

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Nickel-titanium (NiTi) rotary files are now widely used for the cleaning and shaping of the root canal system. The inherent characteristics of the NiTi alloy of superelasticity and resistance to torsional failure have allowed clinicians to efficiently obtain predictable results with nonsurgical endodontic treatment [12]. One of the most dreaded complications of the use of NiTi files is separation of the instrument during use, which can cause further procedural errors in endodontic therapy.
The incidence of fractured rotary NiTi files, based on only a small number of recent investigations, has been shown to be in the range of 0.4% to 4.6% [345]. Any case with a separated instrument inside the root canal can be managed with either an orthograde or a surgical approach. Possible orthograde approaches include an attempt to either remove or bypass the instrument or, alternatively, to prepare and obturate to the fractured fragment. Significant advances have been made in this field with regard to the use of various devices, techniques, and methods. In particular, the use of a microscope along with an ultrasonic device has proven to be an effective and comparatively safe method for the removal of separated instruments [67]. The advantage of an ultrasonic instrument is its ability to vibrate the obstruction loose while causing minimal damage to the canal wall. However, ultrasonic techniques are time-consuming and have been demonstrated to have only moderate success.
In a recent meta-analysis [8], it was concluded that randomized controlled clinical trials were required to substantiate the limited available evidence in support of either maintaining or changing the current practice regarding separated instruments. No consensus has yet been reached on the optimal approach for the management of such cases. Nevertheless, when a clinician encounters a separated instrument within a root canal, a full understanding of the management options and related factors is essential.
A recently-developed file removal system, the Terauchi file retrieval kit (TFRK) (Dental Engineering Laboratories, Santa Barbara, CA, USA), has been claimed to minimize the amount of dentin removal and the time required to remove a separated instrument [9]. However, little information is available regarding the efficacy of this system compared with other ultrasonic devices. Therefore, the present study was an attempt to compare the effectiveness of this new retrieval kit with ultrasonic tips in the removal of separated instruments from the root canal.
Go to : 
MATERIALS AND METHODS
The present study was conducted at the Department of Conservative Dentistry and Endodontics at the Maulana Azad Institute of Dental Sciences in Delhi, India. Eighty extracted human first mandibular molars with moderate root canal curvature (as determined by the Schneider method) [10] and closed apices were collected. The study was approved by the ethical committee of the institute. Consent was obtained from the patients regarding the use of their extracted teeth for scientific research. All extracted teeth were initially stored in chlorhexidine after extraction and were continuously hydrated throughout the experimental procedures. The mesial roots were selected and examined for pre-existing cracks with an operating microscope (Carl Zeiss Meditech AG, Jena, Germany) at ×21 magnification. The teeth were radiographed preoperatively to exclude any tooth that had previously been subjected to root canal treatment or that demonstrated any pathological and/or iatrogenic complications such as resorption, complete obliteration, or perforation.
Conventional access preparations were then made under the operating microscope using a cavity access set (Dentsply-Maillefer, Ballaigues, Switzerland). The pulp tissue remnants were removed, and patency was established in the mesiobuccal canals using a size 10/15 K-file (Dentsply-Maillefer). Engine-driven ProTaper rotary NiTi files (Dentsply Maillefer) were selected as instruments for this study. Orifice shapers (ProTaper Sx, Dentsply-Maillefer) were used to widen the orifice openings of the respective canals. The teeth were divided into 2 groups of 40 teeth each based on the instrument kit to be used for instrument removal: the P group, constituting the group treated using ProUltra tips (Dentsply Tulsa Dental Specialties, Johnson City, TN, USA) and the T group, representing the group treated using TFRK. Based on the level at which the instrument was fractured in the canal, each group was further subdivided into 2 smaller groups of 20 teeth each, according to whether the ProTaper F1 rotary instruments were fractured in either the coronal third (C, constituting the PC and TC groups) or the middle third (M, constituting the PM and TM groups). These instruments were notched 4 mm from the tip with a high-speed diamond disk to a depth of one-half of the instrument thickness to facilitate their fracture in the root canal (Figure 1).
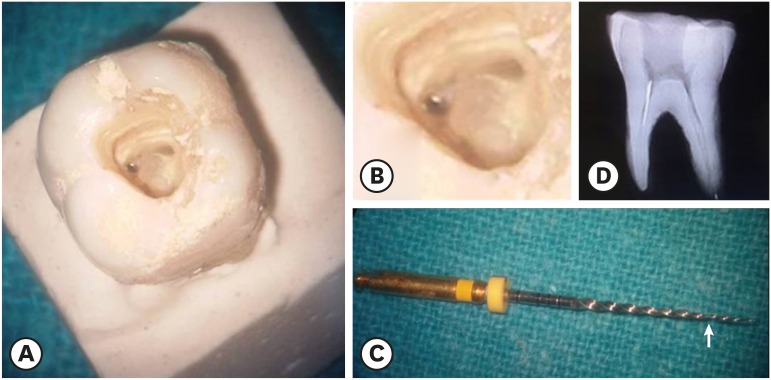 | Figure 1(A) Separated instrument in the coronal third of the mesiobuccal canal. (B) Magnified view of Figure 1A. (C) The arrow shows the separated portion of the ProTaper F1 rotary file. (D) Radiograph showing an instrument in the coronal third of the canal.
|
Instrument retrieval was performed using ProUltra tips in group P and TFRK in group T. The removal process was initiated with the formation of a staging platform using a modified Gates-Glidden drill (Mani Inc., Kiyohara, Tochigi, Japan). Successful removal was defined as complete removal of the fractured NiTi fragment from the root canal without creating a root perforation. The allotted instrument removal time was set as 60 minutes, a reasonable chair-side time. Time was recorded from the start of staging platform preparation until the instrument was either successfully removed (within 60 minutes) or, in cases of failure, until the attempts to do so were halted for any reason, such as perforation, a lack of visualization of the fractured instrument as a result of dislocation or secondary fracture, or the inability to grip the fractured fragment. Statistical analysis included the application of descriptive statistics and the unpaired t-test, with p-values of less than 0.05 indicating statistical significance.
Go to :
RESULTS
In total, 74 out of 80 fractured instruments were removed, corresponding to an overall success rate of 92.5%. When instrument removal was performed using the ultrasonic tips (group P), the overall success rate was 90%, whereas the success rate was 95% when instrument removal was performed using the TFRK (group T) (p > 0.05). Furthermore, when the success rate was investigated according to location, it was observed that all fragments fractured in the coronal thirds of the canals were successfully removed in both groups. The use of ultrasonic tips led to the successful removal of 16 of 20 instruments (80%) from the middle third of the canal, whereas the use of the TFRK led to the removal of 18 of 20 instruments (90%) from that region (p > 0.05).
It should be noted that in 3 of the 4 failed attempts in group P, the reason for failure was a secondary fracture of the broken fragment; in the fourth, the time limit was reached. In group T, there were 2 failed attempts: 1 due to secondary fracture and 1 due to reaching the time limit.
With regard to efficiency, the mean time for instrument removal from the coronal third was higher (17.9 minutes) when the ultrasonic tips were used than when the TFRK (15.3 minutes) was utilized (p > 0.05). Similarly, for removal from the middle third, the mean time required to retrieve the instrument was slightly higher in group P (46.4 minutes) than in group T (44.2 minutes). However, the difference was not found to be statistically significant (Table 1) (p > 0.05). Additionally, instrument removal from the middle third of the root canal required a significantly longer time than removal from the coronal third in both group P and group T (Table 2) (p < 0.05).
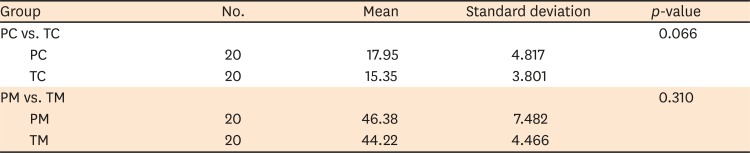
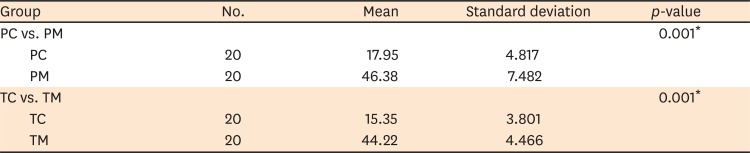
Table 1
Intergroup comparison of the time (in minutes) taken for instrument retrieval (p > 0.05)
| Group | No. | Mean | Standard deviation | p-value | |
|---|---|---|---|---|---|
| PC vs. TC | 0.066 | ||||
| PC | 20 | 17.95 | 4.817 | ||
| TC | 20 | 15.35 | 3.801 | ||
| PM vs. TM | 0.310 | ||||
| PM | 20 | 46.38 | 7.482 | ||
| TM | 20 | 44.22 | 4.466 | ||
PC, ProUltra tips and coronal third; TC, Terauchi file retrieval kit and coronal third; PM, ProUltra tips and middle third; TM, Terauchi file retrieval kit and middle third.
![]()
Table 2
Intragroup comparison of the time (in minutes) taken for instrument retrieval (p < 0.05)
| Group | No. | Mean | Standard deviation | p-value | |
|---|---|---|---|---|---|
| PC vs. PM | 0.001* | ||||
| PC | 20 | 17.95 | 4.817 | ||
| PM | 20 | 46.38 | 7.482 | ||
| TC vs. TM | 0.001* | ||||
| TC | 20 | 15.35 | 3.801 | ||
| TM | 20 | 44.22 | 4.466 | ||
PC, ProUltra tips and coronal third; TC, Terauchi file retrieval kit and coronal third; PM, ProUltra tips and middle third; TM, Terauchi file retrieval kit and middle third.
*Statistical significance was determined at p < 0.05.
![]()
Go to :
DISCUSSION
Management of a separated instrument in the root canal is both a challenging task and an important factor in the long-term prognosis of endodontic treatment. In such cases, removal of the instrument is considered to be a preferred option over leaving it in the canal [11]. Only after removal of the fractured instrument can the root canal be optimally negotiated, cleaned, and shaped. For the removal of separated instruments, many techniques and devices have been described, including chemical solvents [1213], Stieglitz forceps [14], wire loops [15], hypodermic surgical needles [1617], braiding of endodontic files [6], Masserann instruments [1819], extractors [20], Canal Finder systems [21], lasers [2223], electrochemical procedures [24], and ultrasonic techniques [112526]. All of these devices and methods have advantages and disadvantages. Various studies have been conducted to assess the success rate of ultrasonic techniques in removing fractured instruments, and based on the results, the majority of those studies advocate the use of ultrasonic tips for this purpose [2728].
Excessive instrumentation of the root canal and associated dentin removal are known to increase the chances of tooth fracture [29]. For this reason, when a fractured instrument is removed from the canal, the potential loss of dentin must be taken into account. Therefore, ultrasonic tips are preferred over other systems, as they involve less loss of tooth structure [30]. However, it has been observed that a substantial amount of guttering around the fragment is required. Therefore, even after the fragment is disengaged from the canal wall, it keeps swaying in the canal and does not exit easily. In such cases, further instrumentation may compromise the integrity of the tooth and increase the risk of perforation. Hence, it was desirable to develop a technique whereby after the coronal part of the fragment is exposed, it could be grasped by a device and removed. A new file system developed by Terauchi et al. [9] contains a loop device in addition to the ultrasonic tips. The system also contains a modified Gates-Glidden bur for use in preparing a staging platform. In addition, it includes a trephine bur to make a trough around the shank end of the broken file if needed, as well as a microexplorer with an extremely fine tip to explore the canal for broken files and impediments. Under this system, it has been claimed that if the fractured fragment does not exit even after 0.7 mm of coronal exposure, it can be grasped in the loop device and retrieved without further canal enlargement [9]. Moreover, this technique does not require the separated instrument to be fully upright for its removal, thereby facilitating instrument retrieval from the curved portion of the canal.
The present study compared the effectiveness, in terms of time required, of this new system with that of an existing ultrasonic device in removing separated instruments from the root canal. The time required for instrument retrieval was found to be higher for group P than for group T. However, the difference was not statistically significant. This can be attributed to the fact that in both groups, the majority of files could be removed with ultrasonic vibration only. In the situations where the loop device was used, the insertion of the loop on the coronal end of the fragment involved a considerable amount of time. As the loop is composed of 0.08-mm NiTi wire, it is very fragile and requires substantial practice and dexterity to avoid its rupture. The available data suggest that for broken file removal performed using different systems, the time required for ultrasonic techniques varied from 3 to 40 minutes, while using the ultrasonic tips with the loop device took only 4 to 7 minutes [931]. This may be due to the fact that these cases were treated by experts who had years of experience handling the loop device and the associated tips.
Furthermore, intragroup comparisons showed that the instrument retrieval time was higher for the middle third than for the coronal third in both groups, and the difference was statistically significant. This can be explained by the poor accessibility and limited visibility in the region of the middle third, in agreement with previously documented data [631].
The allotted instrument removal time was set as 60 minutes to provide adequate time for the use of each system. Suter et al. [6] recommended a time slot of 45 to 60 minutes for removing the fractured fragments due to the possibility that the success rate might drop with increasing treatment time due to operator fatigue, secondary fracture, or excessive removal of dentin leading to fracture or perforation.
During the application of these 2 systems for fractured rotary file removal, the only procedural error observed was a secondary fracture of the file fragment, which can be prevented by carefully guttering around the tip of the fragment without touching it with the ultrasonic tip. The occurrence of this error was more prevalent when the ultrasonic tips were used than when the TFRK was utilized. This may be due to the transfer of excessive ultrasonic vibrations to the separated fragment.
Go to :
CONCLUSIONS
Under the conditions of this in vitro study, both ProUltra tips and the TFRK were successful in removing the majority of the fractured files from root canals, with success rates of 90% and 95%, respectively. Although the TFRK performed marginally better, further studies on larger sample sizes are needed to substantiate this finding. Both systems are excellent clinical tools for instrument retrieval, but the loop device in TFRK requires slightly more dexterity than the ProUltra tips.
Go to :
 XML Download
XML Download