

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Percutaneous mitral valve repair began with the first human MitraClip implant (Abbott Structural Heart, Santa Clara, CA, USA) in Venezuela in 2003.1)2) Since then, the Endovascular Valve Edge-to-Edge Repair Study (EVEREST) II study successfully showed the MitraClip therapy to be a viable therapeutic option for patients with severe mitral regurgitation (MR), in both severe functional mitral regurgitation (FMR) or degenerative mitral regurgitation (DMR), when compared against conventional surgery.3) With EVEREST II, surgical therapy provided greater efficacy although the MitraClip was associated with greater safety. Further studies have shown the MitraClip to be a treatment option for DMR patients with high surgical risk.4)5) In 2018, the Cardiovascular Outcomes Assessment of the MitraClip Percutaneous Therapy for Heart Failure Patients with Functional Mitral Regurgitation (COAPT) and Percutaneous Repair with the MitraClip Device for Severe Functional/Secondary Mitral Regurgitation (MITRA-FR) studies were published.6)7) While results were discordant, the COAPT study was generally accepted to show that the MitraClip therapy was superior to medical therapy alone for the treatment of severe symptomatic FMR. Since its first case, there have been more than 100,000 cases performed worldwide.
Besides the MitraClip, other novel technologies have been developed. These include repair devices such as the Carillon (Cardiac Dimensions, Kirkland, WA, USA), Mitralign (Edwards Lifesciences, Irvine, CA, USA), PASCAL(Edwards Lifesciences), Cardioband (Edwards Lifesciences), Millipede (Boston Scientific, Malborough, MA, USA) and MVRx (San Mateo, CA, USA). There has also been a plethora of percutaneous mitral valve replacement devices. None of these newer devices have had the success of the MitraClip and none have completed any major pivotal trial against surgery for DMR or optimal medical therapy for FMR. For the purpose of this paper, DMR is treated as synonymous with primary MR and FMR with secondary MR. In this review, the focus will be on the MitraClip therapy.
Go to : 
EVOLUTION OF THE MITRACLIP
The MitraClip device was initially developed by Evalve before the company was acquired by Abbott. With the success of the COAPT study, several iterations of the device have been developed. The device and procedure have been well described previously.8)9)
Figure 1 shows the evolution of the device. The MitraClip NT system was the first major update to the device in 2016 on the original classic MitraClip system. Enhancements were made to the steerable sleeve which allowed for greater precision in steering of the clip—there was reduced anterior movement with turning of the M knob. In addition, the gripper material was changed from Elgiloy to Nickel to enable an increase in gripper drop angle for more efficient and active leaflet capture.

Next was the MitraClip NTR/XTR system in 2018 which brought about the following improvements. Firstly, the clip delivery shaft is now a multi-lumen extrusion with reinforced braid and Pebax jacket. The stiffer shaft system reduces the degree of rotation during clip advancement into the left ventricle (LV). Secondly, a 1.5 cm increase in length of the clip delivery shaft allows for a higher transseptal puncture and yet still maintain sufficient reach on the mitral valve. The increased height gives more space for system maneuvring within the left atrium. Thirdly, the ability to open and close the clip arms without locking the device minimizes inadvertent undesirable medial and lateral movements. Lastly, the XTR system has 3 mm longer clip arms which allows for a greater reach and improved grasp to handle more complex anatomies.
Most recently in 2019, the MitraClip G4 was launched which added the option of wider clips. The additional 2 mm wider clip arms provide 50% greater grasping area and maximizes horizontal coaptation. Hence with the NTW and XTW, together with the earlier NTR and XTR, we now have 4 clip options of varying length and widths in our armamentarium to tackle a greater variety of leaflet pathologies. Another new feature of the G4 is Controlled Gripper Actuation which allows for independent gripper movement for leaflet grasping optimization. Lastly, an integrated pressure monitor in the MitraClip catheter allows for continuous left atrial pressure monitoring during implant.
Go to :
EVIDENCE FROM RANDOMIZED CONTROLLED TRIALS
Data supporting the use of the MitraClip can be broadly divided into those for DMR and FMR; and into randomized controlled trials versus registry studies.
The EVEREST II was the first study to compare percutaneous treatment of MR against surgery.3) It was a landmark study, influential not just for staking a claim that MR can be treated with the MitraClip but perhaps more importantly, demonstrating that FMR may also be treated effectively. The EVEREST II study was a randomized controlled trial of 279 patients in North America. It compared the MitraClip therapy against conventional surgery for DMR or FMR patients who met indications for surgical treatment of MR. Importantly, these were normal surgical risk patients—an important point to note. This is in comparison to studies like the initial PARTNER studies in which inoperable or high risk aortic stenosis patients were study subjects.
The results of EVEREST II should be interpreted in the context not just of the study population. Several other factors bear discussion as well. First, the MitraClip technology was in early human use. Second, the study teams all had limited experience performing the procedure. Third, 3D transesophageal echocardiogram was not available in most centres yet.10) During the study, most teams relied on the transgastric view for clip perpendicularity assessment. While technically achievable by most teams, it was nonetheless not easy and perpendicularity may have influenced technical success.
EVEREST II trial showed that surgery remained superior for the primary composite end point for efficacy which comprised of freedom from death, from surgery for mitral-valve dysfunction, and from grade 3+ or 4+ MR at 12 months. At 12 months, the rates of the primary end point for efficacy were 55% in the percutaneous-repair group and 73% in the surgery group (p=0.007). The respective rates of the components of the primary end point were as follows: death, 6% in each group; surgery for mitral-valve dysfunction, 20% vs. 2%; and grade 3+ or 4+ MR, 21% vs. 20%. The primary safety end point was a composite of major adverse events (MAEs) within 30 days. Not surprising, this was lower in the MitraClip arm with MAEs occurred in 15% of patients in the percutaneous-repair group and 48% of patients in the surgery group at 30 days (p<0.001). However, it was driven by complications many physicians and surgeons may consider less important: need for ≥2 units blood transfusions and prolonged ventilation (defined as mechanical ventilation >48 hours). The superior efficacy of surgery is also not surprising since surgery is a tried and tested therapy with operators having substantial experience. It would be unlikely for the MitraClip to achieve a similar technical result with the operators having limited experience, not just of the device, but of the entire procedure including its imaging components. Notwithstanding the superior outcomes of surgery, at 12 months, both groups had improved LV size, New York Heart Association (NYHA) functional class, and quality-of-life measures, as compared with baseline.
The EVEREST II study therefore established the following key benefits of the MitraClip, allowing the field to progress:
1. Lesser efficacy but superior safety when compared to surgery in DMR and FMR patients when randomized against surgery in normal risk patients.
2. Similar benefits in terms of functional improvement and quality-of-life.
3. MitraClip is a viable treatment option for FMR (not just DMR).
4. Despite MR reduction to only ≤2+, there was substantial clinical benefit with NYHA improvement.
While the EVEREST II study examined patients at normal risk for surgery, there were patients who failed the enrolment criteria due to higher surgical risk. These patients were at high surgical risk5) and of these, some were at prohibitive risk.4) These cohorts were analysed for outcomes. In the high risk cohort, patients were selected with the same anatomic criteria used for the randomized EVEREST II trial. Patients with grades 3+ to 4+ MR and a surgical mortality risk of ≥12%, based on the Society of Thoracic Surgeons risk calculator or the estimate of a surgeon co-investigator following pre-specified protocol criteria, were enrolled. The 351 patients completed 12 months of follow-up. MitraClip reduced MR to ≤2+ in 86% of patients at discharge. MAEs at 30 days included death in 4.8%, myocardial infarction in 1.1%, and stroke in 2.6%. At 12 months, MR was ≤2+ in 84% of patients. NYHA class improved from 82% with class III/IV at baseline to 83% with class I/II at 12 months (p<0.001). Therefore, the study showed that the MitraClip significantly reduced MR and improved clinical symptoms at 12 months in this high surgical risk cohort.
Of the high risk DMR patients, 127 were at prohibitive risk and had 1-year follow-up.4) In these patients, the MitraClip procedure was successfully performed in 95.3% and average hospital length of stay was 2.9±3.1 days. MAEs at 30 days included death in 6.3%, myocardial infarction in 0.8%, and stroke in 2.4%. The 1-year survival was 23.6%, with 82.9% of surviving patients having MR ≤2+ at 1 year, 86.9% in NYHA class I or II. SF-36 quality-of-life scores improved and hospitalizations for heart failure were reduced in patients whose MR was reduced. In summary, MitraClip in prohibitive surgical risk patients was associated with remarkable safety and good clinical outcomes, including decreases in re-hospitalization, and functional improvements at 1 year.
Arising from the EVEREST II randomized trial, high risk registry and prohibitive risk data, the Food and Drug Administration (FDA) approved the use of the MitraClip for patients with symptomatic DMR deemed high risk for mitral valve surgery on October 25, 2013.11) With that, it also entered the American Heart Association/American College of Cardiology guidelines in 2014 as a class IIb indication.12)13) The phrasing of the recommendation followed the data arising from the EVEREST II series of studies, recommending the MitraClip only in severely symptomatic patients with DMR at prohibitive surgical risk.
Only 27% of the EVEREST II study had FMR. Further the design of the EVEREST II study could not adequately address the question of whether the MitraClip was superior to optimal medical therapy. Surgery had not been convincingly shown to be beneficial as standard-of-care in FMR and optimal medical therapy was felt to be the gold standard. Hence additional studies were needed to convince the medical community and regulatory bodies that the MitraClip provided clinical benefits superior to optimal medical therapy alone.
The MITRA-FR6) and COAPT14) studies were therefore natural next steps in studying the appropriate use of the MitraClip. Both studies released the findings in 2018 and had, on the surface, discordant results. However, careful examination of both studies has highlighted key learnings.
Go to :
MITRA-FR
The French MITRA-FR study, presented at European Society of Cardiology (ESC) Congress in August 2018 and simultaneously published in the New England Journal of Medicine (NEJM) was the earlier study to be released.6) This was an investigator-initiated European study that examined FMR patients with moderate-severe MR that in the opinion of the heart team had been optimally medically treated.6)15) Although the study was funded by the French government and Abbott Vascular, the latter had no role in the design of the trial. The key criteria for study inclusion were severe secondary MR (defined as an effective regurgitant orifice area [EROA] of >20 mm2 or a regurgitant volume of >30 mL per beat), and a left ventricular ejection fraction (LVEF) between 15% and 40%. The study randomized 307 patients with symptomatic LV dysfunction and significant secondary MR to either medical therapy or medical therapy combined with the MitraClip procedure. The 92% of patients achieved an MR grade ≤2+ immediately after the procedure while there was no difference in the primary outcome of all-cause death and unplanned re-hospitalization for heart failure at 1 year which occurred in 54.6% of the intervention group and 51.3% of the control group. The mortality rate was 24.3% in the intervention group vs. 22.4% in the control group. The study utilized the ESC criteria for severe MR with EROA of 0.2 cm2.16)17) There were important limitations in the study. First, it did not have an independent committee for patient selection. Patients could be enrolled as long as the local heart team was convinced that the patient was on optimal medical therapy. MITRA-FR also did not mandate follow-up echocardiograms or 6-minute walk-tests for study subjects, and not surprisingly, a significant amount of follow-up data on echocardiographic outcome and functional status at 12 months were missing. Interestingly, the study allowed investigators to participate as long as they had performed 5 prior MitraClip procedures. Concerning the MITRA-FR study, one additional comment is necessary: despite the shortcomings of the study, the clinical event rates were similar with optimal medical therapy. This suggests that, as a strategy, the use of the MitraClip did not confer any significant additional risks, beyond the cost of the procedure.
Go to :
COAPT
The COAPT study was an industry-sponsored North American study that recruited 604 patients and randomized in a 1:1 ratio to either MitraClip and guideline-directed medical therapy (GDMT) or GDMT only.7)18) The results were announced at the Transcatheter Cardiovascular Therapeutics meeting 2 months after ESC and also simultaneously published in NEJM. COAPT enrolled patients with symptomatic heart failure and ≥3+ FMR, despite the use of maximal doses of GDMT. Patients had to have LVEF ≥20% and ≤50%, and a left ventricular end systolic dimension ≤70 mm. The primary effectiveness end point was all hospitalizations for heart failure within 24 months of follow-up.
In the COAPT study, the procedural success rate was 95%, defined as patients who had a successful clip implantation with MR ≤2+.7) The procedural complication rate was 8.5% and the primary safety endpoint of freedom from device-related complications at 12 months was 96.6%. At 1 year, the proportion of patients who continued to have ≤2+ MR was 95%.7) The annualized rate of all hospitalizations for heart failure within 24 months was 35.8% per patient-year in the device group as compared with 67.9% per patient-year in the control group (hazard ratio [HR], 0.53; 95% confidence interval [CI], 0.40–0.70; p<0.001). All-cause mortality within 24 months occurred in 29.1% of the patients in the device group as compared with 46.1% in the control group (HR, 0.62; 95% CI, 0.46–0.82; p<0.001). The number needed to treat over a 2-year period was 3.1 for the primary end-point of hospitalization for heart failure; and 5.9 for all-cause mortality. All prespecified secondary endpoints including quality of life and functional assessments were significantly improved in the MitraClip arm.
These stunning results showed that the MitraClip offered clinically superior results, including all-cause mortality, when compared to GDMT. Some key features in COAPT that contributed to these results included a central subject eligibility committee that adjudicated patient selection suitability—a key consideration being whether patients were indeed on maximally tolerated optimal medical therapy. The study also used a tiered set of criteria adapted from the 2003 American Society of Echocardiography (ASE) guidelines to quantify MR severity.18) Further, the study mandated follow-up echocardiograms and 6-minute walk tests. The results of the COAPT study were surprising, especially in the light of the just released MITRA-FR study. As a direct result of the study, on March 14, 2019, the FDA approved the use of the MitraClip for the treatment of patients with severe FMR who remain symptomatic despite GDMT.
Table 1 shows the key differences between the MITRA-FR and COAPT studies. While there are many learnings from a careful analysis of the MITRA-FR and COAPT studies, perhaps the most important insight is the conceptual framework of proportionate and disproportionate MR in the setting of impaired LV systolic function.19)20) Described by Grayburn, Sannino and Packer, the concept of proportionate and disproportionate MR provides at least a big part of the explanation on the difference between the 2 studies.19) In brief, the question is whether the MR is proportionately severe in relation to the degree of LV dysfunction and dilatation—such that excessive (i.e., disproportionate) MR beyond what was proportionate contributes to the adverse outcomes. As Grayburn et al.20) discussed, the principal reason to fully characterize and quantify the determinants of functional MR is to determine if an intervention directed at the mitral valve is capable of changing the clinical course of the disease. And thus, MR severity assessment is an integral part of this and here, there is already one key difference between MITRA-FR and COAPT. The MITRA-FR study used the 2014 ESC guidelines in which an EROA of 0.2 cm2 would qualify as severe. On the other hand, the COAPT study used a tiered set of criteria adapted from the 2003 ASE guidelines to quantify MR severity. The assessment of MR severity was also not limited to just the EROA. Instead, an integrative approach was adopted in COAPT. For example, tier one required EROA of ≥0.3 cm2 or presence of pulmonary systolic vein flow reversal.21)22)23) For the COAPT study, the majority of cases either met EROA criteria of ≥0.3 cm2 or had the presence of pulmonary vein systolic flow reversal. In essence, the COAPT study selected patients who had more severe MR than those selected for the MITRA-FR study. Second, the COAPT study excluded patients with severely dilated LVs. Compared to the MITRA-FR study, where the mean LV end diastolic volume was 135±35 mL/m2 while that of the COAPT study was 101±34 mL/m2. Overall, patients in COAPT had more MR and less sick and dilated hearts (i.e., disproportionate MR), while those in MITRA-FR has sicker hearts and less MR (proportionate MR). By extension, it made sense to treat the MR in patients where the MR was disproportionately more severe; while in those where the MR was not so severe, the LV dysfunction was the primary problem and fixing the MR did not make substantial difference (and no additional harm) in the eventual outcome.
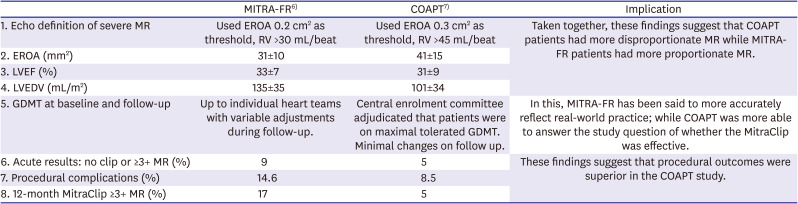
Table 1
Key differences between MITRA-FR and COAPT studies
| MITRA-FR6) | COAPT7) | Implication | |
|---|---|---|---|
| 1. Echo definition of severe MR | Used EROA 0.2 cm2 as threshold, RV >30 mL/beat | Used EROA 0.3 cm2 as threshold, RV >45 mL/beat | Taken together, these findings suggest that COAPT patients had more disproportionate MR while MITRA-FR patients had more proportionate MR. |
| 2. EROA (mm2) | 31±10 | 41±15 | |
| 3. LVEF (%) | 33±7 | 31±9 | |
| 4. LVEDV (mL/m2) | 135±35 | 101±34 | |
| 5. GDMT at baseline and follow-up | Up to individual heart teams with variable adjustments during follow-up. | Central enrolment committee adjudicated that patients were on maximal tolerated GDMT. Minimal changes on follow up. | In this, MITRA-FR has been said to more accurately reflect real-world practice; while COAPT was more able to answer the study question of whether the MitraClip was effective. |
| 6. Acute results: no clip or ≥3+ MR (%) | 9 | 5 | These findings suggest that procedural outcomes were superior in the COAPT study. |
| 7. Procedural complications (%) | 14.6 | 8.5 | |
| 8. 12-month MitraClip ≥3+ MR (%) | 17 | 5 |
Values are presented as mean±standard deviation.
COAPT = Cardiovascular Outcomes Assessment of the MitraClip Percutaneous Therapy for Heart Failure Patients with Functional Mitral Regurgitation; EROA = effective regurgitant orifice area; GDMT = guideline-directed medical therapy; LVEDV = left ventricular end-diastolic volume; LVEF = Left ventricular ejection fraction; MITRA-FR = Percutaneous Repair with the MitraClip Device for Severe Functional/Secondary Mitral Regurgitation; MR = mitral regurgitation; RV = regurgitant volume.
![]()
An inevitable question that arises from these studies is how to decide which case has proportionate or disproportionate MR. Some clinicians have tried to use the mean figures in both studies as reference data points to decide on what constitutes proportionate or disproportionate MR. Like others, we strongly discourage the use of these values in this manner. The mean values imply that there is a range of value for which the MR may be considered proportionate or disproportionate. Instead, it is far more important to consider the conceptual framework instead and adopt it to the care of the individual patient.
Go to :
REGISTRIES
Since the approval for commercial use of the MitraClip, a multitude of registries (Table 2) with large patient populations has given us insight to its real-world experience. The European registries provided us the early experience with the therapy after the EVEREST II trial. They are the ACCESS-EU24) which included 567 patients from 14 European sites, Transcatheter Valve Treatment Sentinel Pilot Registry (TCVT)25) with 628 patients from 25 centres in 8 European countries and transcatheter mitral valve interventions (TRAMI)26) with 749 patients from Germany. The patients treated were elderly and were a high risk cohort (Logistic EuroSCORE: ACCESS-EU 23.0, TCVT 20.4 and TRAMI 20.0).24)25)26) Nonetheless, there were excellent results with acute procedural success in excess of 90%, as compared to 77% in EVEREST II. This highlights the learning curve and improved results with increased experience in using the device. The procedure has also proven to be safe with low periprocedural adverse events. In addition, more than 70% of the patients treated had FMR. Though mortality was high at 1-year (approximately 15–20%), this was not surprising considering the patients treated were older, sicker and predominantly FMR with depressed LV function and increased co-morbidities. The COAPT and MITRA-FR studies on MitraClip for FMR reflected similar mortality rates.6)7)
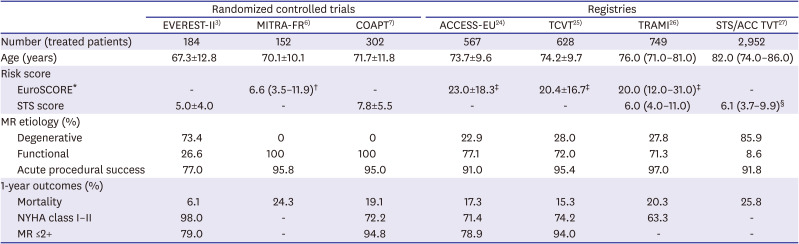
Table 2
Overview of key trials and registries
| Randomized controlled trials | Registries | |||||||
|---|---|---|---|---|---|---|---|---|
| EVEREST-II3) | MITRA-FR6) | COAPT7) | ACCESS-EU24) | TCVT25) | TRAMI26) | STS/ACC TVT27) | ||
| Number (treated patients) | 184 | 152 | 302 | 567 | 628 | 749 | 2,952 | |
| Age (years) | 67.3±12.8 | 70.1±10.1 | 71.7±11.8 | 73.7±9.6 | 74.2±9.7 | 76.0 (71.0–81.0) | 82.0 (74.0–86.0) | |
| Risk score | ||||||||
| EuroSCORE* | - | 6.6 (3.5–11.9)† | - | 23.0±18.3‡ | 20.4±16.7‡ | 20.0 (12.0–31.0)‡ | - | |
| STS score | 5.0±4.0 | - | 7.8±5.5 | - | - | 6.0 (4.0–11.0) | 6.1 (3.7–9.9)§ | |
| MR etiology (%) | ||||||||
| Degenerative | 73.4 | 0 | 0 | 22.9 | 28.0 | 27.8 | 85.9 | |
| Functional | 26.6 | 100 | 100 | 77.1 | 72.0 | 71.3 | 8.6 | |
| Acute procedural success | 77.0 | 95.8 | 95.0 | 91.0 | 95.4 | 97.0 | 91.8 | |
| 1-year outcomes (%) | ||||||||
| Mortality | 6.1 | 24.3 | 19.1 | 17.3 | 15.3 | 20.3 | 25.8 | |
| NYHA class I–II | 98.0 | - | 72.2 | 71.4 | 74.2 | 63.3 | - | |
| MR ≤2+ | 79.0 | - | 94.8 | 78.9 | 94.0 | - | - | |
*Shown as mean standard±deviation or median (interquartile range) as according to primary paper; †EuroSCORE II; ‡Logistic EuroSCORE; §STS score 6.1% (3.7–9.9%) and 9.2% (6.0–14.1%) for mitral valve repair and replacement, respectively.
ACC TVT = American College of Cardiology Transcatheter Valve Therapy; COAPT = Cardiovascular Outcomes Assessment of the MitraClip Percutaneous Therapy for Heart Failure Patients with Functional Mitral Regurgitation; EVEREST = Endovascular Valve Edge-to-Edge Repair Study; MITRA-FR = Percutaneous Repair with the MitraClip Device for Severe Functional/Secondary Mitral Regurgitation; MR = mitral regurgitation; NYHA = New York Heart Association; STS = Society of Thoracic Surgeons; TCVT = Transcatheter Valve Treatment Sentinel Pilot Registry; TRAMI = transcatheter mitral valve interventions.
![]()
The United States (US) subsequently published its data from the national Society of Thoracic Surgery/American College of Cardiology Transcatheter Valve Therapy (STS/ACC TVT) Registry with 2,952 patients treated at 145 hospitals.27) Once again, the patients treated were elderly (median age, 82 years) and high risk (STS predicted risk of mortality 6.1% and 9.2%) for mitral valve repair and replacement respectively, but acute procedural success rates remained high at 91.8%. As the FDA only approved the use of MitraClip for DMR in US then, in contrast to the European registries, 85.9% of patients treated in the registry had DMR.
Go to :
APPROVED USE AND EXPERIENCE IN ASIA
The MitraClip is approved for use in Europe, US, Australia/New Zealand, parts of Asia including Brunei, Hong Kong, Indonesia, Japan, South Korea, Malaysia, Philippines, Singapore, Taiwan, Thailand, and other parts of the world.
In the Asia-Pacific, use of the MitraClip started in 2011 in Australia and Singapore. The early experience as shown in the MitraClip Asia-Pacific Registry (MARS) show that initial clinical outcomes were similar to US and European real world experience.28) The procedural volume remained low till 2019, in large part due to the cost of the device. In April 2018, MitraClip was approved for use in Japan, with reimbursement provided. By July 2020. the procedural volume in Japan have reached more than 2,000 cases. The Japanese experience suggest that the uptake of the therapy is closely associated with appropriate reimbursement policies. In countries like Australia, Malaysia and Singapore, where reimbursement for the therapy remains less well established, uptake has been more patchy and slower.
MARS is a regional multi-centre registry started in February 2011 in an effort to describe the MitraClip experience in the Asia-Pacific region. Thus far, 17 centres from 10 countries (Australia, Singapore, Taiwan, Hong Kong, New Zealand, Indonesia, Vietnam, Thailand, China and Malaysia) are included. In the first publication, Yeo et al.28) described outcomes in a series of 145 patients treated between February 2011 to October 2013. Of note, the logistic EuroSCORE and STS scores were 16.8±14.6% and 7.4±8.1%, respectively. Interestingly, the proportion of DMR patients was more than what was seen in the European experience where the device had been in longer commercial use. In MARS, the self-reported acute procedural success at 93.7% was higher than in EVEREST II (77.0%) and comparable with all other registries (91% in ACCESS-EU, 95.4% in TCVT-EU, 97% in TRAMI and 92% in STS/ACC TVT).3)24)25)26)27) The 30-day mortality in MARS (5.6%) was similar with ACCESS-EU (3.4%), TRAMI (4.5%) and STS/ACC TVT (5.2%) but higher than EVEREST II (1.0%), reflecting the differences in risk profiles. There was significant improvement in NYHA functional class (82.1% in class I or II at 30-day compared to 31.7% at baseline, p<0.001) as well as MR reduction to ≤2+ (76.8% at 30-day compared to 0% at baseline, p<0.01). When compared to the ACCESS-EU data, the degree of MR reduction ≤2+ at 30 days was lower (91.2% for ACCESS-EU vs. 76.8% for MARS). There are 2 important reasons that may explain this. First, the ACCESS-EU study represent a large cohort of patient across Europe over a longer period of time, suggesting a likely greater experience with the therapy. Second, the MARS data was early in the experience of all participating sites with the 145 patients divided across multiple countries and hospitals, such that each hospital had very limited experience.
Relative to Europe, there was a greater proportion of DMR patients than FMR patients treated with the MitraClip. An inevitable question is whether results in FMR and DMR were similar. MARS data showed that, for FMR and DMR, the acute procedural success (95.5% vs. 92%, respectively, p=0.515), 30-day mortality (4.5% vs. 6.7%, respectively, p=0.555) and functional improvement to NYHA class 1 and 2 at 30 days (78.2% vs. 83.0%, respectively, p=0.525), were similar in both groups.29) The 30-day MAEs rate suggested that DMR patients may have more complications although this was not statistically significant between the 2 groups (FMR 9.2% vs. DMR 14.7%, p=0.281).
In Japan, the AVJ-514 trial was a prospective multi-centre observational trial, demonstrating the use of MitraClip for the purpose of regulatory approval.30) 30 patients were enrolled with the mean age of 80.4±7.0 years, STS score of 10.3±6.59%. The 53.3% of the patients had DMR while the rest were FMR. Acute procedural success was achieved in 86.7% and there was no MAE. At 30-days, there were no deaths, 86.7% had MR ≤2+ and 96.7% were NYHA functional class I or II. With this study, the MitraClip obtained regulatory approval with the first case in Japan in April 2018. In Taiwan, Lee et al.31) reported their early experience of MitraClip in Taiwan in 20 patients. The authors reported in the single centre study excellent acute procedural success (95%), safety (no peri-procedural MAE) and low 30-day mortality (5%) in a high risk group of patients (EuroSCORE II 13.2±17.7% and STS score 8.7±9.0%). There was also significant improvement in MR as well as NYHA functional class at 1 month compared to baseline.
Go to :
OFF-LABEL USE OF THE MitraClip
With increased experience on the use of the MitraClip therapy, more complex and unique subsets of patients have been treated, off-label, with encouraging results. Symptomatic hypertrophic obstructive cardiomyopathy (HOCM) has traditionally been addressed by medical therapy and invasive septal reduction therapy in suitable patients. Systolic anterior motion of the mitral valve contributes not just to LV outflow tract obstruction but also frequently MR. Recently, percutaneous mitral valve plication with the MitraClip device to address systolic anterior motion of the mitral valve has shown to reduce LV outflow tract gradients, improve MR grade and bring about symptom relief.32)33)34) In patients with concomitant primary mitral valve disease and HOCM, MitraClip can be a feasible therapy especially in those who are at high or prohibitive surgical risk.32)
Dynamic worsening of FMR from either volume overload or increase in afterload has been associated with poor outcomes35)36) and reduced exercise capacity.37)38) Thus far, there is a paucity of data on effective therapies to address dynamic MR and most treatment options have been drawn from experiences with handling FMR. Reports of MitraClip to treat dynamic MR have shown promising results in symptom relief but more studies on this under-recognized clinical entity is required.39)40)
Various transcatheter techniques to address tricuspid regurgitation (TR) are rapidly emerging. Percutaneous edge-to-edge repair, with its success in the mitral space, have naturally steered its way to the tricuspid valve and currently is the leading therapy to treat TR. Both the TRILUMINATE trial and TriValve registry have demonstrated the efficacy of this technique in reducing TR severity and symptom improvement.41)42)
Go to :
PASCAL
The PASCAL system is the next percutaneous edge-to-edge repair system to join the transcatheter mitral valve repair armamentarium. It received CE Mark approval for treatment of patient with MR in February 2019 and for patients with TR in May 2020. Similar to the MitraClip system, it uses a transseptal approach and share similar anatomical considerations in the suitability and complexity of edge-to-edge repair. However, the PASCAL system has certain innovative features that may provide some technical advantages. Firstly, it has a central spacer to fill the regurgitant orifice area. In addition, the spacer reduces the need to pull the mitral valve leaflets together for approximation, hence reducing stress on the leaflets especially if there is a wide coaptation gap. Secondly, the broad and contoured paddles distribute the forces applied on the leaflets over a larger area. Thirdly, the PASCAL system developed the independent clasping function which allowed for optimization of leaflet capture. Lastly, device elongation slenderizes the system and make maneuvering in the subvalvular space safer. The CLASP study was the first study evaluating the PASCAL system.43) It was a prospective single-arm study which demonstrated excellent MR reduction (MR grade ≤2+ and ≤1+ were 98% and 86%, respectively) and significant functional improvement at 30-days. Randomized controlled trials pitting PASCAL with the MitraClip system are currently underway in the CLASP IID (DMR) and CLASP IIF (FMR) studies.
Go to :
CONCLUSION
Percutaneous mitral valve repair has come a long way since the first human case in 2003. The edge-to-edge MitraClip repair remains the gold standard for percutaneous technologies. Newer technologies will have to demonstrate at least non-inferiority to this established front-runner. It is also the only mitral valve interventional or surgical therapy to show superior efficacy and safety against GDMT for isolated FMR. Continued enhancements in the MitraClip technology, as well as in imaging, are expected to reduce procedural complexity and improve technical outcomes. The REPAIR MR aims to study the use of the technology in moderate risk cohorts of DMR patients.44) Additional studies are also required to better understand the timing of the MitraClip in FMR patients including its priority and position relative to different drugs and biventricular pacing.
Go to :
 XML Download
XML Download