

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Approximately half of patients with signs and symptoms of heart failure (HF) have preserved ejection fraction.1)2)3)4)5)6) As the population ages and the comorbidity increases, the prevalence of HF with preserved ejection fraction (HFpEF) increases considerably.1)3)4)5)6) The results of the early epidemiologic study revealed that patients with HFpEF were older, more female, and had a higher rate of comorbidity, such as hypertension, diabetes mellitus (DM), obesity, chronic kidney disease, and atrial fibrillation (AF).1) What these patients have in common is that ejection fraction is preserved, but there are symptoms and signs of clinical HF. Therefore, it has been considered a kind of syndrome in the absence of a confirmative diagnostic or therapeutic indicator. The basic question is whether we have to continue to fill this difficult “jigsaw puzzle” named HFpEF, or whether we have to make a new base after breaking all of the HF classification methods based on ejection traction. In this review, we will review some pretty meaningful pieces that are already set in the puzzle, and we believe that these will not be changed even if the base of the puzzle changes.
Go to : 
HEART FAILURE WITH PRESERVED EJECTION FRACTION VS. DIASTOLIC HEART FAILURE
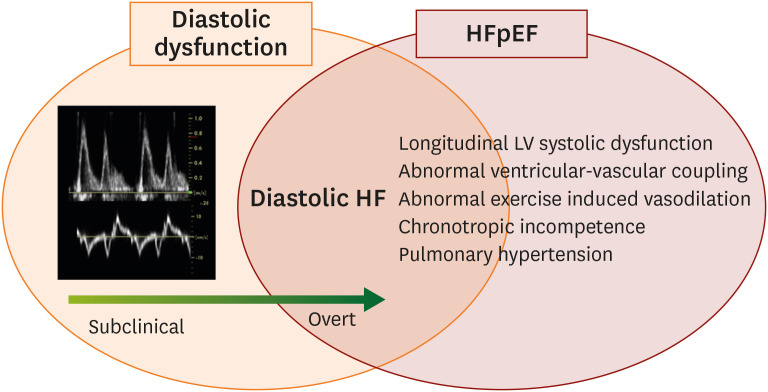
HFpEF was initially termed diastolic HF.7) HFpEF and diastolic HF have been used interchangeably and confusedly for the last 20 years. In principle, HFpEF and diastolic HF are not the same diagnostic terms, and the former should be understood to a larger range of diagnosis since several alternative and complementary mechanisms exist either presence or absence of left ventricular (LV) diastolic dysfunction (Figure 1).8)9) There has been a recent expansion of the ejection fraction derived classification of patients with HF. Accordingly, HF with midrange ejection fraction and HF with improved ejection fraction appeared recently.10)11) Therefore, the term “diastolic HF” tends not to be used although diastolic HF is also an important term in terms of mechanism. Each of these two terms has its pros and cons. For example, if a patient presented with HF but a meaningful diastolic dysfunction or elevation of LV filling pressure are not proven in diagnostic tests, the patients can be diagnosed with HFpEF, but not enough to be diagnosed with diastolic HF. In the case of HFpEF which the diastolic dysfunction is not proven, there is a fundamental limitation in developing a therapeutic agent because of lack of any indicators to monitor. In order to overcome these shortcomings of HFpEF, there is a trend to classify several key phenotypes in this heterogeneous disease, and construct a treatment strategy according to the main pathophysiology.
Go to :
PATHOPHYSIOLOGY AND PHENOTYPES OF HEART FAILURE WITH PRESERVED EJECTION FRACTION
There have been a number of efforts to defining phenotypes of patients with HFpEF according to their main features and pathophysiology after a few clinical trials, but repetitively failed to prove benefits of potential pharmacologic treatments in this heterogeneous syndrome.12)13)14)15) Different treatment strategies according to the phenotype have been presented very convincingly, however, it is often difficult to specify this as only one phenotype.12)13)14)15)
Representative phenotypic classifications of HFpEF are presented in Figures 2 and 3, which might help physicians to understand the main clinical presentation and pathophysiology in managing patients with HFpEF.12)15) As shown in Figure 2, patients with HFpEF can be roughly classified into 3 phenotypes: exercise induced elevation of LV filling pressures, volume overload or right HF.12) The first phenotype of “exercise-induced elevation of LV filling pressures”, expressing the lowest risk type, but also the most difficult to diagnose as HFpEF.12) The predominant symptom in these patients is exertional dyspnea and there are no definite clues in echocardiographic features or brain natriuretic peptide (BNP) levels.12) The second phenotype of “volume overload” is the common one that physicians recognize.12) The third phenotype of “right HF” is the highest risk clinical subclass with poor prognosis.12) An another attractive phenotype classification of HFpEF that provides clinicians with a specific and effective therapeutic strategies to individual patients is demonstrated in Figure 3.15) There are 8 phenotypes, which include predominant metabolic syndrome (often referred to as “garden variety” associated with hypertension, obesity, DM, metabolic syndrome, and/or chronic kidney disease), coronary artery disease, predominant right HF, AF, hypertrophic cardiomyopathy like phenotype, valvular heart disease, high-output HF, rare causes such as restrictive cardiomyopathy or constrictive pericarditis.15) This phenotype classification based on etiology and pathophysiology is quite helpful in guiding initial treatment, but not mutually exclusive, and therefore sometimes difficult to place patients into a single category.15) However, even in patients classified as a garden variety phenotype after exclusion of certain diseases that require specific treatment, the mechanism of HFpEF varies with a more predominant contributing components among aortic stiffness (increased afterload), cardio-metabolic (systemic inflammation), and cardio-renal (increased preload) aspects. Recently, a few novel “phenomapping” techniques by machine learning to define clusters of patients based on dense phenotypic data have been suggested to provide an unbiased way to classify heterogeneous clinical syndromes of HFpEF.16)17)
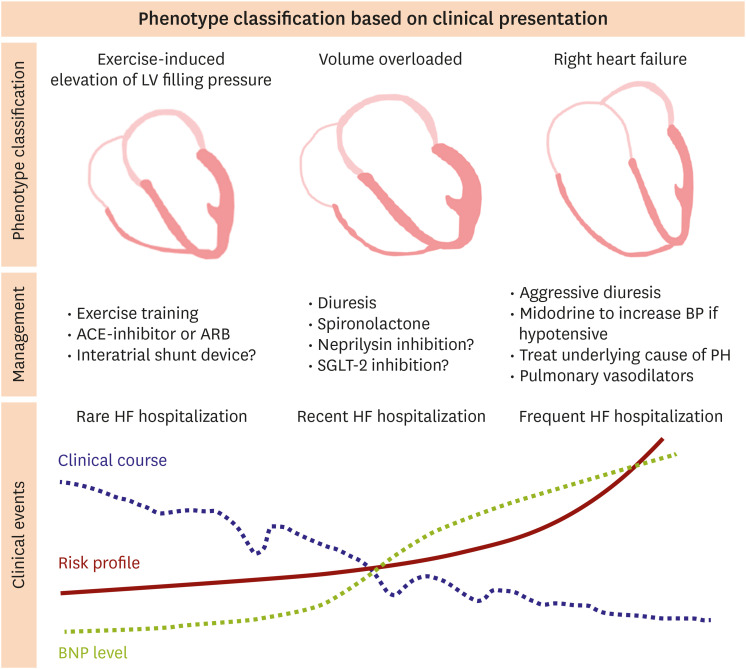 | Figure 2Phenotype classification of HF with preserved ejection fraction based on clinical presentations.ACE = angiotensin-converting enzyme; ARB = angiotensin II receptor blocker; BNP = brain natriuretic peptide; BP = blood pressure; HF = heart failure; LV = left ventricular; PH = pulmonary hypertension; SGLT-2 = sodium-glucose cotransporter-2.
|
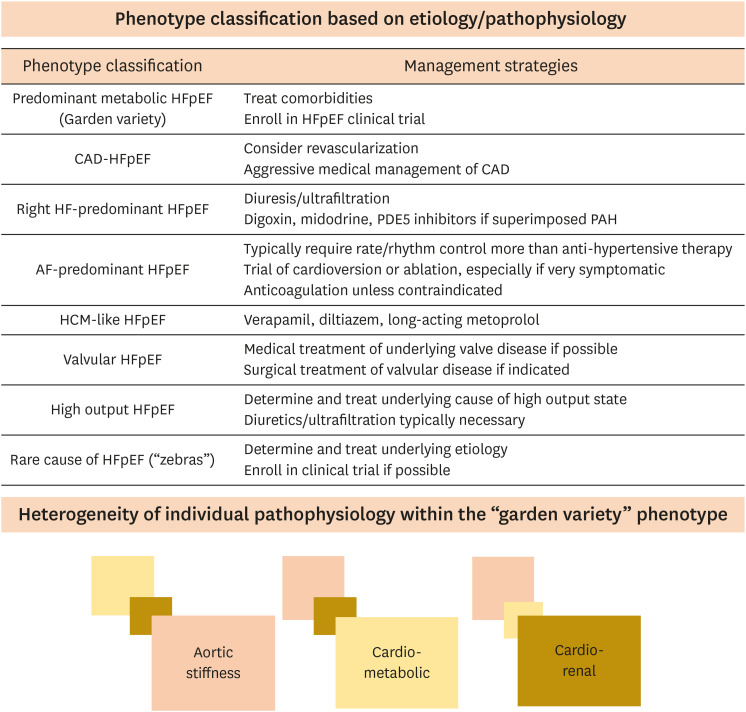 | Figure 3Phenotype classification of HFpEF based on etiology and pathophysiology.AF = atrial fibrillation; CAD = coronary artery disease; HCM = hypertrophic cardiomyopathy; HF = heart failure; HFpEF = heart failure with preserved ejection fraction; PAH = pulmonary arterial hypertension; PDE5 = phosphodiesterase type 5.
|
Go to :
DIAGNOSTIC CHALLENGES IN HEART FAILURE WITH PRESERVED EJECTION FRACTION
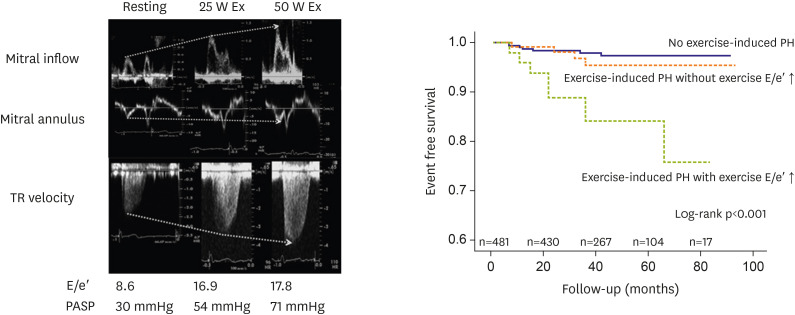
The diagnosis of HFpEF is still challenging, because symptoms are nonspecific and can be explained by several alternative non-cardiac conditions, such as chronic lung disease, anemia, and chronic kidney disease.8) In patients with phenotypes of volume overload or right HF based on clinical presentation,12) it is not difficult to document typical signs and symptoms of HF, such as pulmonary congestion, elevated BNP, and advanced diastolic dysfunction on Doppler echocardiography. However, in patients with the phenotype of exercise-induced elevation of LV filling pressure especially in those with significant LV structural abnormalities, we often encounter a few problems of echocardiogram only assessed at rest for HFpEF diagnosis.18)19)20) First, diastolic dysfunction as assessed by echocardiogram is highly prevalent in the elderly population.19)20) Second, echocardiographic variables indicating diastolic dysfunction may be absent in a significant proportion of patients diagnosed with HFpEF.19) The existing tools to assess LV systolic performance are far from perfect.19) Last, viewing HFpEF as results of ventricular stiffening and diastolic dysfunction only is an oversimplification although there are complementary and complex mechanisms.19) Additionally, exertional dyspnea is a common clinical problem. It can be complex and multiple etiologies such as respiratory causes, cardiac causes, metabolic causes and psychological causes.20) The differential diagnosis of HFpEF is challenging in stable elderly patients with equivocal symptoms. Therefore, we need to perform an exercise stress test because we cannot explain the patients' symptom completely with a resting echocardiography.20)21) A noninvasive diagnostic test for diastolic dysfunction using supine bicycle exercise Doppler echocardiography has been set up about 15 years ago.20) Because this echocardiographic method has advantages for evaluation of diastolic function during exercise. It is possible to get continuous imaging at each stages of exercise.20) Moreover, since the supine position increases myocardial wall tension and oxygen demand, it is suitable for diastolic stress.20) Currently, diastolic stress test is recommended for evaluation of exercise-induced elevation of LV filling pressure if the resting echocardiographic evaluation is inconclusive for diagnosis or exclusion of HFpEF.18)21) In a simultaneous invasive-echo study in patients with HFpEF and non-cardiac dyspnea, much improved diagnostic performance of adding exercise E/e′ on the European Society of Cardiology criteria were proven by demonstrating a 30% increase of sensitivity from 60% to 90%.18) In addition to the improvement of diagnostic performance and risk stratification of HFpEF,21)22)23)24)25) diastolic stress test can provide a prognostic information.26)27)28) Holland et al. showed the incremental prognostic implications of LV filling pressure with exercise in patients with or without inducible myocardial ischemia.26) Our previous work also demonstrated the prognostic values of exercise-induced elevation of LV filling pressure and consequent exercise-induced pulmonary hypertension in subjects with preserved LV ejection fraction (Figure 4).27) The types and methods of diastolic stress test vary from invasive to noninvasive techniques.21) Therefore, it is needed to apply an appropriate stress test after considering the patient's clinical situation and the established facility in each institution.
Go to :
COMMON COMORBIDITIES IN HEART FAILURE WITH PRESERVED EJECTION FRACTION: HYPERTENSION AND ARTERIAL STIFFNESS
Arterial stiffness is a cardinal feature of vascular aging and hypertension.29) The aorta deliveries blood from the LV to the capillaries, acting as a highly efficient conduit and cushion. As the aorta stiffens, blood travels faster, returns earlier, and boosts pressure in late systole. As a result, arterial stiffness results in elevation of augmentation pressure and augmentation index, and widening of the arterial pulse pressure.30)31)
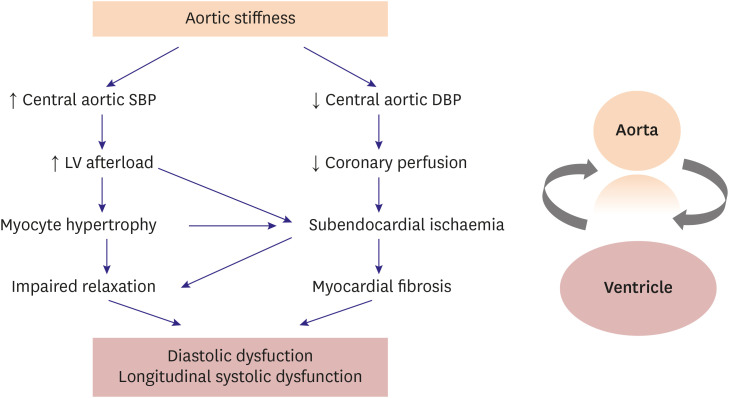
Figure 5 shows the possible relationship between arterial stiffness and LV diastolic/longitudinal systolic dysfunction which was originally proposed by Mottram et al.32) Increased central systolic blood pressure (BP) results in increasing LV afterload and makes myocyte hypertrophy and impaired relaxation. Simultaneously, central aortic diastolic BP decreases.32) It reduces coronary perfusion and induces subendocardial ischemia and fibrosis.32) These adverse effects finally lead to LV diastolic dysfunction and longitudinal systolic dysfunction. Recent studies have demonstrated that noninvasively assessed central BP and variables reflecting arterial mechanical function at rest and with exercise are well correlated with LV diastolic function and LV systolic functional impairments such as LV global longitudinal strain and apical rotation.33)34)35)36)37)38) In terms of sex difference in HFpEF, the indices reflecting central arterial stiffness in radial arterial tonometry were higher in women than in men.38) Additionally, we found that the relationship between variables of arterial stiffness and LV diastolic function was stronger in women.38) In another study, the dynamic changes of arterial elastance during exercise in patients with hypertension were investigated.39) When age-matched men and women with hypertension were compared, there was a steeper rise of arterial elastance index during exercise in hypertensive women.39) Moreover, the arterial elastance index during exercise was an independent determinant of exercise duration.39) To summarize, arterial stiffness and ventricular-vascular interaction at rest and dynamic changes during stress are considered a principal pathophysiology in patients with HFpEF and should be a therapeutic target for preventing HFpEF.40)41)42)43)
Go to :
DIABETES MELLITUS
DM is a common comorbidity in HF and has an adverse impact on prognosis.44)45) Classically, many studies have been conducted on the mechanisms and treatment strategies of diabetic cardiomyopathy, in which myocardial dysfunction occurs in absence of significant coronary artery stenosis in patients with DM.46)47) Although definite pathophysiological mechanisms of DM in HFpEF have yet to be elucidated, several common pathological mechanisms have been suggested including microvascular dysfunction, metabolic derangements and systemic inflammation, sodium retention, and impaired skeletal muscle function.45) Insulin resistance in DM leads to increase free fatty acid utilization by cardiac myocytes, which may lead to mitochondrial dysfunction, production of toxic lipid intermediates, and increased reactive oxygen species.45) Hyperglycemia-induced advanced glycation end products result in microvascular dysfunction and decline nitric oxide availability.48) In addition, hyperglycemia causes up-regulation of the sodium-glucose cotransporter-2 (SGLT-2) leading to increased proximal renal sodium absorption, volume expansion, and decreased of diuretics response.49) As a result, many previous studies have demonstrated LV diastolic dysfunction and impaired LV longitudinal functional reserve in patients with DM.50)51) Furthermore, impaired LV longitudinal functional reserve in patients with DM without overt heart disease provided incremental prognostic information for composite of death and HF hospitalization.28) Recently, as expectations for the effect of SGLT-2 inhibitors on improving HF outcome have increased, interests in DM as a risk factor of HFpEF have been amplified. SGLT-2 inhibitors have demonstrated convincing reductions in the incidence and risks of HF in patients with DM.52)53)54)55) Now, studies are underway to prove the beneficial effects of SGLT-2 inhibitors in overt HF patients with or without DM.
Go to :
OBESITY AND OBSTRUCTIVE SLEEP APNEA
Obesity is a major risk factor of HF and also one of the most common comorbidities in patients with HFpEF.56) Obesity has several harmful effects in aspects of HF, mediated by changes in volume status, cardiac loading, energy substrate utilization, tissue metabolism and systemic inflammation that are believed to promote disease progression.57)58) Typically, obese patients with HFpEF have increased plasma volume with greater biventricular filling pressure, typical myocardial remodeling characterized by increased LV dimensions and mass.57)58) Interestingly, obesity is more important risk factor of occurrence of HFpEF in women than in men.59) Our previous study also demonstrated overweight women had exercise intolerance than lean women through displaying impaired arterial compliance during exercise.37) Because obesity is possible to be treated by weight reduction and physical activity, many studies have demonstrated significant improvement in cardiac structure and function after bariatric surgery, dietary or exercise intervention.60) In obese patients, obstructive sleep apnea (OSA) is frequently combined and OSA might deteriorate LV diastolic dysfunction and longitudinal systolic function by exposing to episodic hypoxemia, nocturnal sympathetic nervous system activation, elevated BP, oxidative stress and inflammation.61)62) In our recent randomized, sham controlled clinical trial, continuous positive airway pressure treatment for 3 months in patients with severe OSA improved LV diastolic function more than sham treatment, and was accompanied by improvements in arterial stiffness and ventricular-vascular coupling.63) Moreover, we additionally proved that LV mechanical function assessed by speckle-tracking echocardiography and right ventricular fractional area change were significantly improved by continuous positive airway pressure.64) Hence, obesity and OSA are modifiable risk factors, so it is necessary to actively evaluate and treat them before myocardial structural and functional changes are too advanced.
Go to :
CONCLUSION
HFpEF is a heterogeneous clinical syndrome and the single greatest unmet need in cardiovascular medicine. We hope that HFpEF will become a solved disease entity with lots of evidence in the future through more scientific phenotype classification in the era of precision medicine, improved diagnostic imaging even in early stage of disease, applying appropriate drugs and intervention focusing each pathophysiologic mechanism.
Go to :
 XML Download
XML Download