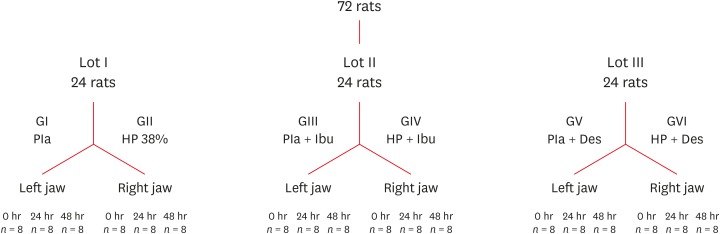
This study was approved by the Ethics Committee on the Use of Animals in Research of São Paulo State University (UNESP) School of Dentistry (protocol No. 2014-00817). The project studied 3 pain management treatments (control, ibuprofen administration, and a topical desensitizing agent) at 3 time points (T0, immediately after the bleaching procedure; T1, 24 hours after the bleaching session; and T2, 48 hours after the bleaching session). Two response variables were considered: pulp morphological analysis and neuropeptide expression.
Animals
Seventy-two male rats (Rattus albinus, Wistar), weighing approximately 250 g were kept in an environment with temperatures ranging between 22°C and 24°C and under controlled light-dark cycles (12 hours light and 12 hours dark), with 4 rats per cage. The animals were fed throughout the experimental period with a solid diet and water ad libitum.
Bleaching and desensitizing agents
The bleaching agent used in this study was Opalescence Boost, with a 38% concentration of hydrogen peroxide (Ultradent Products Inc, South Jordan, UT, USA). This product is commercially available in 2 syringes, one containing hydrogen peroxide and the other containing the thickening agent. These syringes were coupled together, and the plunger was alternated 8 times to correctly mix the product.
The desensitizing treatment prior to bleaching was carried out using Desensibilize KF 2% (FGM Dental Products, Joinville, SC, Brazil). This product contains 5% potassium nitrate and 2% sodium fluoride and is commercially available as a gel contained in a single syringe. Ibuprofen (in the form of drops of a suspension) was used at a concentration of 40 mg/kg body weight and administered by gavage.
Experimental groups and protocol of desensitizing treatments
The animals were divided into 6 groups based on the treatment received and further subdivided according to the time of analysis as follows: GI, control; GII, only dental bleaching; GIII, only ibuprofen; GIV, ibuprofen administered 30 minutes before and after the bleaching treatment and every 12 hours until the analysis; GV, only topical application of a desensitizing agent; and GVI, topical application of a desensitizing agent before dental bleaching, All placebo treatments were performed on the upper left jaw, and the bleaching treatments were performed on the upper right jaw (Figure 1).
The animals from lot 1 (GI and GII) were anesthetized through an intramuscular injection of xylazine hydrochloride (10 mg/kg, Dopaser, Calier SA, Barcelona, Spain) and ketamine hydrochloride (80 mg/kg, Vetanarcol, König SA, Avelaneda, Argentina), following which the bleaching procedure was performed on the upper right jaw [24]. No topical or systemic agent was used in the control group.
In lot 2 (GIII and GIV), the rats received 0.2 mL of 40 mg/kg ibuprofen or placebo gel application prior to anesthesia and after the bleaching treatment, which was administered every 12 hours until the time of analysis [23]. For this, a flexible, blunt-ended tube with a diameter of 4 mm was gently inserted into the animal’s mouth until it reached the stomach, and then the drug was administered. After drug administration, anesthesia was performed as in group I (GI), followed by the bleaching treatment. After the bleaching treatment or placebo gel application, one-third of the animals were euthanized, another one-third were given ibuprofen every 12 hours for a period of 1 day (analysis time, 24 hours), and the remaining one-third were given the drug for a period of 2 days (analysis time, 48 hours).
For lot 3 (GV and GVI), the anesthetic protocol was the same as that used for GI and GII. Desensibilize KF 2% was applied topically to the anesthetized rats. For this purpose, the product was deposited in a graduated syringe, and 0.01 mL of the product was applied to the rats’ molars 30 minutes before the bleaching procedure or placebo gel application. The product remained in contact with the enamel for 10 minutes, and was then removed with the aid of a gauze. The teeth were then washed to remove the product completely.
Bleaching session
Thirty minutes after the administration of ibuprofen or the application of a topical desensitizing agent in the respective groups, the gingival tissue around the upper molars of the right hemi-arch was protected with a gingival barrier (FGM Dental Products) and approximately 0.01 mL of 38% hydrogen peroxide bleaching gel was applied. The product remained in contact with the enamel for 40 minutes, after which it was removed and the surface was cleaned with cotton, paper towels, and water.
Euthanasia and obtaining samples
The animals were returned to their cages and were kept under the conditions described above. Each group was subdivided into 3 sub-groups that were either euthanized immediately or 24 hours and 48 hours after the interventions described earlier. For euthanasia, the animals were anesthetized as described above and initially subjected to transcardiac perfusion with 100 mL of 0.9% sodium chloride solution, followed by 700 mL of fixative solution consisting of 4% formaldehyde (Sigma-Aldrich, St. Louis, MO, USA) and 3.8% sodium tetraborate (Sigma-Aldrich) at an overall concentration of 0.1 M (4°C, pH 9.5). The jaws were then carefully dissected.
Histological processing
After dissection, the jaws were kept in the same fixative solution for 8 additional hours, rinsed in running water for 12 hours, and immersed in a 10% ethylenediaminetetraacetic acid demineralizing solution (Sigma-Aldrich).
Subsequently, the jaws were again washed in running water and gradually dehydrated using ethyl alcohol. They were then diaphanized in xylol, and the pieces were impregnated and embedded in paraffin. The correct orientation of the specimen was checked at the time of inclusion in paraffin, which helped to obtain histological sections covering the upper molars and their supporting structures in the longitudinal direction.
Microtomy was performed using a slip microtome (Leica Microsystems - RM 2045, Wetzlar, Germany), resulting in 6-µm-thick serial sections, which were collected on albumin-coated slides. The sequence of the sections was 1 section for histological analysis followed by 2 sections for immunohistochemical analysis. Following this sequence, 4 sections that were destined for histopathological analysis were stained with hematoxylin and eosin [25].
Indirect immunoperoxidase technique
The histological sections were deparaffinized in xylol and hydrated in decreasing concentrations of ethanol. Antigenic recovery was performed by immersing the histological slides in a pressurized Decloaking Chamber (Biocare Medical, Concord, CA, USA) containing Diva Decloaker buffer (Biocare Medical) at 95°C for 10 minutes at the end of each step of the immunohistochemical reaction, at which point washes were performed with 0.1 M phosphate-buffered saline (pH 7.4).
The histological sections were immersed in a 3% hydrogen peroxide solution for 1 hour and then in a 4.5% powdered milk solution to block endogenous biotin. The sections were subsequently immersed in 1% bovine serum albumin for 12 hours to block non-specific sites. Subsequently, incubation was performed for 24 hours with one of the following primary antibodies: anti-SP (Santa Cruz Biotechnology, Santa Cruz, CA, USA) or anti-CGRP (Santa Cruz Biotechnology). The primary antibodies were diluted in Dako Antibody Diluent (Dako Laboratories, Carpenteria, CA, USA). In the subsequent steps, the Universal Dako Labeled (horseradish peroxidase [HRP]) Streptavidin-Biotin Kit (Dako Laboratories) was employed. Histological sections were incubated in the biotinylated secondary antibody for 2 hours and treated with streptavidin conjugated with HRP for 1 hour. In the disclosure step, diaminobenzidine 3,3′-tetrachlorhydrate (DAB chromogen Kit, Dako Laboratories) was used as the chromogen. The histological sections were protected using a mounting medium and glass coverslip. As a negative control, the specimens were subjected to the procedures described above without the use of primary antibodies.
Histopathological analysis
The histological preparations were observed under an optical microscope (DM 4000 B, Leica, Wetzlar, Germany). Four equidistant histological sections of the maxillary first molar dental pulp were used. In the histopathological analysis, the following parameters were evaluated: the degree of inflammation, the presence and extent of necrosis, the status of the vasculature, and the cellularity pattern of the odontoblastic layer, subodontoblastic layer, and central zone of the pulp. A semi-quantitative analysis of inflammation was performed. The following scores were assigned to each third of the crown (occlusal, medial, and cervical) and each third of the root (coronal, medial, and apical): 1, absence of inflammatory cells or a negligible number thereof; 2, minimal inflammatory infiltrate; 3, moderate inflammatory infiltrate; 4, severe inflammatory infiltrate; and 5, necrosis and absence of any cell type (modified from Cintra et al. [9]).
Immunohistochemical analysis
The histological preparations were observed under an optical microscope (Optiphot-2, Nikon, Tokyo, Japan) at ×1,000 magnification by an evaluator who was unaware of the experimental groups being analyzed. Immunostaining was defined as the presence of a brownish color in cells, nerve fibers, and extracellular matrix. For each marker, 4 equidistant histological sections of the maxillary first molar dental pulp were used. Immunohistochemical analysis was performed for each third of the coronary pulp (occlusal, medial, and cervical) and root pulp (coronal, medial, and apical), with the following scores assigned to each third: 1, no immunostaining; 2, low immunostaining; 3, moderate immunostaining; 4, high immunostaining; and 5, areas of necrosis with markings of cell precipitates.
Statistical analysis
In order to analyze the effects of the desensitizing agent and ibuprofen in isolation on the pulp health of the rats, the statistical analysis of the control groups was performed separately from the other groups in which the bleaching agent was applied. The results are described according to the coronary (occlusal, middle, and cervical) and radicular (coronal, middle, and apical) thirds. The data were analyzed by the Kruskal-Wallis test, followed by the Dunn test (p < 0.05).
Go to :
RESULTS
Analysis of control groups
In the histological and immunohistochemical analysis, the crown and root portions of the 3 control groups (GI, GIII, and GV) showed normal pulp tissue. The sections that received placebo and control gel treatments showed tissue in normal condition, indicating that neither treatment damaged the pulp tissue. The immunohistochemical analysis showed light immunolabeling for both neuropeptides (SP and CGRP) in the 3 control groups. However, there were no statistically significant differences between any of the sections and time points analyzed.
Histological analysis
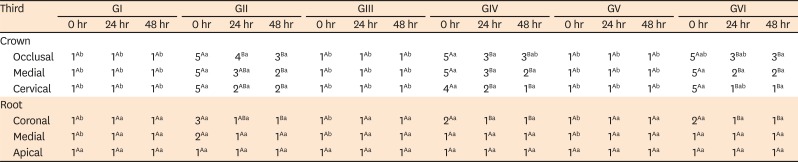
Table 1 and Figure 2 show the scores from the histopathological analysis of each coronary and root third of the bleaching groups. At 0 hours, all of the groups receiving the bleaching treatment were similar to each other. However, GII and GVI presented areas of necrosis and cell absence throughout the coronary portion. Despite the predominance of necrotic cells in GIV, inflammatory cells were observed in the coronary thirds in the bleaching groups. Regarding the root portion, only GII presented severe inflammatory infiltrate in the coronary third, while GIV presented moderate inflammatory infiltrate and GVI presented mild inflammatory infiltrate, similar to the control group. At 24 hours, GVI was the only group that presented moderate inflammatory infiltrate in the medium third and low inflammatory infiltrate in the cervical third, similar to the control group. At 48 hours, the coronary thirds of GII, GIV, and GIV showed similar patterns of cell proliferation and other parameters. Over time, the condition of the pulp showed significant improvements in all groups that underwent bleaching treatment. No statistically significant differences in the root portion were found between any of the groups.
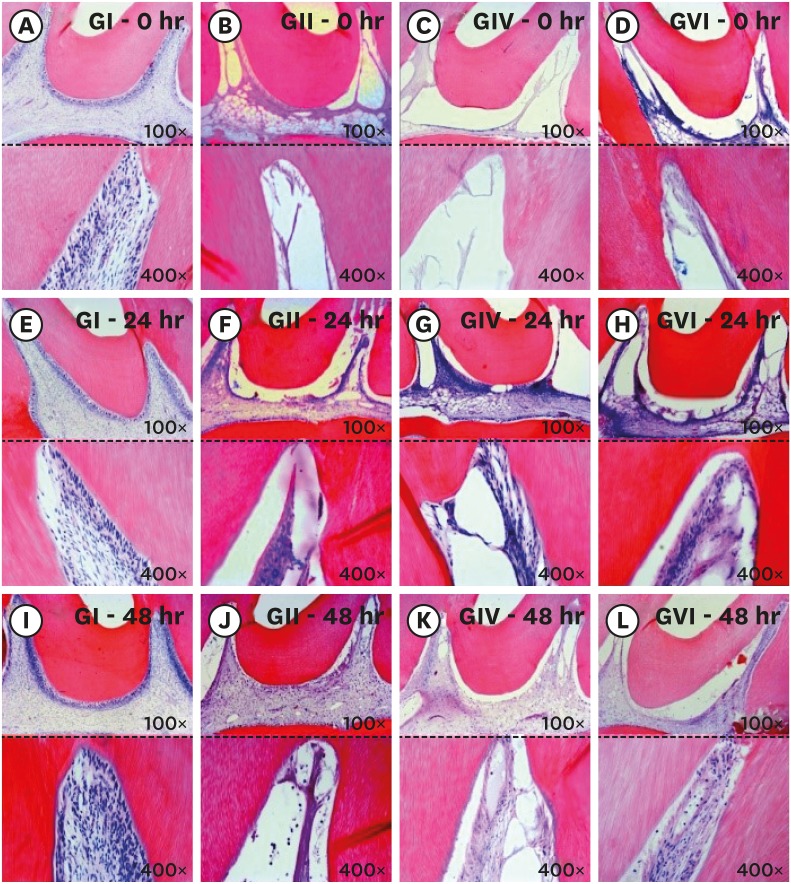 | Figure 2Longitudinal section of the coronary third of the pulp tissue of the study groups. The (A-D) correspond to photomicrographs immediately after bleaching: control group (A), 38% hydrogen peroxide without pain-relieving therapy (B), bleaching therapy associated with oral administration of ibuprofen (C), and bleaching therapy associated with topical application of Desensibilize KF 2% (D). The (E-H) correspond to photomicrographs at 24 hours after bleaching: control group (E), 38% hydrogen peroxide without pain-relieving therapy (F), bleaching therapy associated with oral administration of ibuprofen (G), and bleaching therapy associated with topical application of Desensibilize KF 2% (H). The (I-L) correspond to photomicrographs at 48 hours after bleaching: control group (I), 38% hydrogen peroxide without pain-relieving therapy (J), bleaching therapy associated with oral administration of ibuprofen (K), and bleaching therapy associated with topical application of Desensibilize KF 2%.
|
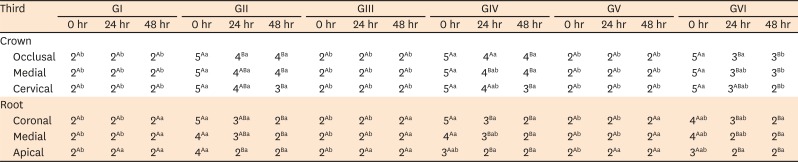
Table 1
Median scores from the histological analysis of each crown and radicular third for all groups
Six groups were divided as follows: GI, control; GII, boost 38%; GIII, control + ibuprofen; GIV, boost 38% + ibuprofen; GV, control + desensibilize; and GVI, boost 38% + desensibilize.
Means followed by different letters represent statistically significant differences (p < 0.05). Different lowercase letters indicate statistically significant differences between columns in the same rows, and uppercase letters indicate statistically significant differences between rows within the same column.
![]()
Immunohistochemical analysis
1. Immunohistochemical analysis of SP
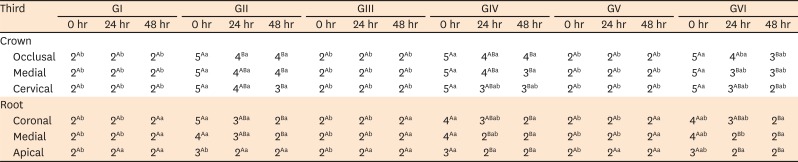
Table 2 and Figure 3 present the scores from the immunohistochemical analysis of each coronary and root third of the bleaching groups. At 0 hours, the coronary thirds of the bleaching groups (GII, GIV, and GVI) presented areas of necrosis in all sections analyzed. There was a statistically significant difference between these groups and the control group (GI), which presented a low immunostaining pattern, but without necrotic areas. At 24 hours, only the GVI (in the middle third) and group GIV (in the cervical third) presented a low immunolabeling pattern. At 48 hours, only GVI presented a low immunolabeling pattern in all thirds. Regarding the root thirds at 0 hours, it was observed that the bleaching groups (GII, GIV, and GVI) presented a high immunostaining pattern and areas of necrosis with markings of cell precipitates, reflecting a statistically significant difference from the control group (GI). At 24 hours, a moderate immunostaining pattern was observed, and at 48 hours a low immunostaining pattern was noted, with a gradual and continuous improvement in all thirds over time.
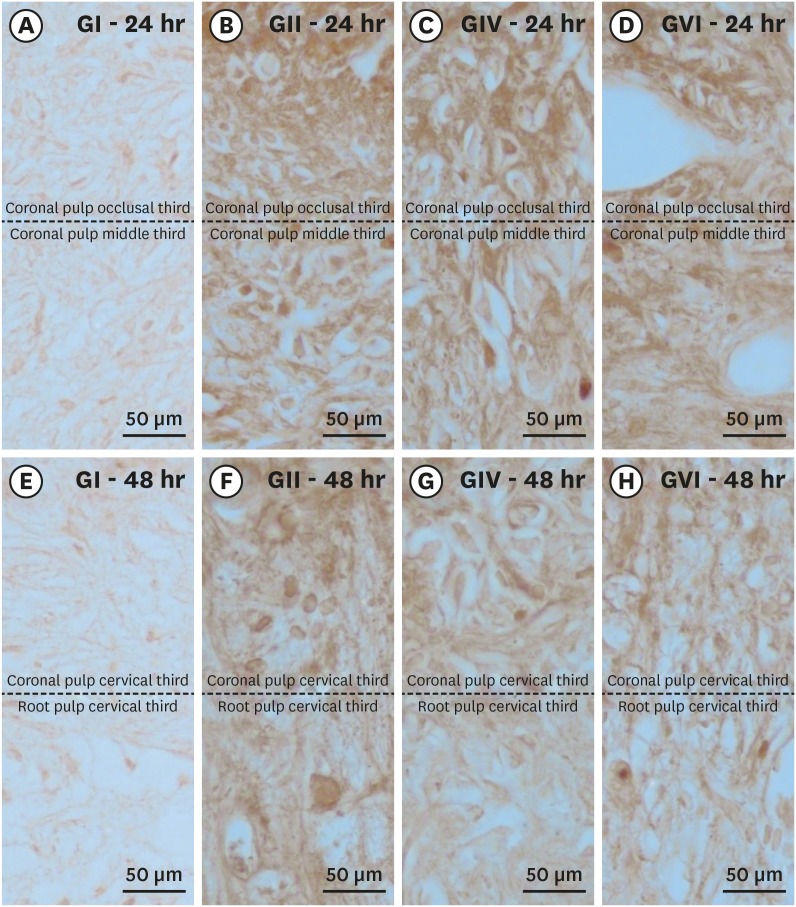 | Figure 3Histological sections showing immunostaining patterns for substance P. Photomicrographs showing the pattern of immunostaining for SP in the dental pulp in groups GI (A, E), GII (B, F), GIV (C, G) and GVI (D, H) after 24h (A–D) and 48h (E–H) local post treatment. It's possible observe the baseline level of SP expression in the control group and the significant increase in immunostaining for SP after bleaching therapy. Original magnification: ×1,000.
|
Table 2
Median scores from substance P immunostaining in each crown and radicular third for all bleaching groups
Six groups were divided as follows: GI, control; GII, boost 38%; GIII, control + ibuprofen; GIV, boost 38% + ibuprofen; GV, control + desensibilize; and GVI, boost 38% + desensibilize.
Means followed by different letters represent statistically significant differences (p < 0.05). Different lowercase letters indicate statistically significant differences between columns in the same rows, and uppercase letters indicate statistically significant differences between rows within the same column.
![]()
2. Immunohistochemical analysis of CGRP
Table 3 and Figure 4 show the scores from the immunohistochemical analysis of each coronary and root third of the bleaching groups. At 0 hours, the coronary thirds of the bleaching groups (GII, GIV, and GVI) presented areas of necrosis in all sections analyzed. This reflected a statistically significant difference from the control group (GI), which presented mild marking, but without the presence of necrotic areas. At 24 and 48 hours, only the GVI presented a low immunolabeling pattern in all thirds, reflecting a statistically significant difference from GII and GIV. Regarding the root thirds at 0 hours, GVI showed better results than GII and GIV, as it presented a low immunostaining pattern. At 24 hours, the occlusal thirds in all bleaching groups were similar to each other and presented a low immunostaining pattern, as was also observed in the middle and cervical thirds of GIV and GVI. At 48 hours, all groups were evenly matched in the root thirds, with a low immunostaining pattern.
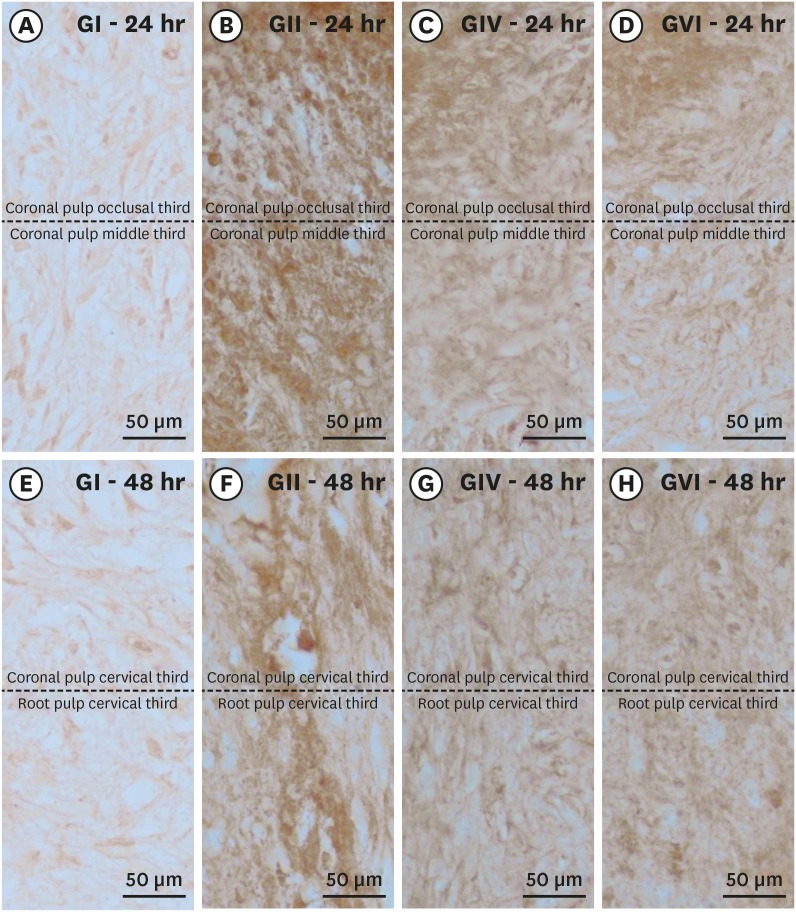 | Figure 4Histological sections showing the immunostaining pattern for calcitonin gene-related peptide. Photomicrographs showing the pattern of immunostaining for CGRP in the dental pulp in groups GI (A, E), GII (B, F), GIV (C, G) and GVI (D, H) after 24h (A–D) and 48h (E–H) after local treatment. It's possible observe the baseline level of CGRP expression in the control group and the significant increase in immunostaining for CGRP after bleaching therapy. Original magnification: ×1,000.
|
Table 3
Median scores from calcitonin gene-related peptide immunostaining in each crown and root third for all groups
Six groups were divided as follows: GI, control; GII, boost 38%; GIII, control + ibuprofen; GIV, boost 38% + ibuprofen; GV, control + desensibilize; and GVI, boost 38% + desensibilize.
Means followed by different letters represent statistically significant differences (p < 0.05). Different lowercase letters indicate statistically significant differences between columns in the same rows, and uppercase letters indicate statistically significant differences between rows within the same column.
![]()
Go to :
DISCUSSION
Bleaching treatment is considered to be a relatively safe procedure with proper dosage and indications. However, errors in either the execution or patient selection can seriously compromise the dental pulp, and bleaching protocols with high concentrations should therefore be avoided because of their potential impact on odontoblast cells [25]. Several in vitro studies have proven the potentially toxic effects of bleaching treatments [69], but few studies have investigated the effects of dental bleaching on dental pulp [26]. Thus, we used Wistar rats as an experimental model, because this model is both straightforward to investigate and can shed light on therapies that may reduce the inflammation caused by bleaching treatments [27].
7The histopathological analysis of the rat dental pulp subjected to the bleaching treatment using 38% hydrogen peroxide showed large areas of pulp necrosis, especially immediately after the procedure. Since dental structure and physiology are different in rats and humans [28], it is likely that the rat model favored a more intense penetration of hydrogen peroxide, causing changes in vascular permeability and consequently immediate dissolution of the pulp tissue [29]. In the 24- and 48-hour analyses after the bleaching procedure, a significant and gradual improvement in the inflammatory tissue was observed in the coronary portion. This directly reflects the recruitment of undifferentiated mesenchymal cells while maintaining tissue integrity (i.e., cellularization).
A study by Cintra et al. [30] showed a high occurrence of cell death at 48 hours post-treatment in a group subjected to 35% hydrogen peroxide bleaching for a single 45-minute session, with areas of intense inflammatory infiltrate, as well as hemorrhage, vasodilation, and disorganization of the odontoblastic layer. Those findings corroborate the results of our study, but a limitation of the above-mentioned study is that it only analyzed the 48-hour time point, leaving some doubts regarding the response at 0 and 24 hours after the bleaching treatment, which is when a higher occurrence of tooth sensitivity is reported. Therefore, our study provides insights into the pulp condition at shorter time intervals after treatment, confirming the aggressiveness and intensity of this in-office bleaching technique.
Substances such as topically applied desensitizing agents or drugs can be used to minimize the adverse effects reported by patients after bleaching. In the present study, ibuprofen was administered by gavage at 30 minutes and every 12 hours after the bleaching procedure, in the form of drops of a suspension. A histological analysis by Gallinari et al. [31] showed that using ibuprofen instead of a topical drug for this purpose was not very advantageous, because ibuprofen is more effective at the systemic level than at the local level [22].
The use of a topical desensitizer in the form of a low-viscosity gel, such as Desensibilize KF 2% (based on potassium nitrate and sodium fluoride) is another way to combat tooth sensitivity during and/or after bleaching treatment [32]. The statistical analyses conducted in our study showed that the animals that received a desensitizing agent presented a distinct pattern compared to the other groups.
The histological analysis also showed some inflammatory cells when a topical desensitizer was used, even immediately after the bleaching treatment, unlike all the other groups that underwent pulp necrosis treatment. In addition, the 24- and 48-hour analyses showed improvements in inflammatory conditions, which were mild and resembled the control group, unlike the other groups, further validating the effectiveness of a topical desensitizer as part of a bleaching protocol.
To evaluate the effect of the pain-relieving therapies, we also chose to analyze the levels of the neuropeptides SP and CGRP in the pulp tissue, as these neuropeptides play a role in the onset of pain signals from the area of tissue injury. The immunohistochemical analysis showed that ibuprofen had a significant effect on neuropeptide expression by influencing prostaglandin production. Consequently, ibuprofen led to decreased levels of pulp inflammation and neuropeptide release, which explains the similarity of the ibuprofen-treated group to the control group at 24 hours after the bleaching treatment.
Due to the large areas of necrosis at T0 in the group where a topical desensitizer was used, it was only possible to observe the immunostaining of the neuropeptides in the cell precipitates. This pattern was observed mainly in GII, which presented necrosis in all specimens of the coronary pulp. In the other groups, positive immunostaining was observed for both neuropeptides, which implies an exacerbated painful sensation when compared to healthy dental pulp tissue.
Together with the tissue regeneration that was observed within 24 hours after bleaching, positive immunostaining for both SP and CGRP was observed in all groups that received the bleaching treatment. However, the pulp samples from teeth that received the bleaching treatment showed higher expression levels of the neuropeptides than the groups that did not receive the bleaching therapy. This result is in agreement with a study by Caviedes-Bucheli et al. [33], who observed that both SP and CGRP appeared in all pulp samples, but at higher levels in inflamed pulp. According to the authors of that study, the increased levels of these neuropeptides (SP and CGRP) suggest that the neuronal regulation of pulp blood flow is controlled by primary afferent and sympathetic nerve fibers, in which these neuropeptides are located.
In the same context, Awawdeh et al. [34] analyzed the expression of SP and CGRP, in addition to neurokinin A, in human tooth pulp tissue that was healthy or had a painful sensation, and observed that in symptomatically painful pulp tissue, neuropeptide levels were higher than in healthy pulp tissue, further corroborating the results obtained in this study. In that study, the authors suggested that the increased neuropeptide levels were due to the peptide afferent nerve fibers in the dental pulp, which play an active and important role in the overall response to cell damage in addition to conducting impulses to the central nervous system.
When an inflammatory process occurs in the pulp, as takes place in response to the application of high-concentration whitening gels, edema and increased intrapulpal pressure stimulate the release of neuropeptides related to the transmission of nociceptive information [7], stimulating the production of inflammatory mediators and increasing inflammation [835]. Some of these neuropeptides remain stored in vesicles at nerve endings and are released in response to various stimuli, thereby intensifying the inflammatory process and feedback inflammation. However, because desensitizing agents block nerve transmission, we observed that their use can have positive effects by decreasing the inflammation and the expression of pain-related neuropeptides, minimizing the pain caused by the bleaching treatment.
In a clinical study, Rahal et al. [36] analyzed tooth sensitivity during in-office bleaching and after desensitizing agent treatment and found that the use of topical desensitization was effective in reversing the dental cold sensation thresholds caused by highly concentrated peroxides. The reduction in pain sensitivity may have been due to the mechanism of action of the desensitizing agent, which sealed the dentinal tubules and thereby promoted lower sensitization of the pulp tissue cells, reducing the amount of inflammatory mediators. These mediators are responsible for the exacerbated and persistent painful sensitization that is associated with the use of high concentrations of hydrogen peroxide, which is why reducing their levels has a beneficial effect [37].
Based on the results of the present study, it can be concluded that the use of ibuprofen and Desensibilize KF 2% had positive effects, as they did not produce any adverse effect on the pulp tissue, which maintained a normal condition similar to that observed in the control group. This shows that the negative effects were undoubtedly due to the application of the bleaching agent on the dental surface [37].
Although the present study has some limitations regarding the use of rats as an experimental model due to differences in the morphological and biological responses of rat teeth compared to human teeth, the results nonetheless show that this type of bleaching treatment can cause serious damage to the pulp tissue. However, when performed under professional care, with the correct indications, and with proper execution, the use of topically applied desensitizing agents can minimize the adverse effects resulting from bleaching treatment.
Go to :
 XML Download
XML Download