

 PDF
PDF Citation
Citation Print
Print



A 76-year-old woman with a history of coronary artery bypass graft surgery underwent percutaneous coronary intervention of a calcified left circumflex artery (LCx) lesion with proximal tortuosity and enlargement (Figure 1A-C). On a RotaWire Floppy, a 1.5-mm burr was managed to cross the lesion with a rotational speed of 220,000 rpm (Figure 1D, Supplementary Video 1). During a final polishing run, the burr collided with the lesion, and the driveshaft prolapsed into the distal left main coronary artery (LM). The driveshaft was suddenly fractured (Figure 1E, Supplementary Video 2), resulting in Ellis type III perforation (Figure 1F, Supplementary Video 3). After the implantation of two polytetrafluoroethylene-covered stents, left coronary angiography revealed no contrast extravasation (Figure 1G). Conversely, angiography of bypass graft elucidated persistent contrast extravasation from the distal LM, requiring surgical repair by filling and sealing the perforation site with surgical cotton (Figure 1H, Supplementary Video 4).
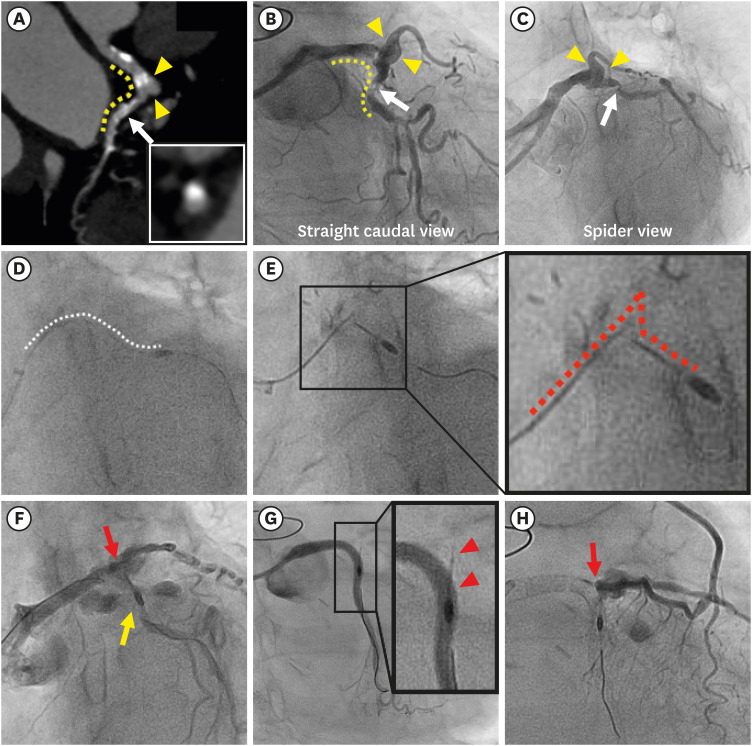 | Figure 1Computed tomographic, fluoroscopic and angiographic images. (A-C) Baseline computed tomography and coronary angiography revealing severe tortuosity (yellow dotted line) and enlargement (yellow arrowheads) proximal to the culprit lesion (white arrow). The inset in A demonstrated a protruding calcified nodule. (D) The white dotted line indicates the normal course of the driveshaft during initial rotablation. (E) Prolapse and fracture of the driveshaft (red dotted line) at the extremely tortuous and enlarged segment. The inset presents an enlarged image. (F) Ellis type III coronary perforation of the distal left main with vascular ectasia (red allow) and left circumflex artery (yellow allow). (G) Left coronary angiography showing no contrast extravasation. The inset presents an enlarged image of the fractured and remnant driveshaft (red arrowheads). (H) Persistent contrast extravasation confirmed by angiography of left internal mammary artery to left anterior descending artery graft (red arrow).
|
Three possible mechanisms of rotablator driveshaft fracture and massive coronary perforation were analyzed: 1) After the burr collided with the lesion, the driveshaft was easily prolapsed due to significant proximal tortuosity and enlargement. 2) Significant mechanical forces exerted at the acute bend of the ostial LCx led to driveshaft fracture. 3) The fractured driveshaft lacerated the arterial wall of the distal LM.
This case highlights the potential precautions of rotational atherectomy in cases with significant proximal tortuosity and enlargement. To prevent this catastrophic complication, delivering rotablator burrs through deep insertion of the guide catheter or child guide catheter beyond the top of the angulation is mandatory (Figure 2).1)2)
 | Figure 2Computed tomographic, angiographic, and intravascular ultrasound images of rotational atherectomy using a 5Fr child guide catheter (“mother-and-child” technique). (A) Baseline CT showing heavily calcified chronic total occlusion lesion in the distal right coronary artery (white arrow). The inset shows a cross-sectional CT image of the culprit lesion with dense calcification. (B, C) Baseline coronary angiography (B: LAO cranial view, C: RAO view) revealing severe tortuosity (yellow dotted line) proximal to the culprit lesion (white arrow). (D) Deep insertion of 5Fr child guide catheter (Heartrail ST01, Terumo, Tokyo, Japan) (yellow arrow) beyond the tortuous segment, by the anchor balloon technique. (Inset in D) After predilatation with 2.25-mm semicompliant balloon resulted in underexpansion, intravascular ultrasound images of the distal RCA lesion (white arrow) revealed severe concentric calcification. (E) Deep insertion of the child guide catheter (yellow arrow) beyond the tortuous segment enabled smooth delivery of a 1.25-mm burr (red arrow) and rotational atherectomy. (F) Final angiography after stenting and postdilatation. White line indicates the implanted stent.CT = computed tomography; LAO = left anterior oblique; RAO = right anterior oblique.
|

 XML Download
XML Download