

 PDF
PDF Citation
Citation Print
Print



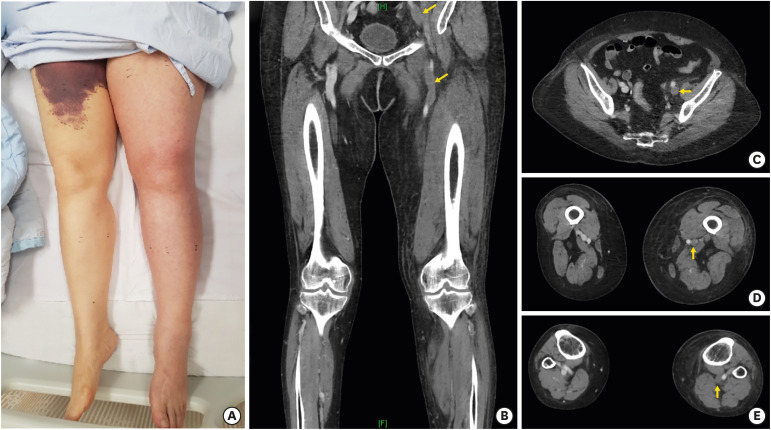
A 76-year-old woman was admitted for electrophysiologic study. The patient was obese with a body mass index of 32.9 kg/m2, but did not have any risk factors of deep vein thrombosis. Both femoral veins were catheterized. During the study, atrioventricular (AV) nodal reentrant tachycardia was induced, and AV nodal slow pathway was ablated. Hemostasis was achieved through use of manual compression at puncture sites and absolute bed rest. One day after the procedure some ecchymosis was observed at the right inguinal area, however the left inguinal area was clear and the patient was subsequently discharged. One week later the patient reported discomfort in the left inguinal area during sleep, and progressive swelling of the left lower extremity. Upon examination, the patient's left lower extremity was swollen, red, and cooler than the right extremity (Figure 1A). Computed tomography (CT) of the patient's left lower extremity revealed extensive thrombosis in the left iliac and femoral veins in coronal sections (Figure 1B) and extensive swelling and deep vein thrombosis in horizontal views (Figure 1C-E). There was no extrinsic venous compression on CT images, thus, May-Thurner syndrome was ruled out. The patient was placed on Apixaban 10 mg twice a day (b.i.d.) for 10 days, then reduced 5 mg b.i.d. orally for 3 months. Swelling in the left lower extremity was reduced after the patient began Apixaban and was normalized after 2 weeks of treatment. This case displayed an unusual delayed complication of electrophysiologic study and serves as an instructive case for electrophysiologists to be aware of possible delayed complications.
The informed consent that allows the publication of clinical data was obtained from the patient.
 XML Download
XML Download