

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Although anemia is a well-known risk factor for poor outcome in patients with cardiovascular diseases,1)2) the association between polycythemia and incident atrial fibrillation (AF) has not been well studied. A population study showed elevated hematocrit level is associated with an increased risk of adverse cardiovascular events3)4) and adverse cardiovascular events include ischemic stroke, and ischemic stroke is highly related to AF. Recent studies investigated the relationship between anemia5) or red cell distribution width6) and AF, however, there had not been studied about the association between the elevated hematocrit and incident AF yet. Recently, we also investigated the clinical impact of elevated hemoglobin levels on cardiovascular events after coronary intervention.7) The potential mechanisms of polycythemia on cardiovascular outcomes are suggested, such as, the pathophysiologic roles of stored iron burden and its hemorheological risks as hemodynamic force. Polycythemia increases blood viscosity and can contribute to increasing hemodynamic shear stress8): a physical force generated by blood flow that can contribute to pressure overload and cardiovascular remodeling.9)10)11) An experimental study also revealed that cardiac inflammatory change under the condition of myocardial ischemia can contribute AF development via cardiac remodeling.12) Therefore, elevated hemoglobin level can affect clinical cardiovascular event, especially AF development, those had not been well studied yet.
Taken together, there were evidences that hemodynamic forces may affect cardiovascular remodeling.11)13) Despite this, the clinical impact of polycythemia and its contribution to AF developments have not been well investigated.8)14) In the present study, we conducted a large, comprehensive investigation using a Korean cohort covering the general population. The primary objective is to identify the association between increased hemoglobin and incident AF. The secondary objective is to identify the specific hemoglobin concentration more associated with an increased risk for these adverse events. Subgroup analyses were performed according to cardiovascular comorbidities to investigate whether high hemoglobin level affects the risk of incident AF.
METHODS
This nationwide and retrospective cohort study investigated the relationships between increased hemoglobin and incident AF. It was performed according to the recommendations of the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement reporting guidelines (Supplementary Table 1).15) The study protocol adhered to the ethical guidelines of the 2013 Declaration of Helsinki and was approved by the Institutional Review Board of Yonsei University College of Medicine (IRB No.3-2019-0322). The need for informed consent was waived as the study involved retrospective analysis of an anonymized cohort.
Data source
The present study used the Korean National Health Insurance Service (NHIS)-based National Sample Cohort (NSC) database (more than 1 million subjects).16) Because all Korean medical facilities were necessarily linked by Korean NHIS, NHIS database includes the information of the entire Korean population (more than 50 million subjects). And this sample cohort was extracted using probability sampling from all beneficiaries of the National Health Insurance and National Medical Aid in 2002 depending on the entire national cohort information. Systematic sampling was performed (sampling rate of 2.2% of the whole eligible Korean population in 2002 and they were followed until 2015) with respect to each of the 1,476 strata, based on age, sex, eligibility status, socioeconomic status, and income level, with the sample size proportionate to the cohort size of the strata. A previous study confirmed that the sample was representative by comparing it with the entire Korean population.16)
The cohort database consisted of the three following datasets: i) sociodemographic information of the beneficiaries; ii) medical claims, including information on diagnoses based on the 10th revision of the International Classification of Disease (ICD-10) codes, as well as on records of outpatient visits (including visits to individual physician's office), admission, and treatment; iii) National Health Examination data of the cohort members. The National Health Examination dataset was created for the entire Korean population from 2002 to 2015 by the National Health Insurance Corporation. During this time, the National Health Examination was conducted biennially and involved chest X-rays, physical examinations, detailed questionnaires regarding medical history and lifestyle behaviors (smoking and alcohol intake), and regular blood tests including serum creatinine (mL/min) measurements. The death registration database of the Korea National Statistical Office, which includes the date and cause of death, was linked with the NHIS cohort database. Every subject in the sample cohort was linked using Korean social security numbers, all of which were deleted after the cohort was constructed and replaced by subject serial numbers to prevent leakage of personal information.
Study cohort
Among the entire South Korean population (about 47 million people in 2002), 96.6% were registered in the NHIS. About 70% of the entire cohort underwent a National Health Examination. Adults over 18 years of age (n=506,805) who had undergone a National Health Examination at least once between 2009 and 2015 were included in the NHIS-NSC (n=1,041,441) (NHIS-2016-2-189).16) Each of them was then followed from the day of their health examination until 31 December 2015. To acquire the enrolled subjects' medical history, screening was carried out from January 2002 to December 2008 (disease-free baseline period). The subjects' past medical histories were assessed based on the ICD-10 codes (Supplementary Table 2) to identify diseases such as heart failure, hypertension, diabetes mellitus, stroke, myocardial infarction (MI), peripheral vascular disease, or AF diagnosed before the health examination. Each diagnosis was defined as the first occurrence on at least 2 different days of outpatient hospital visits or on the first hospital admission (Supplementary Table 2).16)17) The following exclusion criteria were applied (Figure 1): i) those diagnosed with AF (n=4,926, diagnoses based on the ICD-10 codes: ICD-I48) before undergoing a health examination; ii) those with valvular AF, such as mitral valve stenosis or prosthetic valve disease (n=304, ICD-I050, I052, I342); and iii) missing data (n=67,306) such as laboratory data or questionnaires about smoking status and alcohol intake administered at the health examinations. Because it had been known that the mechanisms or the causes of AF development between valvular and nonvalvular AF were different, we excluded valvular AF as the consensus of other previous studies. A final population of 434,269 subjects was included in the analysis (Figure 1). In the sensitivity analysis, we additionally excluded those with chronic kidney disease (CKD) (with an estimated glomerular filtration rate [eGFR; estimated by serum creatinine using CKD-EPI formula18)] lower than 60 mL/min; n=21,115), chronic obstructive pulmonary disease (J41–44; n=22,811), cirrhotic liver disease (K74; n=7,123), or any malignant disease (C00–C97; n=25,813) because these diseases are related to anemia; therefore, they are major confounding factors when analyzing the relationship between hemoglobin level and incident AF. After applying these criteria, a population of 366,442 subjects without chronic diseases related to anemia were included in the sensitivity analysis to investigate the robustness of our main analysis. The cohort was followed until the time of death; to a condition disqualifying receipt of the NHIS services, such as emigration; or to the end of the study (December 31, 2015).

Figure 1
Study cohort and included subjects from the NHIS-NSC (overall general population).
NHIS-NSC = National Health Insurance Service-National Sample Cohort.
*A total of 67,306 were excluded owing to invalid data in health examination items including baseline characteristics blood test results, and smoking and alcohol history.
![]()
Lifestyle factors and other clinical variables, and the primary outcome
The subjects' past medical histories were analyzed using medical claims data with ICD codes (Supplementary Table 2), questionnaires regarding disease history, and measurements of blood pressure and fasting blood glucose levels collected during the health examinations. Subjects were classified as obese (body mass index [BMI] ≥27.5 kg/m2), overweight (23.0–27.4 kg/m2), normal BMI (18.5–22.9 kg/m2), or underweight (<18.5 kg/m2).19) Smoking status was classified as non-smoking, <20 pack-years or ≥20 pack-years (former- or current-) smokers. Alcohol intake was classified as either 0–220.5 g/week or ≥220.5 g/week. Socioeconomic status variable was obtained based on participants' income level, and it was divided into 11 categories (0–10) and was applied in main analysis.16)
The primary outcome was the relationship between increased hemoglobin level and incident AF. To acquire the subjects' stroke history, we investigated cerebral bleeding and infarction (ICD-10 code: I60–64), excluding transient ischemic attacks (G45) or other kinds of thromboembolisms. The accuracy of the stroke diagnosis in the NHIS database has been previously validated.16)
Statistical analyses
To understand cohort characteristics according to hemoglobin level, we divided the subjects according to hemoglobin categories (moderate-to-severe anemia: hemoglobin <11.0 g/dL for both sexes; mild anemia: ≥11.0 and <13.0 g/dL for men and ≥11.0 and <12.0 g/dL for women; normal: ≥13.0 and <16.5 g/dL for men and ≥12.0 and <16.0 g/dL for women; and polycythemia groups: hemoglobin ≥16.5 g/dL for men and hemoglobin ≥16.0 g/dL for women) based on World Health Organization statement.20) Accordingly, all analyses were separately done for both sexes.
Cox proportional-hazards model regression analyses were used to analyze the association between incident AF and polycythemia or anemia, with adjustments for confounding variables. Models adjusting for clinical variables (including age, sex, BMI, socioeconomic status, hypertension, dyslipidemia, diabetes mellitus history, eGFR, and lifestyle factors such as smoking status and alcohol intake) were used to assess these associations. The included subjects were followed from their National Health Examination until death, disqualification (emigration), or end of the study in the Cox-regression analysis.
To minimize the effects of potential confounders and investigate the robustness of our study results, a sensitivity analysis was performed by analyzing subjects without chronic diseases related to anemia (see METHODS – Study cohort) to investigate the pure effect of hemoglobin on incident AF in this population. Linear estimates of hazard ratios (HRs) about relationship between hemoglobin levels and incident AF were tested with adjustment for clinical variables. Furthermore, we estimated the predictive accuracy of hemoglobin in case of incident AF among subjects with normal hemoglobin levels and those with polycythemia by calculating the c-index on the basis of the receiver operating characteristic (ROC) curve from logistic regression models. To investigate the specific hemoglobin concentration that increased the occurrence of AF, we analyzed the sensitivities and specificities of different hemoglobin levels and determined the point with the highest Youden's index (sensitivity + specificity − 1).21)22)
A 2-sided p value of <0.05 was considered statistically significant. All statistical analyses were performed using R software (version 3.5.2; R Project for Statistical Computing) and SAS software (version 9.2, SAS Institute, Cary, NC, USA).
RESULTS
Baseline characteristics
Because the hemoglobin categories were different in both sexes based on World Health Organization statement, all analyses were done separately for both sexes. The baseline characteristics of men and women according to baseline hemoglobin categories are summarized in Table 1. The entire cohort included 217,497 men (851,375 person-years of follow-up) and 216,772 women (821,634 person-years of follow-up) who had undergone National Health Examinations between 2009 and 2015. The mean hemoglobin levels in the moderate-to-severe anemia, mild anemia, normal hemoglobin, and the polycythemia groups were 9.7, 12.3, 14.9, and 17.0 g/dL in men and 9.9, 11.5, 13.2, and 16.5 g/dL in women, respectively. Among men, subjects with polycythemia (10.0%) were younger, and there were more subjects with obesity and heavy alcoholics (≥220.5 g/week) in the polycythemia group than in the other groups, while there were fewer subjects with hypertension, diabetes, dyslipidemia, chronic lung disease, malignant diseases, and who are taking anti-platelet agents, beta-blockers, and statins (each p<0.01) (Table 1). Among women, a small number of subjects with polycythemia (0.2%) were older, and more subjects had obesity, hypertension, diabetes, dyslipidemia, chronic lung disease, and malignant diseases, and more subjects were heavy smokers (≥20 pack-years) and heavy alcoholics (≥220.5 g/week) than in the other groups (p<0.01 in all cases) (Table 1).
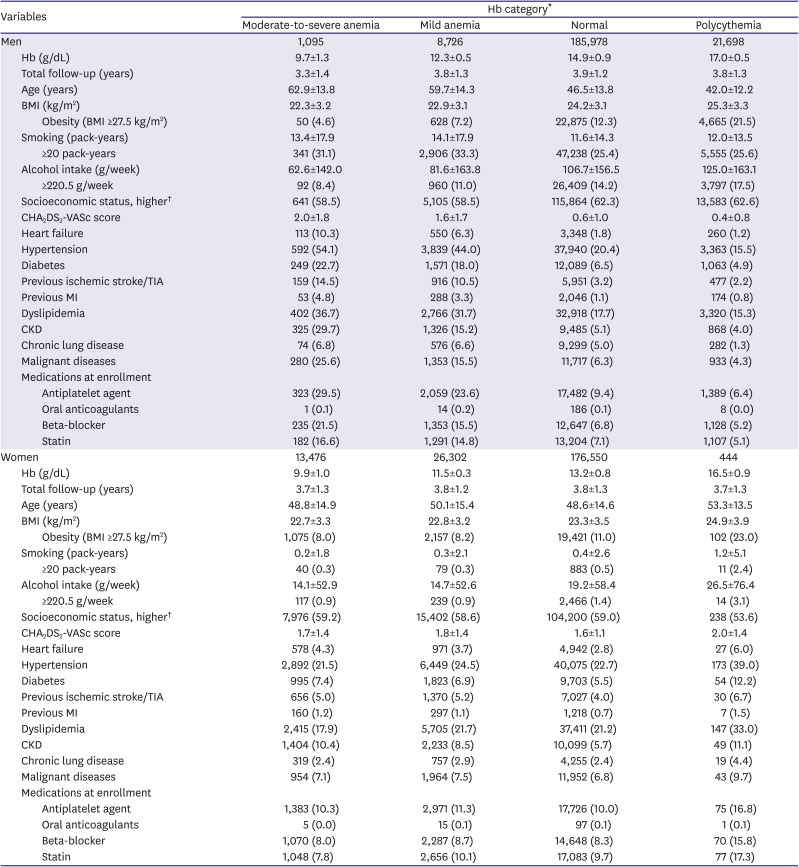
Table 1
Baseline characteristics of men (n=217,497) and women (n=216,772) according to Hb levels
Values are expressed as mean±standard deviation or number (%).
BMI = body mass index; CKD = chronic kidney disease; Hb = hemoglobin; MI = myocardial infarction; TIA = transient ischemic attack.
*Baseline Hb levels of included subjects were categorized as followings based on World Health Organization statement (moderate-to-severe anemia: Hb <11.0 g/dL for both sexes; mild anemia: ≥11.0 and <13.0 g/dL for men and ≥11.0 and <12.0 g/dL for women; normal: ≥13.0 and <16.5 g/dL for men and ≥12.0 and <16.0 g/dL for women; and polycythemia: Hb ≥16.5 g/dL for men and Hb ≥16.0 g/dL for women).20) †In our cohort, socioeconomic status was divided into 11 categories (0–10) and was applied in main analysis. In this table, socioeconomic status was divided into 2 groups: higher (6–10 categories of income level) and lower (0–5 categories of income level).
![]()
Sex-based approach for the associations between increased hemoglobin and incident atrial fibrillation
In men, the Cox proportional-hazards models using the covariates of age, BMI, socioeconomic status, smoking and alcohol intake habits, baseline creatinine, and histories of hypertension, diabetes, and dyslipidemia showed that polycythemia was independently associated with increased risks of incident AF (HR with 95% confidence interval [CI], 1.50 [1.28–1.76], p<0.001) when compared with normal hemoglobin levels (Table 2). Incident AF events in Table 2 are represented as “per 100,000 person-years” to provide more accurate comparisons among groups because the follow-up time periods differed among groups. In women, it showed that polycythemia was independently associated with increased risks of incident AF (1.69 [1.13–2.56], p<0.001) when compared with normal hemoglobin levels (Table 2). We performed a sensitivity analysis to examine the robustness of our main results in a smaller population after the exclusion of patients with chronic diseases affecting hemoglobin levels (see METHODS – Study cohort; n=366,442); the overall results were consistent (Supplementary Table 3).
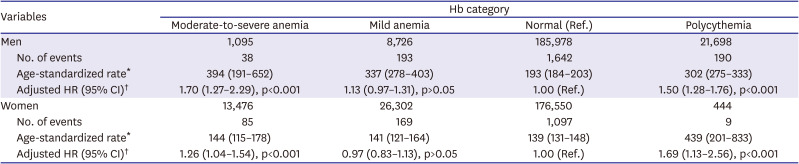
Table 2
Event rates and corresponding adjusted HRs for incident AF in relation to Hb levels in men and women
AF = atrial fibrillation; CI = confidence interval; Hb = hemoglobin; HR = hazard ratio.
*Age-standardized rate: events per 100,000 person-years (age standardization was stratified by 5-year interval). †Age and clinical variables (including body mass index, socioeconomic status, smoking and alcohol history, baseline creatinine, and history of hypertension, diabetes, and dyslipidemia)–adjusted HR.
![]()
Figure 2 showed the relationships between hemoglobin level and incident AF tested using the log-linear model with a thin-plate spline among the overall study population of 434,269 subjects. This test indicated U-shaped associations between hemoglobin level and incident AF. The sensitivity analysis among 366,442 subjects also showed consistent results (Supplementary Figure 1).
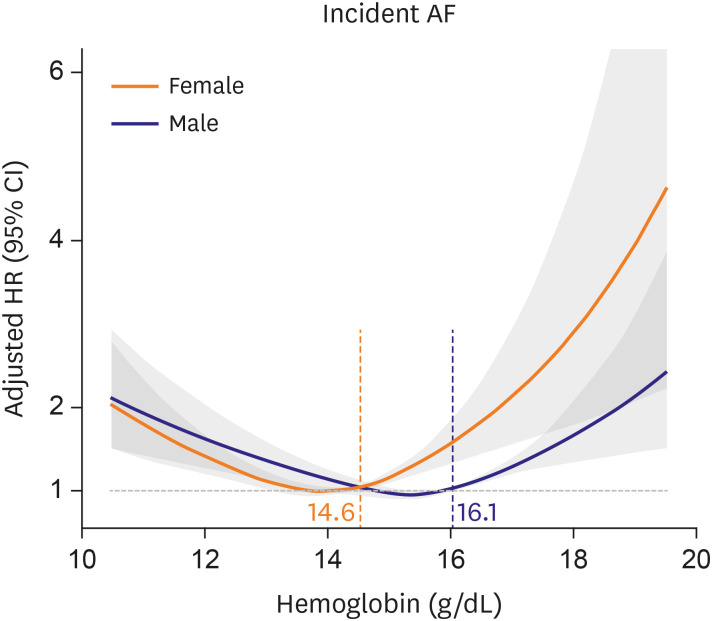
Figure 2
Concentration-responsive U-shaped relationships between Hb level and incident AF tested by log-linear model with a thin-plate spline (age, body mass index, serum creatinine, history of hypertension, diabetes, and dyslipidemia, socioeconomic status, and smoking and alcohol intake habits-adjusted HRs). It also showed the specific Hb level (lower 95% CI more than 1.0 of HR) associated with increased risk of incident AF in both sexes.
AF = atrial fibrillation; CI = confidence interval; Hb = hemoglobin; HR = hazard ratio.
![]()
The age-standardized incidence rate of each relevant outcome was also higher in the polycythemia group than in the normal hemoglobin group, for both men and women (Table 2).
In both men and women, moderate-to-severe anemia was associated with increased incidences of AF (1.70 [1.27–2.29] and 1.26 [1.04–1.54], respectively; p<0.001 in all cases) (Table 2).
Sex-based approach for the associations between hemoglobin and incident atrial fibrillation among normal hemoglobin and polycythemia group
We fit the covariate-adjusted Cox proportional-hazards log-linear models with the thin-plate spline curves for hemoglobin, and the increment in hemoglobin concentration was significantly associated with an increased risk of incident AF among subjects with normal hemoglobin levels and those with polycythemia. The relationships between hemoglobin level and incident AF were almost linear above 14.6 g/dL in women and above 16.1 g/dL in men (Figure 2; and Supplementary Figure 1 for the sensitivity analysis). When setting reference value as cutoff level of polycythemia, the results also showed consistently in both sexes (Supplementary Figure 2). As it had been known increased hematocrit had thromboembolic risks, we also analyzed the relationship between increased hemoglobin and incident ischemic stroke, and it showed consistent U-shaped relationship (Supplementary Figure 3).
Figure 3A shows the ROC curves for the association between hemoglobin concentration and incident AF among women and men. The c-indices of hemoglobin levels concerning these associations in the prediction models were 0.82 (0.81–0.83) and 0.83 (0.81–0.84) for women and men, respectively. The specific level of hemoglobin associated with an increased risk of incident AF was analyzed as above 14.5 g/dL in women and above 16.0 g/dL in men based on the highest Youden's index (Figure 3 and Supplementary Table 4; Supplementary Figure 4 and Supplementary Table 5 for the sensitivity analysis). Figures 3B (women) and 3C (men) are Kaplan-Meier cumulative incidence curves according to hemoglobin cutoff (≥14.5 g/dL in women and ≥16.0 g/dL in men) among these subjects (all log-rank p<0.05).

Figure 3
(A) ROC curves of specific Hb level for predicting incident AF among normal Hb and polycythemia subjects (among female subjects with Hb ≥13.9 g/dL and male subjects with Hb ≥15.2 g/dL who had linearly increasing relationships between Hb and incident AF as they were shown in Figure 2). The c-indices on the basis of the AUC for Hb in predicting incident AF were 0.82 and 0.83 in women and men, respectively. Hb levels above 14.5 g/dL in women and above 16.0 g/dL in men showed the highest Youden's index (sensitivity + specificity - 1). (B and C) Kaplan-Meier curves (B, women; C, men) about the time-dependent incident AF cases according to Hb cutoff (≥14.5 g/dL in women and ≥16.0 g/dL in men) among these subjects (all long-rank p<0.05).
AF = atrial fibrillation; AUC = area of receiver operating characteristic curve; Hb = hemoglobin; ROC = receiver operating characteristics curve.
![]()
Subgroup analysis
Several subgroups among subjects with polycythemia showed association trends about an increased risk of incident AF in men and women when compared with the normal hemoglobin group: older age subgroup (≥65 years), subjects with heavy smokers (≥20 pack-years), subjects with lower socioeconomic status, and subjects with diabetes, however, interaction p-values compared with the opposite subgroups were all >0.05 in these subgroups (Table 3). Meanwhile, hypertensive male subgroup among subjects with polycythemia showed higher association trends with an increased risk of incident AF when compared with the normal hemoglobin group (1.72 [1.48–2.04] vs. 1.27 [1.07–1.46], p-value for interaction was 0.019 compared to the subgroup without history of hypertension) (Table 3).
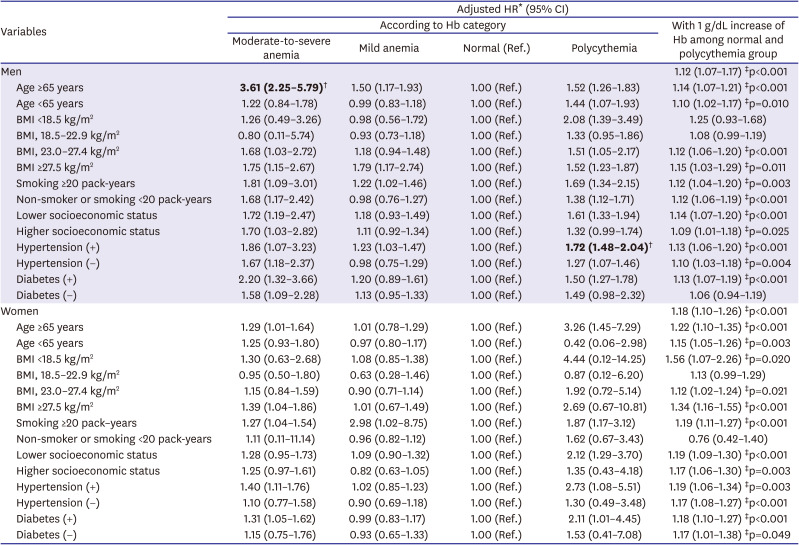
Table 3
Subgroup analysis of incident AF and corresponding adjusted HRs in relation to Hb levels in men and women
Bold-faced p values are <0.05 compared to normal Hb group.
AF = atrial fibrillation; BMI = body mass index; CI = confidence interval; Hb = hemoglobin; HR = hazard ratio.
*Age and clinical variables (including BMI, socioeconomic status, smoking and alcohol history, baseline creatinine, and history of hypertension, diabetes, and dyslipidemia)–adjusted HR. †Interaction p value <0.05 (compared with the opposite subgroup of each). ‡p<0.05.
![]()
In the normal hemoglobin and polycythemia groups, a 1 g/dL increase in hemoglobin levels was associated with a further increase in the risks of incident AF (1.12 [1.07–1.17] with p<0.001 in men; and 1.18 [1.10–1.26] with p<0.001 in women), and most subgroups also showed consistent results in both men and women (Table 3).
In patients with moderate-to-severe anemia, most subgroups among male subjects, and elderly, obese, heavy smokers, hypertensive, or diabetes female subjects showed association trends about an increased risk of incident AF when compared with the normal hemoglobin group, however, most interactions with the opposite subgroups were not significant except elderly (aged ≥65 years) male subjects (interaction p<0.001, Table 3).
DISCUSSION
This nationwide study used a large cohort covering the Korean general population. It found that both the polycythemia and anemia groups were associated with increased risks of incident AF when compared with the normal hemoglobin group, and that hemoglobin levels showed a U-shaped relationship with these conditions. Specifically, above normal hemoglobin levels, with 1 g/dL increase in hemoglobin concentration were associated with a further increase in the risk of incident AF (by 12.0% in men and by 18.0% in women), even after adjusting for clinical variables. We also observed that a hemoglobin level above 14.5 g/dL in women and above 16.0 g/dL in men had association trend with an increased risk of incident AF.
Although anemia is a well-known risk factor for adverse cardiovascular outcomes,1) the association between polycythemia and incident AF had not been well studied. Recent observational study revealed the relationship between anemia and AF, however, this study did not investigated the association between polycythemia and AF, nor hemoglobin cutoff related to an increased risk of AF.5) Another studies have investigated the association between high hemoglobin levels and an increased risk of ischemic cardiovascular outcomes or mortalities.23) However, moderate elevations in hematocrit and blood viscosity can also be beneficial, because shear stress also induces nitric oxide release.24) Our group recently investigated the relationship between anemia and AF recurrence after catheter ablation.25) However, these studies did not investigate the relationship between elevated hemoglobin and incident AF,5)23)25) or did not investigate either the cutoff value of hemoglobin associated with an increased risk of incident AF related to high hemoglobin levels.5)
Interestingly, our data showed that subjects with increased hemoglobin had an increased risk of incident AF among men even relatively higher cardiovascular comorbidities compared to normal hemoglobin group. The hemorheological risk with hemodynamic force of the stored iron burden might be one of the potential mechanisms of increased hemoglobin on incident AF. Previous studies showed that increased hematocrit was associated with increased blood viscosity and elevated shear stress, it can be possible that increased hemoglobin may also be associated with tissue hypoxia or atrial dilation and subsequent AF development.8)26)27) In the present study, these associations were observed in several subgroups of men and women, and there were higher association trends for incident AF among elderly subjects and subjects with hypertension, diabetes, obesity, heavy smokers (≥20 pack-years), and lower socioeconomic status in men and similar association trends in women also (Table 3). And hypertensive male patients showed more significant association between polycythemia and incident AF compared to patients without hypertension (interaction p-value 0.019, Table 3), it might suggest that careful observations about cardiovascular events are needed especially in these population.
Several studies have addressed the association between increased hematocrit and elevated endothelial shear stress,8)10) or red cell distribution width and AF,6)28) but not much is known about the effect of elevated hemoglobin on the incident AF in general Asian populations. Recent cohort studies suggested that adverse arrhythmic or neurological outcomes are increased, showing a U-shaped relationship between hemoglobin levels and AF,5) and dementia.29) A pilot study also suggested that high hematocrit might worsen the degree of disability after ischemic stroke.30) Our group previously studied the associations between elevated hemoglobin levels and unfavorable outcome after coronary interventions in patients with coronary heart diseases.7) However, specific hemoglobin level associated with increased risk of incident AF or major ischemic cardiovascular outcomes had not been studied well among the general population. In the present study, high levels of hemoglobin were associated with increased risks of incident AF in both sexes; especially levels above 14.5 g/dL in women and above 16.0 g/dL in men. It might suggest that careful observations about cardiovascular events are needed especially in these population. Further prospective studies are needed to investigate these associations among these populations.
Despite its strengths, our study had some limitations. We included subjects from the NHIS-NSC database who had undergone National Health Examinations, thus, there may have been selection bias. However, our database was compiled using a stratified sampling method based on age, sex, eligibility status, socioeconomic status, and income level, and the sample's representativeness was examined previously.16) Furthermore, our analysis adjusted for additional available clinical parameters, including BMI, socioeconomic status, and smoking and alcohol intake habits.
Generally, there were more subjects with anemia in pre-menopausal younger women compared to younger men, therefore, the age discordance between men and women might be resulted from this respect. This study was based on the Administrative claim data, we could not obtain the echocardiographic parameters that affect AF development. Although we analyzed the effect of hemoglobin on incident AF, with adjustment for clinical parameters, there were some confounders regarding the etiologies of anemia and polycythemia. We could not evaluate the effect of serum stored iron, hematocrit, and blood viscosity because those parameters are absent in NHIS-NSC database. However, it is well known that hemoglobin level has relatively linear association with hematocrit or blood viscosity. Moreover, the cause of bleeding events and information about transfusion were not considered in the present study. Despite this, our overall results were consistent after subjects with potential confounders were excluded from the analysis of hemoglobin and adverse events (those with chronic diseases such as CKD, chronic obstructive pulmonary disease, cirrhotic liver disease, or any malignant diseases). Although the study results of female subjects were consistently shown with those of male subjects after adjusting readily available cardiovascular comorbidities, the number of female subjects with polycythemia was small and they had relatively higher cardiovascular comorbidities, therefore, careful interpretation is needed. The conditions of anemia and polycythemia can be influenced by taking certain drugs, such as anticoagulants and oral contraceptives. However, our study excluded patients with histories of prevalent AF (Figure 1), and there were few patients who taking oral anticoagulants (Table 1). Although oral contraceptives can affect hemoglobin levels in women, however, we did not investigate these drugs, this is the limitation of this study. However, the sensitivity analysis with excluding such chronic diseases which can more affect hemoglobin levels than oral contraceptives showed consistently with our main analysis. Because we did not investigate the mechanisms of such hemorheological effects of polycythemia on incident AF, it was hard to investigate the reason of the gender difference of the increased hemoglobin effects on incident AF. It might also be related to the hemorheological effects or hemodynamic forces of the stored iron burden. Previous studies have addressed whether blood viscosity and the shear stress of increased hematocrit are related to endothelial dysfunction,8)10) but we did not investigate whether increased hematocrit is associated with endothelial inflammation or plaque formation; thus, the mechanism of the relationship between increased hemoglobin and incident AF remains unclear. Also, we did not investigate the long-term effect of the red cell distribution width, or the effort for lowering blood viscosity such as voluntary blood donation, further prospective study is needed about this regard.
In conclusion, even in the Korean general population, not only anemia, but also increased hemoglobin were significantly associated with higher rates of incident AF. Especially, subjects with hemoglobin levels ≥14.5 g/dL in women and ≥16.0 g/dL among men were associated with increased risks of incident AF. Further prospective studies are needed to investigate these associations among patients with increased hemoglobin.
 XML Download
XML Download