

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Important biological functions, including physiological, cognition, and cardiovascular system processes [1] occur during sleep, yet more than 27% of adults worldwide suffer from sleep disorders, including difficulty in initiating and/or maintaining sleep [2]. The Korean National Health Insurance Corporation has reported an increasing trend in sleep disorders (disease code: G47) among young adults. Many studies have reported that poor sleep quality and reduced sleep time are related to a decline in overall quality of life and increased risk for further cardiovascular events [3]. As such, sleep itself is considered essential for overall quality of life and cardiovascular health. However, several studies rely upon subjective sleep surveys to investigate nocturnal profiles or intervention effectiveness, despite the fact that self-reported questionnaires introduce method bias that undermines their scientific validity [4]. Objective sleep assessments, in addition to self-reported surveys, are thereby necessary for an accurate sleep health evaluation.
The actigraph is a wearable device with a triaxial accelerometer and is widely used to evaluate sleep/wake cycles. Although polysomnography (pSG) is the predominant tool for diagnosing sleep disorders, it is challenging to use in research settings due to complicated and time-consuming procedures and the need for resource intensive data analysis [5]. A previous study monitored sleep patterns with an actigraph to uncover relationships between sleep and perceived quality of life and concluded that improvement of sleep parameters as detected by actigraph was accompanied by enhanced perceived quality of life [6].
Sleep deprivation is associated with increased cardiovascular disorder (CVD) risk. The Monitoring Project on Risk Factors and Chronic Diseases in the Netherlands study conducted 10–15 yrs of research on 20,432 healthy adults (age 20–65 yrs) without any pathological disorders, and found that people with shorter sleep durations or poorer sleep quality were at greater risk for developing CVD [7]. Cardiac autonomic imbalance due to sleep disorders is associated with CVD incidence [8]. A reduction in vagal tone, including a decrease in parasympathetic activity during sleep, has also been associated with increased morbidity and mortality in CVD [9]. A recent study monitoring chronic fatigue syndrome (CFS) patients with poor sleep quality using heart rate variability (HRV) revealed that these patients demonstrated decreased vagal activity during nighttime sleep, suggesting the HRV index could be a significant predictor of cardiac autonomic imbalance caused by disrupted sleep [10]. As such, when assessing health problems related to sleep disorders, nocturnal HRV indices of cardiac autonomic regulation may provide critical information.
The recent intervention trial has examined alternative strategies such as nutritional [1112] therapies to improve nighttime sleep. Nutritional therapy for induction of sleep could be used long-term without side effects and represents a potential alternative approach for sleep improvement [11]. However, many nutrition-related sleep studies were dependent on self-reporting of the effectiveness of interventions [13]. It remains unknown whether nutritional treatment can improve sleep quality or affect nocturnal HRV indices of cardiac autonomic regulation. New methods are thereby needed to evaluate the effects of sleep-inducing nutritional interventions, a need underscored by the rapid increase of sleep disorders and the relation of long-term sleep disorders to future CVD [23]. We have hypothesized that sleep-inducing juice which was made up of natural extracts will provide positive effects on sleep quality and enhance cardiac autonomic regulation for better-quality in sleep. To examine this hypothesis, the present study was performed to verify effectiveness of sleep-inducing juice composed of natural extracts on sleep quality and to examine whether an intervention to enhance sleep has influenced on HRV in adults who are suffering from sleep deprivation.
Go to : 
SUBJECTS AND METHODS
Subjects
A total of 44 adults complaining of sleep difficulty were recruited for this study. Twelve subjects who did not meet the inclusion criteria were excluded. Inclusion criteria were over 18 yrs of age; difficulty in initiating or sustaining normal nighttime sleep, as evidenced by a score of at least 5 on the Pittsburgh sleep quality index (PSQI); freedom from overt cardiovascular, metabolic (body mass index [BMI] ≥ 30), and/or neurological disorders; a sedentary lifestyle for at least 12 months before the study; no history of sleep-inducing medication use; and no use of prescription medications and/or illicit drugs affecting cardiac autonomic nerve regulation.
Participants of this study were recruited 2 ways. Firstly, we have explained the benefits of applying to join this study using a web bulletin board of Kyungpook National University, from April to May, 2017. And then all volunteers who want to take part in the current study were recruited by telephone counseling. Secondly, we had selected employees who are suffering from sleep deprivation in South Gyeongsang Province-based Hurom Corporation. After selection of experimental subjects who meet the requirements of inclusion criteria for this study through self-reported questionnaire and interviews, order and procedure for each session were designed. The first session was conducted from May to July, 2017. And then second session was carried out from July to September, 2017, following the 2-week washout period. After a comprehensive examination, 32 men and women were enrolled in the study (Fig. 1). The clinical characteristics of the participants are presented in Table 1. After being informed of the experimental procedures, all participants provided written informed consent indicating voluntary participation before beginning the study. This study was approved by the Kyungpook National University Life Science Ethics Committee (IRB: 2017-0033).
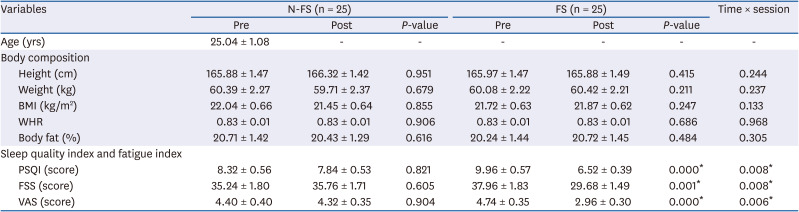
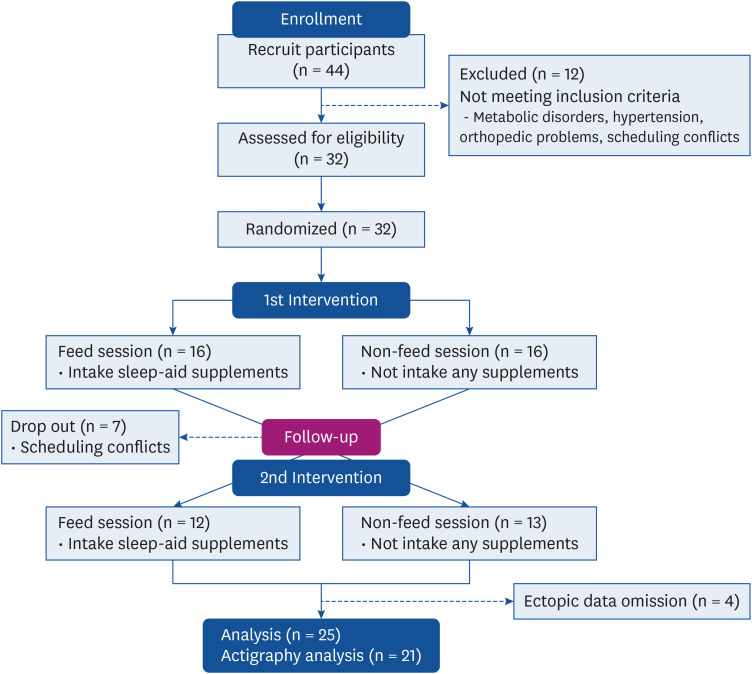
Table 1
Changes in characteristics of subjects and questionnaire scores
Values are mean ± SEM. P-values calculated by Wilcoxon's signed-rank test. Time × session values calculated by repeated measure.
N-FS, non-feeding session; FS, feeding session; BMI, body mass index; WHR, waist-to-hip ratio; PSQI, Pittsburgh sleep quality index; FSS, fatigue severity scale; VAS, visual analog scale; SEM, standard error of mean.
*P < 0.05.
![]()
Trial protocol
An unblinded randomized crossover trial consisting of 8 weeks with (feeding sessions [FS]) or without (non-FS [N-FS]) sleep-inducing juice supplementation, a 2-week wash-out period, and then another 8 weeks in the other (N-FS or FS) group, was conducted. FS received sleep-inducing juice (250 mL/trial) developed from natural ingredients twice per day (morning and afternoon, respectively) for 8 weeks while maintaining their usual lifestyle and diet. Because of relatively a short expiration period of sleep-inducing juice used in the current study, we had to visit at least every 3 days to the home of all subject to supply it. For this reason, whenever we have visited their home, we were allowed to review daily life activities and dietary intake for each subject. In particular, when participants have visited the laboratory due to nocturnal HRV assessment and actigraphy monitoring for 7 consecutive days, we tried more detailed interviews to find whether daily life patterns were altered. None has been reported any marked alteration for daily life patterns, including dietary intake throughout all experimental sessions (data not shown).
For at least 48 hours prior to physical examination at pre- and post- intervention, we instructed all subjects to abstain from strenuous physical activity and intake of alcoholic or caffeinated beverages. After overnight fasting, all subjects visited the laboratory between 9 A.M. and 12 P.M., to exclude circadian variation effects, followed by measurements of anthropometric and hemodynamic indices and HRV, and completion of subjective sleep quality and fatigue surveys (Fig. 2).
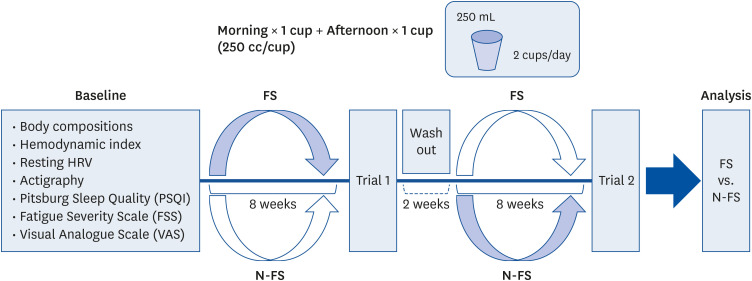
Objective sleep parameters were obtained by asking participants to wear the ActiGraph GT3X (Actigraph, LLC., Pensacola, FL, USA) during sleep along with recording their sleep daily in a diary for 7 days before and after the intervention. Nocturnal RR intervals were collected by Polar RS800CX (polar® Electro Őy, Kemple, Finland) over a single night along with objective sleep evaluation to assess the effects of sleep-inducing juice on cardiac autonomic regulation. Subjects received a comprehensive demonstration and explanation of proper use of these devices to wear at home, and proper use was verified prior to embarking on the study. Experimental procedures are described below (Fig. 2).
Interventions
Sleep-inducing ingredients were obtained as follows: lettuce (Lactuca sativa L.) was supplied by Jeonnam Agricultural Research and Extension Services in Naju, Korea. Oranges, pineapples, and frozen cherries were purchased from a local market. The lettuce, orange, pineapple and frozen cherry were extracted with a vertical-type low-speed masticating juicer (HWS-SBF18; Hurom Co., Ltd., Gimhae, Korea) at a ratio of 28, 44, 14 and 14% respectively. The extracted juice was mixed with 0.1% dried bonnet bellflower and 250 mL of juice placed in a bottle for high pressure sterilization at 550 MPa for 60 s (QFP 350L; Avure Technologies, Kent, WA, USA). Extraction and processing details, such as blending technique, are proprietary and confidential per the manufacturer's instructions.
Anthropometry and hemodynamics
Height and weight were measured to the nearest 0.1 cm and 0.01 kg using an automatic digital stadiometer (DS-102; JENIX Co., Seoul, Korea) and a digital electronic weighing scale (GS 36; Beurer GmBH & Co., Ulm, Germany), respectively. BMI was calculated by dividing weight by height squared (kg/m2). Waist-to-hip ratio was calculated from waist circumference divided by that of the hips. In accordance with the American College of Sports Medicine guidelines [14], body density was calculated by Jackson and Pollock equation following skinfold measurements of 3 sites with caliper (Dynatronics Corp., Salt Lake City, UT, USA) and body fat percentages were estimated by Siri equation. Participants remained in a seated position for 20 min or more, after which systolic blood pressure (SBP), diastolic blood pressure (DBP), and mean heart rate were obtained on their non-dominant arm using a BP monitor (BM 16; Beurer GmBH & Co.). Mean arterial pressure was estimated as follows: [(2 × DBP) + SBP]/3.
Subjective sleep quality and fatigue assessments
The PSQI is a 24-item questionnaire designed for participants to self-evaluate their sleep/wake patterns across 7 different components: subjective sleep quality, sleep latency (SL), sleep duration, habitual sleep efficiency (SE), sleep disturbances, use of sleeping medication, and daytime dysfunction [15]. Each dimension is scored on a Likert-type scale from 0 to 3, with 0 representing normal, and 3 representing extremely disrupted. Global PSQI scores range from 0 to 21. A score of at least 5 indicates a poor sleeper who suffers from serious difficulties in 2 domains or moderate difficulties in 3 domains of sleep. In addition, the Pittsburgh sleep diary consists of bedtime and wake-time sections [16]. Subjects were instructed to complete the both every day when they wore the actigraph. Bedtime questionnaires involved timing of breakfast, lunch and dinner; caffeine, alcohol and tobacco product consumption; use of prescribed and over-the-counter medications; and timing and duration of daytime exercise and naps. Wake-time questionnaires contained timing of going to bed, turning out lights, minutes to sleep onset; final wake-time, method of final waking; incidence, duration, and reasons for wake after sleep onset (WASO); and subjective quality of sleep episode, mood on awakening (tense vs. calm), and alertness on awakening, marked on 10 cm visual analogue scale (VAS). The 9-item fatigue severity scale (FSS) and VAS scores were combined to assess the subjective intensity of fatigue on functional and behavioral aspects of daily life [17]. The Korean version of the FSS presented a high internal consistency (Cronbach's α = 0.93), and the item-total correlation ranged from 0.56 to 0.90 [18]. Each item was expressed on a scale from 1 (strongly disagree) to 7 (strongly agree). Possible scoring range was 9 to 63, with higher scores (≥ 36) reflecting greater levels of fatigue. The 10 cm VAS was also quantified and contributed to calculations of overall fatigue status.
HRV analysis
We evaluated resting and nocturnal cardiac autonomic regulation through HRV, measured at 1,000 Hz by Polar RS800CX (polar® Electro Őy), which records normal-to-normal RR intervals from a wireless chest strap (2-lead) heart rate monitor. Raw data were extracted as a text file (.hrm) by Pro-trainer Polar 5 software (version 5.40.171; polar® Electro Őy) and then imported into HRV analysis software (Kubios HRV version 2.1, 2012; Biosignal Analysis and Medical Imaging Group, University of Kuopio, Kuopio, Finland, MATLAB). Prior to HRV analysis, ectopic beats were excluded by artifact correction. Following a standardized short-term protocol (5 min), a series of RR intervals at 256 points/Hz were selected and re-extracted via detrended method using smoothness priors (λ/500) technique [19]. Presently, a standardized protocol for nocturnal HRV analysis during sleep has not been established. However, previous studies have proposed recording starting one hour after going to bed [2021]. Considering the shortest duration of sleep among study participants, nocturnal cardiac autonomic regulation was evaluated over a 240 min period at least one hour after bedtime. Time-course changes of HRV indices during sleep were assessed by dividing total sleep periods into 30 min intervals (60, 90, 120, 150, 180, 210, and 240 min after sleep). We computed time, frequency, and nonlinear indices using the first 5 min of each period. Time domain index, square root of the mean squared differences between successive RR intervals (rMSSD), and NN50 divided by the total number of RR intervals, which reflect vagal activity, were calculated. Low frequency (0.04–0.15 Hz) and high frequency (HF; 0.15–0.4 Hz) values were extracted via power spectrum density analysis by fast Fourier transform method [22]. Nonlinear techniques have increased in importance in recent studies because non-invasive bio-signals commonly present with non-stationary characteristics. A Poincaré plot applicable to short-term HRV measures schematized the association between continuous RR intervals. This plot is derived from a nonlinear index such as SD of the instantaneous beat-to-beat variability of data (SD1), or deviation of instantaneous RR interval variability by short diameter of ellipse, and transverse axis.
Actigraphy
Objective parameters of the nighttime sleep pattern were assessed by an ActiGraph GT3X+ (ActiGraph, LLC.) equipped with a triaxial accelerometer. All patients were instructed to secure the wristwatch actigraph (4.6 × 3.3 × 1.5 cm, 19 g) on their non-dominant wrist before bedtime over 7 consecutive days (6 nights) to assess nocturnal sleep quality. The following objective sleep parameters were taken: SL, total counts (TC) of movement, SE, sleep fragmentation index (SFI), total sleep time (TST), WASO, number of awakenings, average awakening length, movement index (MI), and fragmentation index. Raw actigraph data stored as digitized computer data were analyzed by ActiLife version 6.9.2 software (ActiGraph, LLC.), wherein the actigraph accelerometer was initialized to collect data and automatically scored sleep in 60 s epochs at 80 Hz [23]. The Sadeh algorithm previously validated on a sample of young adults, was used to calculate objective sleep measures [24]. Validity and reliability were improved by analyzing 4 days, with the 2 least reliable days excluded.
Statistical analysis
Data were analyzed using descriptive statistics performed by SPSS 25.0 (SPSS software; IBM Corp., IL, USA). All variables are represented as mean ± standard error of the mean. The Shapiro-Wilk test was used to assess the normality of the distribution. Changes in independent variables pre- and post-intervention were examined by Wilcoxon signed-rank test for each session. Finally, repeated measurement of variance analysis was conducted to identify potential interaction effects between time and sessions. Significance was set at α = 0.05.
Go to :
RESULTS
Seven participants with scheduling conflicts dropped out of the second trial after the 2-week wash out following the first trial. In the second trial, there were twelve participants in FS, and thirteen participants in N-FS. In addition, 4 participants were excluded from the objective sleep assessment due to missing actigraph recording data. As a result, the present study analyzed 25 participants, but only 21 participants included an analysis of actigraphy data.
Anthropometrics and hemodynamic indices
Measured variables demonstrated no significant differences between baselines for the 2 sessions (P > 0.05; data not shown). No statistical differences in resting blood pressure (data not shown) and body composition (P > 0.05, Table 1) were associated with either group.
Subjective sleep quality and fatigue index
There were no differences between sessions for baseline subjective measures of sleep quality and perceived fatigue. However, self-reported PSQI and FSS scores, including VAS were significantly decreased after FS (P < 0.01, Table 1), while no significant differences in these values were observed for N-FS (P > 0.05, Table 1). Significant session × time period interaction effects were observed on subjective measures of sleep quality and perceived fatigue (PSQI and FSS scores with VAS, P < 0.01; respectively).
Resting and nocturnal cardiac autonomic regulation
There were no significant differences between sessions for resting HRV indices such as time, frequency, domain, and nonlinear parameters in baseline levels (P > 0.05; data not shown). However, resting HF component reflecting vagal tone was significantly increased in FS, while that of N-FS were not statistically different (P < 0.05, Table 2). A significant session × time period interaction effect was observed on HF at rest (P < 0.05, Table 2).
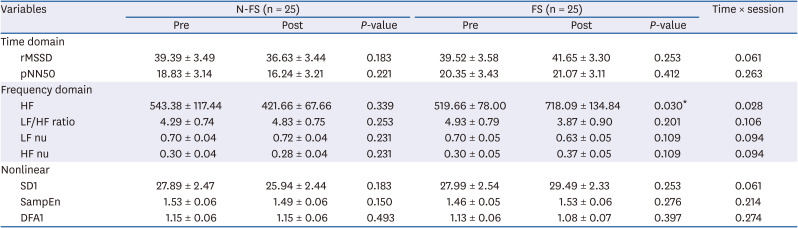
Table 2
Changes in resting heart rate variability parameters
Values are means ± SEM. P-values are calculated by Wilcoxon's signed-rank test.
N-FS, non-feeding session; FS, feeding session; rMSSD, square root of the mean squared differences between successive RR intervals; pNN50, NN50 (number of successive RR interval pairs that differ more than 50 ms) divided by the total number of RR interval; HF, high frequency(0.15–0.4 Hz); LF/HF ratio, ratio between low frequency (0.04–0.15 Hz) and high frequency; LF nu, low frequency normalized unit; HF nu, high frequency normalized unit; SD1, SD of the instantaneous beat-to-beat variability of data; SampEn, sample entropy; DFA1, detrended fluctuation analysis index alpha1 short term fractal scaling exponent; SEM, standard error of mean.
*P < 0.05.
![]()
Nocturnal HRV indices had no baseline statistical differences between sessions (P > 0.05; data not shown). However, enhanced vagal activity accompanied by sympathetic withdrawal during sleep were found after sleep-inducing juice intake. We calculated nocturnal HRV indices to assess cardiac autonomic regulation during sleep over a total of 7 periods (60, 90, 120, 150, 180, 210, and 240 min).
Results of this study indicated that the HRV indices of vagal activity rMSSD, HF, and SD1 were increased (P < 0.05; all 3) following sleep-inducing juice intake at 210 min during sleep (Table 3); those of the N-FS did not show significant differences in total periods of nocturnal cardiac autonomic regulation (data not shown). Significant session × time period interaction effects on HRV indices reflecting vagal activity at 210 min during sleep were also observed (rMSSD, HF, and SD1, P < 0.05; all 3).
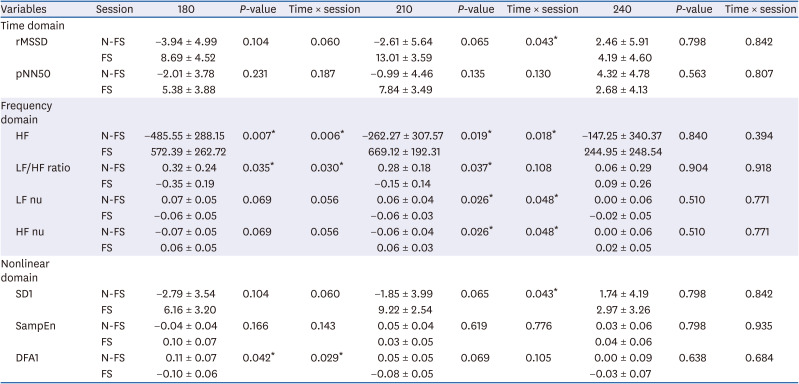
Table 3
Changes in nocturnal heart rate variability parameters
Values are means ± SEM. P-values are calculated by Wilcoxon's signed-rank test.
rMSSD, square root of the mean squared differences between successive RR intervals; pNN50, NN50 (number of successive RR interval pairs that differ more than 50 ms) divided by the total number of RR interval; N-FS, non-feeding session; FS, feeding session; HF, high frequency (0.15–0.4 Hz); LF/HF ratio, ratio between low frequency (0.04–0.15 Hz) and high frequency; LF nu, low frequency normalized unit; HF nu, high frequency normalized unit; SD1, SD of the instantaneous beat-to-beat variability of data; SampEn, smaple entropy; DFA1, detrended fluctuation analysis index alpha1 short term fractal scaling exponent; SEM, standard error of mean.
*P < 0.05.
![]()
Objective sleep quality
There were no significant differences between sessions for baseline objective measures of sleep quality (data not shown). However, TST was statistically increased over baseline in FS (P < 0.05), while that of N-FS tended to decrease compared to baseline (Table 4). In contrast, MI was significantly decreased in FS from baseline (P < 0.05), while that of N-FS tended to increase compared to baseline (Table 4). Significant session × time period interaction effects on TST and MI were also observed (TST and MI, P < 0.01; respectively).

Table 4
Changes in objective sleep quality index
Values are means ± SEM. P-values calculated by Wilcoxon's signed-rank test.
N-FS, non-feeding session; FS, feeding session TST, total sleep time; WASO, wake after sleep onset; NOA, number of awakenings; AAL, average awakening length; MI, movement index; FI, fragmentation index; SEM, standard error of mean.
**P < 0.01.
![]()
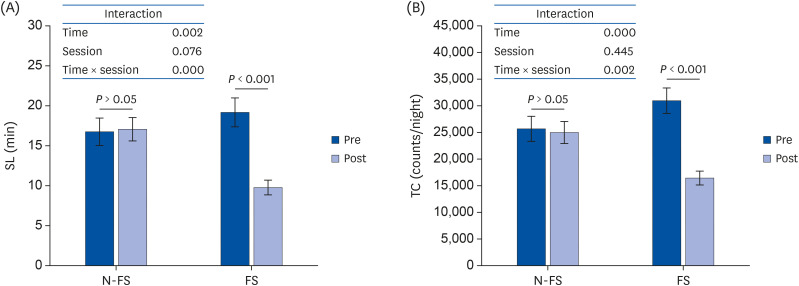
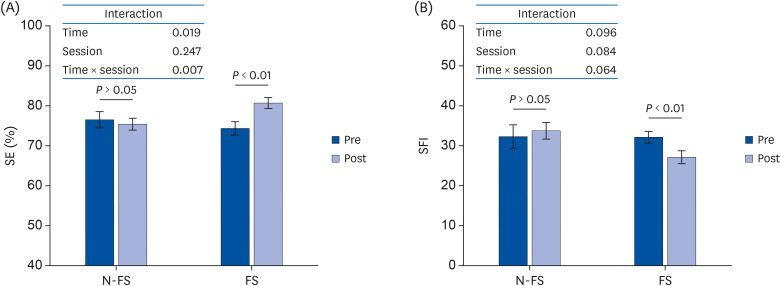
SL, TC, and SFI were significantly increased over baseline in FS (P < 0.01), while values for N-FS showed no significant differences compared to baseline (Fig. 3). Significant session × time period interaction effects on SL and TC were also observed (SL and TC, P < 0.01; respectively). SFI did not have a statistically significant interaction effect (P > 0.05, Fig. 3). SE was statistically increased over baseline in FS (P < 0.01), while that of N-FS tended to decrease compared to baseline (Fig. 4). A significant session × time period interaction effect was also observed for SE (P < 0.01, Fig. 4).
Go to :
DISCUSSION
Human beings spend approximately one-third of their lives sleeping. Despite the importance of sleep health, it is often overlooked. Numbers of patients who suffer from sleep disorders involving reduced sleep time and/or quality are on the increase. The 2004 International Journal of Sleep reported that people who sleep less than 5 hours a night have a significantly higher death rate than those who sleep less than 7 hours a night, indicating that sleep health is important to overall health [25]. The current study examined the effects of sleep-inducing juice made of natural extracts on sleep quality and cardiac autonomic regulation in adults suffering from sleep difficulties.
The sleep-inducing juice employed in the current study was associated with enhanced resting parasympathetic activation and increased vagal tone at specific time points during sleep. Findings suggest that an 8-week course of sleep-inducing juice could improve sleep quality as assessed by self-reported and objective sleep measures. Sleep quality is important for maintaining innate biological rhythms and physiological homeostasis, and many individuals with sleep disorders or poor sleep quality present with other health problems, as well [26]. Persons with poor sleep quality are also more likely to experience cardiovascular events due to autonomic imbalance. The cardiac sympathetic hyperactivity and parasympathetic withdrawal often observed in those with primary insomnia are warning signs indicating an increased risk of morbidity and mortality from CVD [27].
Results from the present study also showed that the 8-week course of sleep-inducing juice was associated with enhanced resting vagal tone, including increased parasympathetic activity. Since participants were asked to maintain their normal lifestyle throughout the trial, it may be that improved nocturnal sleep was related to the changes in resting cardiac autonomic regulation observed in this study. While there are many potential mechanisms by which changes in nocturnal sleep quality could influence resting HRV indices, no physiological markers were measured in this study, and future research will be needed to uncover such mechanisms.
CFS patients with poor sleep quality [10] and individuals suffering from primary insomnia [27] may present with reduced nocturnal HRV due to autonomic imbalances defined as sympathetic hyperactivity and parasympathetic withdrawal. Studies on nocturnal HRV conducted by Tobaldini et al. [28] demonstrated that poor sleep quality induced by pathological sleep conditions, such as sleep breathing disorders, could cause significant cardiac autonomic imbalances during sleep. However, since a standardized protocol for measurement of nocturnal HRV has yet to be established, the effects of sleep quality on cardiac autonomic regulation during night sleep tend to be inconsistent among studies.
Burton et al. [10] conducted a nocturnal HRV analysis based on TST starting one hour after bedtime and found that rMSSD and HF in HRV, measurements of vagal activity, were decreased in patients with CFS. Conversely, Manconi et al. [29] investigated the influence of periodic leg movements during sleep on cardiac autonomic regulation and found no significant differences between patients with restless leg syndrome and healthy subjects for all nocturnal HRV indices. However, unlike Burton et al. [10], Manconi et al. [29] used only 5-min epochs of electrocardiograph signal during non-rapid eye movement sleep stage 2 when comparing differences in nocturnal HRV indices between groups. Another study by Manconi et al. [29] also found no significant results associated with sleep disorders in cardiac autonomic regulation during sleep using 5 min periods of RR intervals in accordance with the standardized protocol for short term HRV analysis. While the different clinical and pathological features of participants may also affect results, HRV analysis protocol can have a significant impact on cardiac autonomic regulation profiles during sleep. The novel findings observed in this study regarding changes in HRV indices suggesting enhanced nocturnal cardiac vagal tone after sleep-inducing juice may be due to the HRV analysis protocol used. The current study used short-term HRV recordings at 7 time points at 30 min intervals starting one hour after bedtime to explore temporal changes in cardiac autonomic regulation during sleep following sleep-inducing juice intake. Parasympathetic activity is key to the induction and maintenance of sleep [10], and HRV indices indicating increased parasympathetic activity during sleep suggest that sleep-inducing juice may contribute to improved sleep quality.
Many studies employ subjective measures, such as PSQI scores, to assess sleep quality or intervention effects under different clinical conditions [30]. Since poor sleep quality may also lead to increased daytime sleepiness and fatigue, the FSS is used to assess subjective fatigue due to disrupted nighttime sleep [31]. The results of the present study indicated that the 8-week intervention with sleep-inducing juice was associated with increased subjective sleep quality and decreased perceived fatigue levels. The PSQI has demonstrated high test–retest reliability and good validity in patients with primary insomnia [32] and has also been used to identify the effects of intervention therapy on sleep quality [33]. However, self-reported questionnaires introduce a certain amount of subjectivity due to differences in personal experiences and emotions. We thereby employed an objective data assessment technique to accompany self-reported estimations of sleep quality.
The pSG is the predominant method used to assess sleep-related disorders, but it is time-consuming and expensive, with difficulties related to procedures and interpretation. As such, many studies have employed an actigraphy monitor with accelerometer algorithms to objectively measure sleep quality [34]. Actigraphy is closely related to subjective sleep quality and perceived fatigue and has been reported as useful in identifying whether an intervention improved nighttime sleep [24]. Recently, the American Academy of Sleep Medicine Clinical Practice guidelines have suggested the use of actigraphy to assess certain sleep disorders such as insomnia, circadian rhythm sleep-wake disorder, sleep-disordered breathing, hypersomnolence, and insufficient sleep syndrome [35]. We thereby employed actigraphy to objectively detect potential effects of sleep-inducing juice on sleep quality.
The actigraphy results of the present study indicated that sleep-inducing juice might contribute to increased SE and decreased sleep onset latency. Another study used actigraphy to assess whether an intervention with natural extracts was associated with improved nighttime sleep. Howatson et al. [12] reported that TST and efficiency as measured by actigraphy were increased, including elevation of urinary melatonin after tart cherry juice intake. Tart cherry juice is known to have anti-oxidative stress and anti-inflammatory properties and high concentrations of melatonin [36]. Melatonin produced by the pineal gland is critical to endogenous circadian clock regulation of the sleep-wake cycle [34]. Thus, the increase of exogenous melatonin by tart cherry juice intake might have contributed to improvements in actigraphy sleep measures [12].
The sleep-inducing juice used in the present study was developed using natural fruit and vegetable extracts, but the major constituents and blend methods were proprietary and confidential per the manufacturer's instructions. This precludes the estimation of physiological mechanisms that could explain positive changes in sleep parameters obtained from actigraphy following sleep-inducing juice intake. The core material constituents of the sleep-inducing juice were theorized to increase the secretion of sleep-promoting hormones such as serotonin and melatonin, and enhance the biological availability of tryptophan [37].
Findings from this study suggest that TST is related to fruit and vegetable consumption in adults [37]. Other studies have shown that individuals with shorter sleep durations also reported lower fruit and vegetable consumption and lower levels of associated biomarkers such as lycopene, vitamin C, total carotenoids, α-carotene, and β-carotene [38]. The sleep-inducing juice evaluated in the present study was manufactured using fruits and vegetables as main ingredients, and increased synthesis of sleep-promoting hormones and changes in fruit and vegetable-associated biomarkers is to be expected from sleep-inducing juice consumption, and may be one of the mechanisms leading to the enhanced objective sleep quality assessed by actigraphy in this study.
There are several limitations of the current study. Since only young, healthy adults in a narrow age range participated in this study, results do not extend to differences associated with age or pathological conditions. Sleep characteristics such as TST and sleep-wake cycle vary based on age, and there are many different types of sleep disorders, rendering results from the present study difficult to generalize. We focused on examining the effectiveness of sleep-inducing juice itself by selecting individuals with mild-to-moderate sleep complaints (global PSQI score > 5) while excluding pathological conditions that might impact sleep quality. However, we did not control for differences in sleep hygiene, such as exercise, stress management, noise, sleep timing, avoidance of caffeine, nicotine, alcohol, and daytime napping [39].
Although water intake may affect the sleep quantity, results from recently published study reported that controlled mild dehydration does not affect sleep quality and quantity in young adults [40]. Thus, we do not think that the differences of water intake supplied to both groups have shown different patterns of sleep. Because, FS group only consumed 500 cc per day. In both group, there was no significant difference in body weight and body composition which affect sleep quality and quantity, as showed in Table 1, during intervention as well. Moreover, with monitoring the confounding factors, such as caffeine intake, alcohol consumption, and physical activity including exercise, the experimental condition in this study was conducted with a strictly controlled experiment by crossover design. Behavioral and environmental recommendations for normal nighttime sleep indicate sleep hygiene improvements, while critical for promoting sleep, can also be used to treat mild or moderate insomnia. We examined the effects of sleep-inducing juice only, instructing participants to continue their usual lifestyle habits over the entire experimental period.
In conclusion, the present study investigated the effects of sleep-inducing juice developed from natural extracts from fruits and vegetables on improvements in sleep quality and changes in nocturnal cardiac autonomic regulation associated with enhanced nighttime sleep in adults suffering from mild-to-moderate sleep problems. Results indicated that both subjective and objective measures of sleep quality were significantly improved by an 8-week course of sleep-inducing juice. The juice was also associated with increases in resting and nocturnal HRV indices of vagal activity, which may be associated with enhanced sleep quality.
Go to :
 XML Download
XML Download